High local levels, low systemic toxicity | PMMA vs calcium sulfate | biphasic elution | heat-stable antibiotics only
- PMMA is the non-absorbable gold standard but 90-95% of antibiotic stays permanently trapped in the matrix - only ~5-10% ever elutes
- Only heat-stable antibiotics (gentamicin, tobramycin, vancomycin) survive PMMA polymerization (exotherm 80-110°C; most denature above 60°C)
- Calcium sulfate is absorbable and osteoconductive, resorbing in 6-12 weeks to allow bone replacement - but can cause sterile drainage/hypercalcaemia
- Hand mixing raises cement porosity and increases elution versus vacuum mixing
- Prophylactic antibiotic cement in primary arthroplasty reduces infection rates (Norwegian Registry evidence)
- “Elution is biphasic: a high initial burst then a low sustained tail; local levels can reach 200-1000× MIC near the carrier
- “Two-stage revision arthroplasty uses a gentamicin/vancomycin PMMA spacer to deliver antibiotic and maintain the joint space
- “Antibiotic beads manage osteomyelitis dead space; absorbable carriers avoid a second removal operation
- “Gentamicin-PMMA was introduced by Buchholz in the 1970s - a classic viva fact
Local Antibiotic Delivery Systems
High-Yield Testing Areas:
- PMMA elution kinetics and factors affecting release
- Heat-stable antibiotics for cement mixing
- Calcium sulfate resorption timeline and complications
- Evidence for prophylactic antibiotic cement in arthroplasty
- Contraindications and complications of local delivery systems


Overview
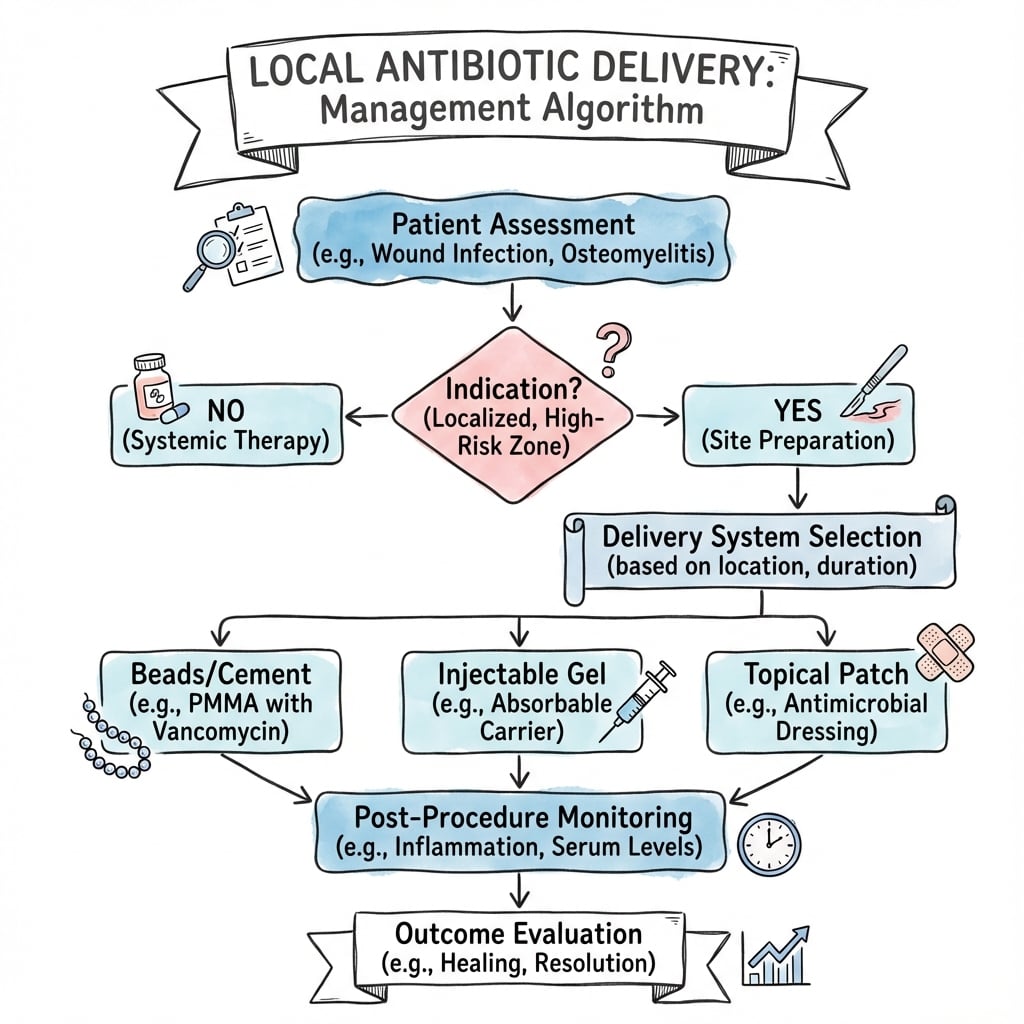
Local antibiotic delivery systems provide targeted antimicrobial therapy directly at the site of infection or contamination, achieving drug concentrations far exceeding those possible with systemic administration while minimizing systemic toxicity. These systems are fundamental to modern management of orthopaedic infections, particularly in the context of prosthetic joint infections, osteomyelitis, and open fracture contamination.
