Block cyclooxygenase (COX) | Reduce pain, inflammation and prostaglandins | Workhorse analgesic but real GI, renal, cardiovascular and bleeding harms | Two big orthopaedic debates: fracture healing and heterotopic ossification
- Mechanism: NSAIDs inhibit cyclooxygenase (COX), reducing prostaglandins - this gives pain relief, less inflammation and less fever, but also explains every major side effect
- COX-1 versus COX-2: COX-1 is the 'housekeeping' enzyme (protects the stomach, helps platelets clot, maintains kidney blood flow); COX-2 is mainly the 'inflammation' enzyme - selective COX-2 drugs spare the stomach and platelets but not the kidney or heart
- The four classic harms: gastrointestinal (ulcers and bleeding), renal (acute kidney injury, especially in dehydrated or elderly patients), cardiovascular (raised risk of heart attack and stroke), and bleeding (non-selective NSAIDs impair platelets)
- Fracture healing is controversial: large clinical studies link NSAID use - particularly prolonged use - with higher nonunion rates, so most surgeons avoid routine prolonged NSAIDs in fresh fractures and high-risk healing
- Heterotopic ossification: NSAIDs are an established prophylaxis against heterotopic bone after hip surgery and around at-risk fractures - the same anti-prostaglandin effect that may slow healing is used deliberately here
- “If asked why NSAIDs cause both stomach ulcers and bleeding, the answer is COX-1: it normally makes the prostaglandins that protect the gastric lining and the thromboxane that helps platelets aggregate
- “Avoid NSAIDs in the dehydrated, elderly, or those on ACE inhibitors and diuretics - the 'triple whammy' is a classic cause of acute kidney injury
- “The same drug effect is a problem in one setting and a treatment in another: anti-prostaglandin action may impair bone healing, yet it is used on purpose to prevent heterotopic ossification
- “COX-2 selective agents protect the stomach and do not impair platelets, so they are attractive perioperatively - but they carry cardiovascular risk and still harm the kidney
NSAIDs inhibit cyclooxygenase (COX), the enzyme that converts arachidonic acid into prostaglandins (and, via thromboxane, helps platelets clot). Less prostaglandin means less pain, less inflammation and less fever - but also explains every side effect, because prostaglandins also protect the stomach, support kidney blood flow, and help platelets work.
COX-1 is the constitutive 'housekeeping' enzyme (protects the gastric lining, enables platelet aggregation, maintains renal perfusion). COX-2 is mostly inducible at sites of inflammation. Selective COX-2 drugs spare the stomach and platelets but still affect the kidney and carry cardiovascular risk.
Gastrointestinal (ulcers and bleeding), Renal (acute kidney injury, especially with dehydration, age, ACE inhibitors and diuretics), Cardiovascular (raised risk of myocardial infarction and stroke), and Bleeding (non-selective NSAIDs impair platelets). Remember these as a group.
The anti-prostaglandin effect may impair fracture healing (linked to higher nonunion, especially with prolonged use), yet the same effect is used deliberately as heterotopic ossification prophylaxis after hip surgery. Know both sides.
Overview
Non-steroidal anti-inflammatory drugs (NSAIDs) are among the most used drugs in orthopaedics. They relieve pain, calm inflammation, and bring down fever, and they do all of this through a single shared mechanism: blocking the enzyme cyclooxygenase (COX) and so reducing prostaglandins.
The word "non-steroidal" simply distinguishes them from corticosteroids - they reduce inflammation without using a steroid. For the exam, the key idea is that the one mechanism explains everything: the benefits (less pain and inflammation) and the harms (stomach, kidney, heart and bleeding) all come from cutting prostaglandin production in different tissues.
Three themes run through this topic and are heavily examined: how COX-1 and COX-2 differ (and why that matters for side effects), the major harms and who is most at risk, and the two orthopaedic bone debates - whether NSAIDs slow fracture healing, and how the same drugs are used on purpose to prevent heterotopic ossification.
Indications in Orthopaedic Practice
The everyday use - acute injury, soft-tissue pain, and osteoarthritis flares. NSAIDs reduce both the pain and the inflammatory swelling, and topical forms are useful for localised joints.
A core component of postoperative pain control. Scheduled NSAIDs (often with paracetamol) reduce opioid requirements, lowering opioid side effects and aiding early mobilisation.
Given after hip surgery (including acetabular fracture fixation) and in other high-risk situations to prevent heterotopic bone - using the anti-prostaglandin effect deliberately.
Used for acute gout and to settle flares in inflammatory arthritis (indomethacin is a traditional choice for gout), where strong, rapid anti-inflammatory action is needed.