The principle relies on sustained release of antibiotics from carrier materials that can be either permanent (PMMA) or absorbable (calcium sulfate, bioabsorbable polymers). Local concentrations can reach 200-1000 times the minimum inhibitory concentration (MIC) of susceptible organisms, providing potent antibacterial activity even in the relatively avascular environment of infected bone and soft tissue. Understanding the pharmacokinetics, carrier properties, and clinical evidence for these systems is essential for orthopaedic fellowship candidates.
Historical Development
- 1970s: Introduction of gentamicin-loaded PMMA bone cement by Buchholz
- 1980s: Development of antibiotic-impregnated beads for osteomyelitis
- 1990s: Calcium sulfate pellets as absorbable antibiotic carriers
- 2000s: Bioabsorbable polymer systems and commercial products
- Current era: Combination carriers and growth factor-loaded systems
Mechanism and Properties
Polymerization Process
PMMA bone cement undergoes exothermic polymerization reaching temperatures of 80-110°C during the liquid-powder mixing phase. This heat generation limits the antibiotics that can be incorporated, as many are denatured at temperatures greater than 60°C. The curing process creates a dense polymer matrix with antibiotics distributed throughout.
Heat-Stable Antibiotics:
- Gentamicin (most common, stable to 110°C)
- Tobramycin (stable, similar profile to gentamicin)
- Vancomycin (stable to 100°C)
- Clindamycin (moderately stable)
- Erythromycin (moderately stable)
Heat-Labile Antibiotics (NOT suitable):
- Cephalosporins (denature above 60°C)
- Penicillins (unstable)
- Fluoroquinolones (variable stability)
Elution Kinetics
PMMA exhibits a biphasic release pattern:
- Initial burst phase (0-24 hours): Rapid release of surface antibiotics, achieving peak local concentrations
- Sustained low-level release (days to weeks): Slow diffusion from deeper layers through microporosity
The majority (90-95%) of incorporated antibiotic remains permanently bound within the cement matrix and never elutes. This has implications for potential antibiotic resistance development and long-term biofilm formation on cement surfaces.
Factors Affecting Elution
Increased Antibiotic Release:
- Higher antibiotic loading (up to 10% by weight)
- Hand-mixed cement (more porous than vacuum-mixed)
- Addition of glycine or glucose (increases porosity)
- Smaller bead surface area to volume ratio
- Lower cement viscosity
Decreased Antibiotic Release:
- Vacuum mixing (reduces porosity)
- High-viscosity cement formulations
- Thick cement mantles
- Smooth cement surfaces
The standard infected-arthroplasty spacer is loaded with both vancomycin and an aminoglycoside (tobramycin/gentamicin) for two distinct, examinable reasons:
- Complementary spectrum: vancomycin covers the gram-positive organisms that dominate PJI (Staphylococci, including MRSA and coagulase-negative), while the aminoglycoside adds gram-negative cover - together they empirically span the likely pathogens while awaiting/optimising cultures.
- Synergistic elution ("passive opportunistic release"): adding a second antibiotic increases the porosity of the cement as each drug elutes, so the two together elute MORE of each other than either does alone - dual loading raises the local concentration and prolongs release beyond simple addition.
This is on top of the core local-delivery advantage: PMMA achieves local concentrations far above the systemic MIC (orders of magnitude higher than safe IV levels) right at the avascular, biofilm-laden surface that systemic antibiotics struggle to reach, while keeping serum levels low.
Caveat: high-dose dual loading weakens the cement (especially vancomycin) and raises systemic-absorption/AKI risk - which is why high-dose loading is for non-load-bearing spacers/beads in established infection, not for prophylactic primary cement.
Exam point: dual vancomycin + aminoglycoside loading gives gram-positive + gram-negative cover AND synergistic (porosity-driven) elution, delivering supra-MIC local levels at the biofilm surface - balanced against reduced cement strength and systemic toxicity at high doses.
Overview
Key Concepts
- Achieve 100-1000× higher local concentrations than systemic
- Minimize systemic toxicity
- Penetrate avascular infected tissue
- Non-absorbable: PMMA cement
- Absorbable: Calcium sulfate, polymers
- Local
- 100-1000× MIC
- Systemic
- 2-10× MIC
- Local
- Minimal
- Systemic
- Dose-limiting
- Local
- Direct
- Systemic
- Vascular dependent
Contraindications
Absolute Contraindications
PMMA Beads/Spacers:
- Known allergy to antibiotic being loaded
- Inadequate soft tissue coverage (exposed cement)
- Severe renal impairment with high-dose aminoglycoside loading
Calcium Sulfate:
- Known hypersensitivity to calcium sulfate
- Areas requiring immediate structural support (load-bearing)
- Severe renal impairment (risk of hypercalcemia with large volumes)
Relative Contraindications
PMMA:
- Organism resistant to available heat-stable antibiotics
- Need for MRI imaging (metal beads on wire)
- Patient unable to tolerate second surgery for removal
Calcium Sulfate:
- High-risk wounds (poor soft tissue coverage, questionable healing)
- Large cavitary defects requiring structural support
- Concern for prolonged wound drainage (cosmetic areas)
Bioabsorbable Polymers:
- Cost constraints (limited insurance coverage)
- Uncertain local environment (ischemic tissue, poor vascularity)
Anatomy
Tissue Considerations
- Cortical bone: Poor penetration (avascular)
- Cancellous bone: Better drug distribution
- Dead space: Primary target for local delivery
- Biofilm formation on implants
- Sequestra create avascular zones
- pH changes reduce antibiotic efficacy
- Challenge
- Avascular
- Solution
- Direct carrier placement
- Challenge
- Protected bacteria
- Solution
- High concentration
- Challenge
- No blood supply
- Solution
- Debride + local delivery
Classification
Carrier Classification
- Non-absorbable: PMMA (permanent, removal needed)
- Absorbable: Calcium sulfate, polymers (no removal)
- Passive diffusion: PMMA, calcium sulfate
- Controlled release: Bioabsorbable polymers
- Example
- PMMA beads/spacers
- Resorption
- Permanent
- Example
- Calcium sulfate
- Resorption
- 4-8 weeks
- Example
- PLGA/collagen
- Resorption
- Weeks-months
Investigations
Pre-Treatment Assessment
- Culture and sensitivity (guides antibiotic choice)
- Tissue biopsy preferred over swab
- Extended cultures for slow-growing organisms
- CRP and ESR (baseline, monitor response)
- Renal function (aminoglycoside toxicity risk)
- WBC (often normal in chronic infection)
- Purpose
- Guide antibiotic selection
- Timing
- Before antibiotics
- Purpose
- Monitor response
- Timing
- Baseline and serial
- Purpose
- Aminoglycoside safety
- Timing
- Pre-op and during treatment
Differential Diagnosis of Persistent Wound Drainage After Carrier Placement
A draining wound after local antibiotic delivery is a common viva scenario. The key decision is distinguishing expected, self-limiting calcium-sulfate seepage from true ongoing infection that mandates return to theatre.
- Typical Features
- Clear/serous, peaks early, settles as pellets resorb (weeks)
- Cultures
- Negative (sterile)
- Management
- Conservative wound care; reassure; avoid overpacking next time
- Typical Features
- Serous collection, no systemic upset, normal/falling CRP
- Cultures
- Negative
- Management
- Observe; aspirate only if symptomatic
- Typical Features
- Purulent, rising CRP/ESR, pain, systemic signs, sinus tract
- Cultures
- Positive (organism)
- Management
- Debridement, repeat sampling, revise antibiotic strategy
- Typical Features
- Bloody, early, may be tense
- Cultures
- Negative unless secondarily infected
- Management
- Evacuate if large/tense; correct coagulopathy
- Typical Features
- Sterile drainage with rapid-degrading PGA
- Cultures
- Negative
- Management
- Usually self-limiting; debride if abscess forms
Key discriminator: Calcium-sulfate drainage is clear/serous, sterile, and time-limited to the resorption phase. Purulent drainage, rising inflammatory markers, or a positive culture point to true infection and warrant return to theatre, not reassurance.
Management
Treatment Principles
- Need for removal vs absorbable
- Load-bearing requirements
- Organism sensitivity (heat-stable antibiotic available?)
- PJI: High-dose PMMA spacer (two-stage)
- Osteomyelitis: Calcium sulfate or PMMA beads
- Prophylaxis: Low-dose PMMA in cement
- Carrier
- PMMA spacer
- Loading
- Vanc + gent high-dose
- Carrier
- Calcium sulfate
- Loading
- Culture-specific
- Carrier
- Antibiotic cement
- Loading
- Low-dose gent
Surgical Technique
Cement Preparation
- Add antibiotic powder to polymer powder
- Mix thoroughly before adding monomer
- Hand-mix (more porous = better elution)
- Roll cement during doughy phase
- Thread beads on surgical wire
- Standard: 4-6 beads per string
- Mould around femoral component
- Articulating spacer preferred
- Ensure adequate antibiotic distribution
- Key Point
- Before monomer
- Rationale
- Even distribution
- Key Point
- Hand preferred
- Rationale
- More porous, better elution
- Key Point
- 6-8mm diameter
- Rationale
- Optimal surface area
Complications
PMMA-Related
Mechanical Failure:
- Spacer fracture (5-15% with high antibiotic loading)
- Reduced compressive strength with greater than 10% loading
- More common with vancomycin than gentamicin
Antibiotic Resistance:
- Theoretical concern with prophylactic cement use
- Sub-inhibitory levels after initial burst phase
- Registry data has not shown increased resistance to date
- Biofilm formation on retained cement surfaces
Systemic Toxicity:
- Rare with standard loading
- Reported cases of acute kidney injury with high-dose spacers
- More common with renal impairment and multiple spacers
Calcium Sulfate-Related
Wound Drainage (most common):
- Incidence 15-30%
- Usually sterile, culture-negative
- Can persist for 2-4 weeks
- Rarely requires reoperation
Inflammatory Reaction:
- Local acidosis from calcium sulfate breakdown
- Seroma formation
- Usually self-limiting
Rapid Resorption:
- Can create transient dead space
- May require bone grafting later if healing inadequate
Polymer-Related
Foreign Body Reaction:
- Inflammatory response to degradation products
- Sterile seroma or abscess formation
- More common with rapid-degrading polymers (PGA)
Unpredictable Release:
- Variable kinetics based on local pH, vascularity
- Acidic degradation products may affect release rate
Renal Impairment: High-dose antibiotic spacers (particularly aminoglycosides) can cause systemic absorption and nephrotoxicity in patients with pre-existing renal dysfunction. A systematic review of two-stage revision reported an average acute kidney injury incidence of 4.8% (Luu 2013, PMID 23578491). Monitor renal function and antibiotic levels in high-risk patients with spacers in situ.