Side Effects and How to Limit Them
- What happens and why
- Loss of COX-1 prostaglandins removes gastric protection - ulcers, gastritis, bleeding
- Who is most at risk / what to do
- Older patients, ulcer history, steroids or anticoagulants - co-prescribe a proton pump inhibitor or use a COX-2 selective agent
- What happens and why
- Prostaglandins keep the afferent arteriole open; blocking them drops renal blood flow - acute kidney injury and fluid retention
- Who is most at risk / what to do
- Dehydrated, elderly, heart failure, or on ACE inhibitors and diuretics (the 'triple whammy') - avoid or use the shortest course
- What happens and why
- Shifting the thromboxane-prostacyclin balance raises risk of myocardial infarction and stroke; fluid retention worsens hypertension and heart failure
- Who is most at risk / what to do
- Established cardiovascular disease - avoid or minimise; naproxen and low-dose ibuprofen are relatively safer choices
- What happens and why
- Non-selective NSAIDs block COX-1 in platelets, reducing thromboxane and impairing aggregation
- Who is most at risk / what to do
- Surgery and anticoagulated patients - COX-2 selective agents do not impair platelets and are preferred where bleeding matters
- What happens and why
- Diverting arachidonic acid toward leukotrienes can trigger bronchospasm
- Who is most at risk / what to do
- Aspirin-sensitive asthma - avoid NSAIDs
- What happens and why
- Reduced prostaglandins may slow the inflammatory phase of fracture repair
- Who is most at risk / what to do
- Fresh fractures at risk of nonunion - avoid prolonged routine use (see evidence below)
An NSAID given alongside an ACE inhibitor (or ARB) and a diuretic is a classic and avoidable cause of acute kidney injury, especially in an older or dehydrated patient. The diuretic depletes volume, the ACE inhibitor drops filtration pressure, and the NSAID removes the prostaglandins the kidney is relying on. Check renal function and hydration, and avoid NSAIDs in this combination where possible.
A clean way to answer "what are the side effects of NSAIDs?" is to work outward from the mechanism. Because they block the prostaglandins that protect the stomach, support the kidney, balance the heart's clotting tendency, and help platelets, you can predict the four big harms - gastrointestinal, renal, cardiovascular and bleeding - rather than memorising a list.
Mechanism of Action
When a cell is injured, an enzyme called phospholipase A2 releases arachidonic acid from the cell membrane. Cyclooxygenase (COX) then converts arachidonic acid into prostaglandins and thromboxane. These molecules drive pain, inflammation, and fever, and they also do useful everyday jobs around the body.
NSAIDs block COX, so less arachidonic acid is turned into prostaglandins. The result is less pain, less inflammation, and less fever - but because the same prostaglandins protect the stomach, support kidney blood flow, and help platelets clot, blocking COX everywhere produces the familiar side effects.