Postoperative Care
Monitoring
- Serial inflammatory markers (CRP, ESR)
- Wound inspection (drainage, healing)
- Renal function if aminoglycosides used
- Plan for bead removal at 2-4 weeks
- Expect wound drainage (15-30%)
- Usually sterile, self-limiting
- Monitor for hypercalcemia (rare)
- Frequency
- Weekly
- Concern
- Should decrease
- Frequency
- Daily
- Concern
- Drainage, healing
- Frequency
- Weekly if aminoglycoside
- Concern
- Nephrotoxicity
Outcomes
Success Rates
- Infection eradication: 85-95%
- Functional success: 70-80%
- Reinfection rate: 5-15%
- Calcium sulfate: 75-90% eradication
- PMMA beads: 80-90% eradication
- Comparable outcomes, but calcium sulfate avoids removal surgery
- Success Rate
- 85-95%
- Notes
- Gold standard
- Success Rate
- 75-90%
- Notes
- Debridement critical
- Success Rate
- 0.5-1% ARR
- Notes
- Registry data
Clinical Applications of PMMA
Two-Stage Revision Arthroplasty
The most established use of antibiotic-loaded PMMA is in articulating spacers for infected total joint arthroplasty:
Standard Protocol:
- Stage 1: Implant removal, debridement, placement of antibiotic spacer
- Interval period: 6-12 weeks of spacer in situ with systemic antibiotics
- Stage 2: Spacer removal, reimplantation of new prosthesis
Antibiotic Loading:
- Standard: 1-2g vancomycin + 2.4-4.8g tobramycin per 40g cement
- High-dose: Up to 10% antibiotic by weight of cement
- Custom loading based on organism sensitivity
Biomechanical Considerations:
- Antibiotic loading greater than 10% significantly reduces compressive strength
- Vancomycin more than tobramycin reduces mechanical properties
- Static spacers require less structural integrity than articulating spacers
For an infected arthroplasty two-stage revision, the spacer type is an examinable choice:
- Articulating spacer (mobile, allows joint motion between stages): preserves range of motion, soft-tissue/capsular length and quadriceps function, eases the eventual reimplantation, and gives better interim function and final outcomes in most patients. The trade-off is a more complex construct that can fracture, dislocate or wear, and it needs reasonable bone stock and a competent extensor mechanism/soft-tissue envelope.
- Static (block) spacer (immobilises the joint): chosen for severe bone loss, an incompetent extensor mechanism or collateral ligaments, a compromised soft-tissue envelope, or where stability is paramount; it sacrifices motion and causes more arthrofibrosis/quadriceps shortening, making reimplantation harder, but it is mechanically safer in a deficient knee.
The unifying principle: articulating by default for function; static when the bone/soft tissue cannot support a mobile spacer or maximal stability is needed.
Exam point: pick an articulating spacer for better motion/function and easier reimplantation when bone stock and the extensor mechanism allow; reserve a static spacer for severe bone loss, extensor-mechanism/soft-tissue compromise, or when stability trumps motion.
Prophylactic Antibiotic Cement
Use of low-dose gentamicin cement (0.5-1g per 40g) in primary arthroplasty remains controversial:
Arguments FOR:
- Reduced revision for infection in cemented THA on meta-analysis (RR 0.66, Farhan-Alanie 2021)
- Combined systemic + cement antibiotics gave the lowest infection revision rate in the Norwegian Register (Espehaug/Engesaeter 1997)
- Cost-effective in high-risk populations
- Minimal mechanical property compromise at low doses
Arguments AGAINST:
- No significant benefit for primary TKA in the same meta-analysis (RR 0.92, not significant)
- Concern for antibiotic resistance
- Low absolute risk reduction in low-risk patients
- Added cost; some systematic reviews argue plain cement saves health-system expense
Current Recommendations:
- Strongest evidence is for cemented THA; the TKA question is genuinely contested
- Reserve for higher-risk patients (diabetes, immunosuppression, prior infection, revision) where evidence is least ambiguous
- Combine with systemic prophylaxis rather than relying on either alone
Antibiotic Beads and Chains
Beads on surgical wire provide:
- Dead space management in osteomyelitis
- Local antibiotic delivery at fracture sites
- Temporary wound coverage with antibiotic elution
Technique:
- Standard: 4-6 beads per surgical wire
- Removal required (second procedure) at 2-4 weeks
- Can be used with negative pressure wound therapy
- PMMA Cement
- Non-absorbable (permanent)
- Calcium Sulfate
- 4-8 weeks complete
- Bioabsorbable Polymer
- Variable (weeks to months)
- PMMA Cement
- Yes (beads/spacers)
- Calcium Sulfate
- No
- Bioabsorbable Polymer
- No
- PMMA Cement
- 5-10% total content
- Calcium Sulfate
- 90-100% total content
- Bioabsorbable Polymer
- 70-95% controlled release
- PMMA Cement
- Days to weeks (low level)
- Calcium Sulfate
- 2-6 weeks
- Bioabsorbable Polymer
- Weeks to months (programmable)
- PMMA Cement
- High (load-bearing)
- Calcium Sulfate
- Low (dead space only)
- Bioabsorbable Polymer
- Variable
- PMMA Cement
- None
- Calcium Sulfate
- Yes (resorbs to bone)
- Bioabsorbable Polymer
- Variable
- PMMA Cement
- Yes (80-110°C)
- Calcium Sulfate
- No (cold-mixed)
- Bioabsorbable Polymer
- No (cold-mixed)
- PMMA Cement
- Low to moderate
- Calcium Sulfate
- Moderate to high
- Bioabsorbable Polymer
- High
- PMMA Cement
- Yes (multiple products)
- Calcium Sulfate
- Yes (Osteoset)
- Bioabsorbable Polymer
- Limited (investigational)
Material Properties
Calcium sulfate (medical-grade plaster of Paris) has been used in orthopaedics since the 1890s for bone defect filling. Modern formulations are specifically designed for antibiotic delivery with controlled resorption rates.
Composition and Setting
- Chemical formula: CaSO₄·½H₂O (hemihydrate) + H₂O → CaSO₄·2H₂O (dihydrate)
- Setting reaction: Exothermic but low temperature (37-42°C)
- Setting time: 5-15 minutes depending on formulation
- Cold-setting: Allows use of heat-labile antibiotics
Biological Properties
Advantages:
- Osteoconductive scaffold for bone ingrowth
- Complete resorption with replacement by host bone
- Provides calcium and sulfate ions (potential local acidosis)
- No second surgery for removal
Disadvantages:
- Rapid resorption can create transient dead space
- Wound drainage common (up to 30% of patients)
- Local acidosis may inhibit osteogenesis
- Limited mechanical strength (non-load-bearing only)
Resorption Timeline
The rapid resorption provides near-complete antibiotic elution but can create temporary void space before new bone formation. This is particularly relevant in load-bearing areas where mechanical support is required during healing.
Clinical Applications
Osteomyelitis Management
Calcium sulfate beads or pellets are placed into debrided osteomyelitis cavities:
Advantages:
- Single-stage procedure (no removal needed)
- High local antibiotic concentrations
- Osteoconductive scaffold for bone healing
- Any antibiotic can be incorporated (cold-mixed)
Technique:
- Thorough surgical debridement first
- Mix antibiotic powder directly into calcium sulfate
- Typical loading: 1-2g antibiotic per 10cc calcium sulfate
- Pack into dead space, avoid overpacking
- Consider closed suction drainage
Open Fracture Management
Use in contaminated open fractures remains controversial:
Potential Benefits:
- Local antibiotic delivery at contaminated fracture site
- Reduced infection rates in some studies
- Dead space management
Concerns:
- Wound drainage complications
- Cost
- Limited high-quality RCT evidence
- May interfere with fracture healing in some cases
Complications
Wound Drainage (most common):
- Incidence: 15-30% of cases
- Usually sterile, culture-negative
- Management: Local wound care, rarely requires reoperation
- Prevention: Avoid overpacking, consider drain placement
Local Inflammatory Reaction:
- Calcium sulfate resorption creates acidic pH
- Can cause seroma formation
- Usually self-limiting
Hypercalcemia:
- Rare, reported with very large volumes (greater than 100cc)
- Usually transient and asymptomatic
- Monitor in patients with renal impairment
Polymer Types and Mechanisms
Polylactic and Polyglycolic Acid (PLA/PGA)
These synthetic polymers undergo hydrolytic degradation:
Chemical Properties:
- PLLA (poly-L-lactic acid): Slow degradation (12-24 months)
- PLGA (poly-lactic-co-glycolic acid): Faster degradation (6-12 months)