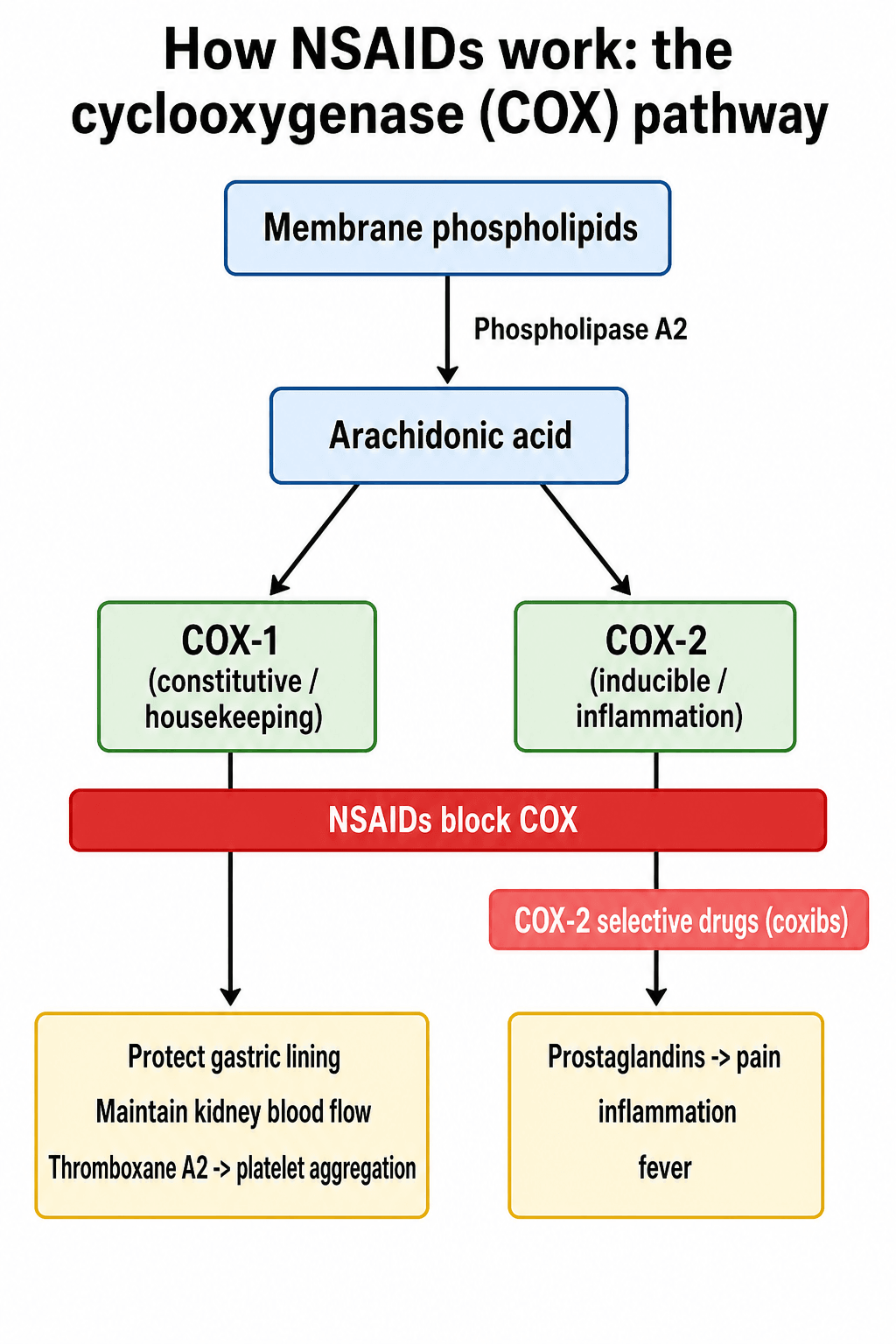
The two forms of the enzyme are the heart of this topic:
- COX-1 (housekeeping)
- Always present (constitutive) in most tissues
- COX-2 (inflammation)
- Mainly switched on (inducible) at sites of injury and inflammation
- COX-1 (housekeeping)
- Protects the gastric lining, enables platelet aggregation (thromboxane), maintains kidney blood flow
- COX-2 (inflammation)
- Produces the prostaglandins that drive pain, swelling and fever; also has roles in the kidney
- COX-1 (housekeeping)
- Removes gastric protection and platelet function - causes ulcers, bleeding and impaired clotting
- COX-2 (inflammation)
- Reduces inflammation and pain - the desired effect
- COX-1 (housekeeping)
- Non-selective NSAIDs block this too (more GI and bleeding harm)
- COX-2 (inflammation)
- COX-2 selective drugs (coxibs) target this and spare the stomach and platelets
The high-yield message: non-selective NSAIDs block both forms, giving strong anti-inflammatory action but more gastric and bleeding problems. COX-2 selective drugs (coxibs) spare COX-1, so they cause less gastric ulceration and do not impair platelets - but they still affect the kidney and carry a recognised cardiovascular risk (thought to relate to an imbalance between prothrombotic thromboxane and protective prostacyclin).
Agents, Selectivity and Routes
- COX selectivity
- Non-selective
- Typical orthopaedic use
- Everyday analgesia, soft-tissue injury, osteoarthritis
- Notes
- Short half-life; relatively lower cardiovascular risk among non-selective agents
- COX selectivity
- Non-selective
- Typical orthopaedic use
- Analgesia and inflammatory conditions
- Notes
- Among the more cardiovascular-neutral NSAIDs; longer acting
- COX selectivity
- Non-selective (somewhat COX-2 leaning)
- Typical orthopaedic use
- Analgesia and heterotopic ossification prophylaxis
- Notes
- Effective but carries higher cardiovascular risk than ibuprofen or naproxen
- COX selectivity
- Non-selective (potent)
- Typical orthopaedic use
- Classic heterotopic ossification prophylaxis; gout
- Notes
- Potent but more gastrointestinal and central side effects
- COX selectivity
- Non-selective (potent, parenteral)
- Typical orthopaedic use
- Short-term strong postoperative analgesia
- Notes
- Powerful opioid-sparing effect; limit to short courses due to GI, renal and bleeding risk
- COX selectivity
- COX-2 selective (coxibs)
- Typical orthopaedic use
- Perioperative analgesia and heterotopic ossification prophylaxis
- Notes
- Spare the stomach and platelets; watch cardiovascular risk and renal effect
Routes matter too. NSAIDs come as oral, intravenous or intramuscular (for example parecoxib and ketorolac for the immediate postoperative period), and topical preparations. Topical NSAIDs deliver drug to a superficial joint with much lower blood levels, so they are a sensible first step for localised osteoarthritis (for example of the knee or hand) in patients who cannot tolerate systemic NSAIDs.
Aspirin: Irreversible COX Inhibition and VTE Prophylaxis
Aspirin is the exception among NSAIDs and a favourite exam point. Whereas the other NSAIDs are reversible, competitive COX inhibitors, aspirin irreversibly acetylates the cyclooxygenase enzyme. Because a platelet has no nucleus and cannot synthesise new COX, a single dose abolishes that platelet's thromboxane production for the rest of its life — so the antiplatelet effect lasts the platelet lifespan (about 7 to 10 days) until enough new platelets are made, far longer than aspirin's short plasma half-life.
This pharmacology underlies two orthopaedic points:
- Stopping before surgery: where platelet function matters, antiplatelet-dose aspirin is typically stopped roughly a week beforehand to allow platelet turnover, whereas the reversible NSAIDs recover within a few half-lives of the drug being cleared.
- Venous thromboembolism (VTE) prophylaxis: low-dose aspirin is now an accepted chemoprophylaxis option after hip and knee arthroplasty and many lower-limb injuries. The randomised evidence is mixed — aspirin performed well in some trials (for example the EPCAT II trial, where aspirin after an initial course of an anticoagulant was non-inferior to continued anticoagulation), while a large trial (CRISTAL) favoured low-molecular-weight heparin for symptomatic VTE — but AAOS and other guidance now list aspirin alongside the anticoagulants, with the choice balancing VTE risk against bleeding.
The Brooker Classification of Heterotopic Ossification
Because NSAIDs are used as heterotopic ossification (HO) prophylaxis around the hip, the examiner expects you to be able to grade HO. The Brooker classification stages HO around the hip on an AP pelvic radiograph and is the system used in the prophylaxis trials below:
- Radiographic appearance
- Islands of bone within the soft tissues around the hip
- Radiographic appearance
- Bone spurs from the pelvis or proximal femur, leaving a gap of at least 1 cm between opposing bone surfaces
- Radiographic appearance
- Bone spurs reducing the gap between opposing bone surfaces to less than 1 cm
- Radiographic appearance
- Apparent bony ankylosis of the hip — opposing surfaces bridged by bone
Grade I is common and usually asymptomatic; Grades III to IV are the clinically important end, restricting movement and occasionally fusing the joint. Prophylaxis (an NSAID course or low-dose radiotherapy) aims to keep an at-risk hip at Brooker 0 to I.
Clinical Relevance
NSAIDs appear in nearly every part of orthopaedic practice and the exam. In clinic, they are the standard treatment for soft-tissue pain and osteoarthritis flares, and the choice between a systemic and a topical agent (and whether to add gastric protection) is everyday decision-making. Perioperatively, NSAIDs are a pillar of multimodal, opioid-sparing analgesia, but the surgeon must weigh bleeding, renal and cardiac risk against the benefits. In trauma and arthroplasty, two bone-specific issues dominate: the fracture-healing controversy (most surgeons avoid prolonged routine NSAIDs in fresh fractures with healing concerns) and heterotopic ossification prophylaxis after hip surgery. Examiners love NSAIDs precisely because the same mechanism is a benefit in one scenario and a hazard in another - so explaining the mechanism, then reasoning to the right decision, scores well.
Guidelines, Registries and Global Practice
- Osteoarthritis guidelines (for example AAOS in the US and NICE in the UK) recommend NSAIDs - topical NSAIDs first where the joint is superficial, then the lowest effective dose for the shortest time of an oral NSAID, with gastric protection or a COX-2 selective agent in those at gastrointestinal risk. The shared message is to individualise the choice to the patient's GI, renal and cardiovascular profile.
- Cardiovascular safety guidance (from medicines regulators in Europe, the UK and the US) is consistent: avoid or minimise NSAIDs in established cardiovascular disease, regard diclofenac and high-dose coxibs as higher cardiovascular risk, and treat naproxen and low-dose ibuprofen as relatively safer choices.