- PGA (polyglycolic acid): Rapid degradation (1-3 months)
- Degradation to lactic and glycolic acid (metabolized via Krebs cycle)
Antibiotic Release Kinetics:
- Programmable release rates based on polymer composition
- Controlled degradation allows sustained therapeutic levels
- Can achieve weeks to months of antibiotic elution
- Release kinetics follow polymer degradation profile
Collagen-Based Carriers
Resorbable collagen sponges or fleece impregnated with antibiotics:
Commercial Products:
- Collatamp G (gentamicin-collagen sponge)
- Septocoll (gentamicin-collagen fleece)
Properties:
- Rapid resorption (4-12 weeks)
- Hemostatic properties
- Conformable to wound beds
- Limited mechanical strength
Chitosan and Natural Polymers
Emerging carriers from natural sources:
- Chitosan: Derived from crustacean shells, antimicrobial properties
- Hyaluronic acid: Viscosupplement carrier for antibiotics
- Fibrin glue: Carrier for antibiotics in wound beds
Antibiotic Characteristics
Ideal Properties for Local Delivery
Essential Characteristics:
- Broad-spectrum activity against common orthopaedic pathogens
- Bactericidal (not just bacteriostatic)
- Heat-stable (if using PMMA)
- Powder formulation available
- Minimal local tissue toxicity
- Low systemic absorption (minimal toxicity)
Common Antibiotic Choices
Gentamicin (most common):
- Broad gram-negative coverage
- Good Staphylococcus activity
- Heat-stable to 110°C
- Well-studied elution profile
- Powder formulation readily available
- Minimal local tissue toxicity
Vancomycin:
- Excellent MRSA coverage
- Heat-stable to 100°C
- Often combined with gentamicin (synergistic)
- Higher cost than gentamicin
- Can reduce cement mechanical properties more than gentamicin
Tobramycin:
- Similar spectrum to gentamicin
- Slightly better Pseudomonas coverage
- Heat-stable
- Used in commercial antibiotic cement products
Other Agents:
- Clindamycin: Anaerobic coverage
- Daptomycin: MRSA, VRE (heat-labile, calcium sulfate only)
- Rifampin: Biofilm penetration (never alone, resistance)
Gentamicin and tobramycin are first-line choices for PMMA cement due to heat stability, broad spectrum, and extensive clinical experience. Combine with vancomycin for MRSA coverage in infected arthroplasty.
Cephalosporins and penicillins denature during PMMA polymerization. They can only be used with cold-setting carriers like calcium sulfate or bioabsorbable polymers.
Dual antibiotic loading (vancomycin + aminoglycoside) provides synergistic activity and broader spectrum. Loading up to 10% total antibiotic by weight of cement is safe for mechanical properties.
Loading Dose Considerations
Prophylactic Loading (Primary Arthroplasty)
Low-dose gentamicin:
- Standard: 0.5-1g per 40g cement packet
- Minimal mechanical property reduction
- Registry evidence for infection reduction
- Cost-effective in high-risk populations
Therapeutic Loading (Infected Arthroplasty)
High-dose combinations:
- Vancomycin 1-2g + Tobramycin 2.4-4.8g per 40g cement
- Can go up to 10% total antibiotic by weight
- Used in articulating spacers for two-stage revision
- Higher doses increase elution but reduce mechanical strength
Osteomyelitis Loading (Calcium Sulfate)
Concentrated local therapy:
- Typical: 1-2g antibiotic per 10cc calcium sulfate
- No mechanical property concerns (non-load-bearing use)
- Culture-specific antibiotic selection when possible
- Can use heat-labile agents (cold-mixed)
Guidelines, Registries & Global Practice
Global Epidemiology and Practice Variation
Periprosthetic joint infection complicates roughly 1-2% of primary and up to 4-15% of revision arthroplasties worldwide, and is a leading cause of revision in every major registry. Local antibiotic delivery is near-universal in two-stage revision, but prophylactic antibiotic-loaded cement (ALBC) in primary arthroplasty varies enormously by region: it is routine across much of Europe (driven by Scandinavian register data) yet historically optional in parts of North America, where many surgeons reserved it for high-risk cases. The strongest registry-derived signal is in cemented THA; the primary TKA evidence is genuinely contested.
- Position
- Two-stage revision with antibiotic spacer is a standard option for chronic PJI; surgeon-directed local antibiotics
- Evidence Level
- Consensus / moderate
- Position
- Systemic prophylaxis mandatory; ALBC not mandated routinely - clinician judgement
- Evidence Level
- Low-moderate
- Position
- Early systemic antibiotics; local antibiotics (e.g. beads/gentamicin) as adjunct after debridement
- Evidence Level
- Consensus
- Position
- Debridement plus local antibiotic carrier (PMMA or bioabsorbable) for dead space
- Evidence Level
- Consensus
- Position
- Routine ALBC in cemented arthroplasty widely endorsed
- Evidence Level
- Register-based
Registry Evidence
- Norwegian Arthroplasty Register: combined systemic + antibiotic cement gave the lowest revision-for-infection rate; cement without antibiotic increased infection risk that ALBC neutralised (Espehaug/Engesaeter 1997; Engesaeter 2006).
- Pooled register/meta-analysis (Farhan-Alanie 2021): ALBC protective for revision-for-PJI in THA (RR 0.66) but not significant in TKA.
- AOANJRR (Australia): tracks cement type and revision for infection and is used to inform local ALBC practice, particularly in cemented fixation and higher-risk patients.
Commonly Used Commercial Products
These antibiotic-loaded cements and resorbable carriers are available internationally (brand availability varies by region):
- PMMA (factory-loaded): Palacos R+G (gentamicin) and Simplex with Tobramycin
- Calcium sulfate (surgeon-loaded): Osteoset and Stimulan, which accept any antibiotic mixed intraoperatively
- Type
- PMMA
- Antibiotic
- Gentamicin 0.5g
- Type
- PMMA
- Antibiotic
- Tobramycin 1g
- Type
- Calcium sulfate
- Antibiotic
- Surgeon-loaded (any antibiotic)
Examiner Favorite: "What factors increase antibiotic elution from PMMA cement?" Answer systematically: Higher antibiotic loading, hand-mixing (vs vacuum), additives like glycine, smaller bead size (higher surface area), and lower cement viscosity. Then contrast with calcium sulfate which releases 90-100% regardless of these factors due to complete resorption.
MCQ Practice Points
Q: What is the most commonly used antibiotic in PMMA bone cement for arthroplasty infection prophylaxis?
A: Gentamicin (tobramycin in some regions). Commercial antibiotic-loaded cements contain 0.5-1g gentamicin per 40g cement. This provides local concentrations 100-1000x higher than MIC for staphylococci while maintaining low systemic levels. For treatment of established infection, higher doses (3-4g per 40g cement) are hand-mixed. Vancomycin 1-2g is added for MRSA coverage.
Q: What are the advantages of local antibiotic delivery compared to systemic administration?
A: (1) Local concentrations 100-1000x higher than achievable systemically, (2) Minimal systemic absorption and toxicity, (3) Effective in avascular areas where systemic antibiotics cannot penetrate, (4) Sustained release over weeks. Limitations: only heat-stable antibiotics survive cement polymerization (gentamicin, vancomycin, tobramycin - NOT beta-lactams), requires surgical placement.
Q: What is the recommended antibiotic-loaded cement spacer regimen for a two-stage revision of an infected total knee arthroplasty?
A: High-dose antibiotic cement: vancomycin 3-4g + gentamicin 3-4g per 40g PMMA cement. Articulating spacer preferred over static spacer (maintains soft tissue tension, easier revision). Cement spacer remains in situ for 6-12 weeks while systemic antibiotics administered. Consider antibiotic holiday (2-6 weeks) before reimplantation to confirm infection clearance.
Q: What are the properties of an ideal local antibiotic delivery system?
A: (1) Heat-stable (survives cement polymerization at 70-100°C), (2) Water-soluble (for elution from cement), (3) Broad-spectrum coverage, (4) Bactericidal, (5) Low allergenicity, (6) Minimal systemic absorption, (7) Prolonged elution kinetics. Gentamicin, tobramycin, and vancomycin meet these criteria. Beta-lactams are heat-labile and not suitable.
Q: What is the role of antibiotic-impregnated calcium sulfate beads in osteomyelitis management?
A: Biodegradable alternative to PMMA beads that does not require removal surgery. Calcium sulfate resorbs over 4-12 weeks, releasing antibiotics and being replaced by bone. Can deliver vancomycin, gentamicin, or tobramycin. Useful for: dead space management, osteomyelitis debridement, open fracture void filling. Complication: transient hypercalcemia, prolonged wound drainage during resorption.
At a Glance
Local antibiotic delivery systems provide targeted antimicrobial therapy achieving concentrations 10-100× MIC while minimizing systemic toxicity. PMMA bone cement (non-absorbable gold standard) exhibits biphasic elution with 80% released in 24 hours but 90-95% permanently trapped in the matrix; only heat-stable antibiotics (gentamicin, tobramycin, vancomycin) survive polymerization. Calcium sulfate (absorbable, osteoconductive) resorbs in 6-12 weeks allowing bone replacement. Hand mixing increases cement porosity and elution versus vacuum mixing. Clinical applications include gentamicin-PMMA spacers for two-stage revision arthroplasty, antibiotic beads for open fractures, and prophylactic antibiotic cement in primary TJA which reduces infection rates (Norwegian Registry evidence).
GENT-VTCHeat-Stable PMMA Antibiotics
Hook:GENT-VTC for heat-stable antibiotic cement options
COLDBONECalcium Sulfate Properties
Hook:COLD BONE for calcium sulfate properties vs PMMA
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with diabetes presents 14 months after primary total knee arthroplasty with chronic sinus drainage and pain. Aspiration grows MRSA. You plan a two-stage revision. Discuss your antibiotic spacer strategy.”
“You are managing chronic osteomyelitis of the tibia following an open fracture. After debridement, you have a 50cc bone defect. The organism is pan-sensitive Staphylococcus aureus. Discuss local antibiotic delivery options.”
“A colleague asks whether they should routinely use antibiotic-loaded bone cement (ALBC) in all primary cemented total knee and hip arthroplasties. Discuss the evidence.”