- Heterotopic ossification prophylaxis after hip and acetabular surgery is supported by randomised trials and meta-analysis: indomethacin, diclofenac and celecoxib all reduce heterotopic bone, with radiotherapy as the main alternative where NSAIDs are contraindicated. The choice between NSAID and radiotherapy varies by centre, patient risk, and the competing concern about fracture healing.
- Where guidance differs is mainly in the threshold for prophylaxis, the preferred agent and the duration of any course, rather than in the underlying pharmacology - the four big harms and the two-edged bone effect are universal.
Memory aids
NSAIDNSAID Side Effects
Hook:The drug spells out its own dangers - NSAID: Nephrotoxic, Stomach, Asthma/Allergy, Increased cardiovascular/bleeding risk, Delayed bone healing.
ADDThe Renal Triple Whammy
Hook:ADD up the three and you get acute kidney injury: ACE inhibitor plus Diuretic plus the NSAID Drug - the classic 'triple whammy'.
CAUTIONWhen to Think Twice Before Prescribing
Hook:Use CAUTION before reaching for an NSAID - and match the drug, dose and duration to the patient in front of you.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner hands you an NSAID and asks: how does it work, and what are its main side effects?”
“A fit 30-year-old has a tibial shaft fracture fixed with a nail; the resident has prescribed regular diclofenac for six weeks. Separately, you are planning fixation of an acetabular fracture. How do you think about NSAIDs in each case?”
Mechanism
- Inhibit cyclooxygenase (COX), reducing prostaglandins
- Less pain, inflammation and fever
- COX-1 = housekeeping (stomach, platelets, kidney)
- COX-2 = mainly inducible inflammation enzyme
Selectivity
- Non-selective (ibuprofen, naproxen, diclofenac, indomethacin, ketorolac) - more GI and bleeding harm
- COX-2 selective coxibs (celecoxib, etoricoxib, parecoxib) - spare stomach and platelets
- Coxibs still affect the kidney and carry cardiovascular risk
- Topical NSAIDs - local relief, low systemic exposure
Four Big Harms
- Gastrointestinal - ulcers and bleeding (add a PPI or use a coxib)
- Renal - acute kidney injury, worst in the 'triple whammy' with ACE inhibitor and diuretic
- Cardiovascular - raised heart attack and stroke risk; naproxen relatively safer
- Bleeding - non-selective agents impair platelets
Bone (Two-Edged)
- Possible impaired fracture healing - avoid prolonged routine use in fresh fractures
- Ketorolac linked to higher nonunion (HR about 2.7 in children)
- Established heterotopic ossification prophylaxis after hip surgery
- Celecoxib and diclofenac effective for HO; radiotherapy is the alternative
Evidence: Bone Healing and Heterotopic Ossification
NSAIDs for Heterotopic Ossification Prophylaxis After Total Hip Arthroplasty (Network Meta-analysis)
- Bayesian network meta-analysis of randomised trials - 26 studies and 6396 total hip arthroplasties
- Compared the available NSAID regimens for preventing heterotopic ossification (graded by the Brooker classification)
- Celecoxib showed the highest rate of Brooker class 0 (no heterotopic bone), followed closely by diclofenac
- Celecoxib also had the lowest rates of the higher (more severe) Brooker grades
Postoperative Ketorolac and Nonunion in Pediatric Long-Bone Fractures (Matched Cohort)
- Large propensity-matched cohort - 48,778 children per group from a multinational research network
- Nonunion occurred in 2.19 percent of those given ketorolac versus 0.93 percent of those who were not
- Ketorolac was associated with a roughly 2.7-fold higher hazard of nonunion (HR 2.71)
- The risk was greatest for lower-limb fractures, particularly the femur
Postoperative NSAIDs and Nonunion in Long-Bone Fractures (Database Study)
- Insurance-database study of operatively treated tibial shaft, humeral shaft and subtrochanteric femur fractures
- Nonunion rates were higher with postoperative NSAID use for every fracture type studied
- Subtrochanteric femur fractures had about a 2.4-fold higher nonunion risk with NSAIDs; humeral and tibial shaft about 1.7-fold
- NSAID use remained an independent risk factor for nonunion on multivariate analysis
Be balanced. Laboratory work shows prostaglandins matter for the early inflammatory phase of fracture repair, and several large clinical studies link NSAID use - especially prolonged use and potent agents like ketorolac - with higher nonunion. The evidence is observational and not unanimous, but the pragmatic, exam-safe position is: use NSAIDs for short-term analgesia where helpful, but avoid prolonged routine use in fresh fractures and high-risk healing (for example smokers, diabetics, or comminuted weight-bearing fractures).