PMMA Antibiotic Cement
Calcium Sulfate Carriers
Bioabsorbable Polymers
Evidence-Based Practice
Complications to Mention
Clinical Applications and Evidence
Current Uses
Applications (evidence mixed):
- Gentamicin-collagen sponges: widely available but the pivotal colorectal RCT (Bennett-Guerrero, NEJM 2010) found no benefit and increased SSI; orthopaedic/spine data are lower quality and inconsistent
- Sternal wound infection prophylaxis in cardiac surgery (also studied with conflicting results)
- High-risk orthopaedic wounds (carrier benefit must be demonstrated per indication, not assumed)
Investigational Applications:
- Fracture fixation with antibiotic-coated implants
- Antibiotic-loaded bone graft substitutes
- Combined growth factor and antibiotic delivery
Limitations
Technical Challenges:
- Manufacturing complexity and cost
- Regulatory approval barriers (limited FDA-approved products)
- Variable release kinetics based on local environment
- Potential for local inflammatory response to degradation products
Clinical Barriers:
- High cost compared to PMMA or calcium sulfate
- Limited long-term outcome data
- Unclear advantage over established systems in most applications
Evidence Base
Norwegian Register: Systemic Plus Antibiotic Cement Lowers Revision for Infection
- Combined systemic + antibiotic cement gave the lowest revision rate for infection
- Systemic antibiotics alone: 4.3x higher revision rate for infection (95% CI 1.7-11.0)
- Antibiotic in cement only: 6.3x higher (95% CI 1.6-25.0)
- No antibiotics: 11.5x higher (95% CI 2.1-63.0)
Antibiotic-Loaded Cement and Revision for Infection: Hip vs Knee Differ
- THA: ALBC protective against revision for PJI (RR 0.66, 95% CI 0.56-0.77)
- THA: no significant difference in all-cause revision (RR 0.62, 95% CI 0.35-1.09)
- TKA: no significant difference for PJI (RR 0.92, 95% CI 0.59-1.45)
- TKA: no significant difference for all-cause revision (RR 0.73, 95% CI 0.53-1.02)
Calcium Sulfate vs PMMA Beads in Chronic Osteomyelitis (RCT)
- Infection eradicated in 86% (12/14) in both calcium sulfate and PMMA groups
- Fewer reoperations with calcium sulfate (7 vs 15, p=0.04)
- Comparable union rates (7/8 vs 6/8 nonunions)
- Calcium sulfate avoids a second procedure for bead removal
Calcium Sulfate Bone Substitute in Infected Long-Bone Defects
- Infection eradicated in 92% (23/25)
- Pellets radiographically resorbed at a mean of 2.7 months
- Isolated bony defects healed in all 9 patients without further treatment
- 8 patients developed sterile draining sinuses that healed on resorption
Gentamicin-Collagen Sponge Does NOT Prevent SSI (and may worsen it)
- SSI higher in the sponge group (30.0%) than control (20.9%), p=0.01
- Superficial SSI 20.3% vs 13.6% (p=0.03)
- More wound-related ER/surgeon visits in the sponge group (19.7% vs 11.0%)
- No reduction in deep SSI
Acute Kidney Injury Risk From Antibiotic Spacers
- Pooled infection control rate 91%
- Average acute kidney injury incidence 4.8%
- Average infection persistence/recurrence 11%
- Marked heterogeneity in spacer antibiotic dosing across studies
Vacuum vs Hand Mixing and Gentamicin Elution
- Vacuum mixing reduced porosity but only minimally reduced total gentamicin release
- Hand-added antibiotic released less than industrially pre-loaded cement
- Release varied substantially between commercial brands
- Porosity is one of several determinants of elution, not the sole driver
Evidence Base
Key Studies
- First described gentamicin-loaded PMMA bone cement
- Foundation of all modern local antibiotic delivery
- Systemic + antibiotic cement gave lowest revision for infection
- Each lesser regimen had progressively higher revision rates
- Tobramycin calcium sulfate: 92% eradication (2002 cohort)
- RCT (2010): equivalent to PMMA beads but fewer reoperations
- Finding
- Systemic + ALBC lowest infection revision
- Level
- Level 2
- Finding
- ALBC protective in THA, not TKA
- Level
- Level 1
- Finding
- CaSO4 = PMMA, fewer reops
- Level
- Level 2
- Finding
- Gent-collagen sponge increased SSI
- Level
- Level 1
Cross-References
Related Basic Science Topics:
- PMMA Bone Cement (polymerization, mechanical properties, thermal effects)
- Calcium Phosphate Cements (alternative osteoconductive carriers)
- Bioabsorbable Materials (polymer degradation kinetics, tissue response)
- Common Pathogens in Orthopaedics (organism-specific antibiotic selection)
- Osteomyelitis Pathophysiology (infection biology, antibiotic penetration)
Related Clinical Topics:
- Periprosthetic Joint Infection (two-stage revision, spacer technique)
- Pediatric Acute Osteomyelitis (dead space management, antibiotic delivery)
- Open Fracture Management (local antibiotic prophylaxis)
- Surgical Site Infection Prevention (prophylactic antibiotic strategies)
Related Surgical Topics:
- Two-Stage Revision Arthroplasty (spacer fabrication and implantation)
- Debridement Techniques for Osteomyelitis (preparation for antibiotic bead placement)
This comprehensive understanding of local antibiotic delivery systems is essential for managing orthopaedic infections and is frequently tested in orthopaedic fellowship examinations across multiple stations.