HGD Deficiency | Homogentisic Acid | Ochronotic Pigment | Spine-First Arthropathy
- Autosomal recessive deficiency of homogentisate 1,2-dioxygenase (HGD) in the tyrosine pathway
- Homogentisic acid (HGA) accumulates, polymerises and binds collagen as a dark ochronotic pigment
- Black urine from birth, but arthropathy and pigment (ochronosis) appear only in the 4th decade
- Spine is affected first: disc calcification and narrowing precede peripheral joint disease
- Nitisinone (a HPPD inhibitor) lowers HGA by ~99% but causes tyrosinaemia/keratopathy
- “Classic triad: dark urine, ochronotic pigmentation, ochronotic arthropathy
- “Diagnosis confirmed by elevated urinary homogentisic acid
- “Disc calcification with vacuum phenomena is the hallmark spine radiograph
- “Differentiate from ankylosing spondylitis: AKU spares sacroiliac joints early and is HLA-B27 negative
Homogentisate 1,2-dioxygenase (HGD) deficiency, autosomal recessive. Blocks tyrosine catabolism so homogentisic acid (HGA) cannot be converted to maleylacetoacetate. HGA accumulates and is excreted, but excess polymerises into pigment.
HGA-derived polymer binds collagen in cartilage, discs, tendons, sclera, ear and heart valves. The dark deposit (ochronosis) stiffens and embrittles connective tissue, driving a secondary osteoarthritis (ochronotic arthropathy).
Axial disease precedes peripheral disease. Lumbar/thoracic disc calcification, narrowing, vacuum phenomena and progressive ankylosis appear earliest. Large joints (knee, hip, shoulder) follow.
Do not call it ankylosing spondylitis. AKU is HLA-B27 negative, spares the sacroiliac joints early, and shows dense disc calcification rather than syndesmophytes/bamboo spine. Black urine on standing is the giveaway.
SCAREDWhere Ochronotic Pigment Deposits
Hook:Connective tissue gets SCARED black by homogentisic acid pigment.
Overview
Alkaptonuria (AKU) is a rare autosomal recessive inborn error of tyrosine metabolism. The downstream connective-tissue disease it causes is ochronosis, and the resulting joint disease is ochronotic arthropathy. The condition is defined by a triad that an examiner expects you to recite: dark urine, ochronotic pigmentation of connective tissue, and a progressive arthropathy.
The key conceptual point is the time course. Because the enzyme block is present from birth, the urine darkens on standing from infancy. However, the pigment that damages tissue takes decades to accumulate, so ochronosis and arthropathy are usually silent until the fourth decade of life. Patients therefore often present to orthopaedics with "early, severe, spine-dominant osteoarthritis" long before the metabolic diagnosis is made.
Ochronosis is a favourite basic-science and viva topic because it links a single enzyme defect to a recognisable arthropathy, a classic spine radiograph, a named disease-modifying drug (nitisinone) and several "spot diagnosis" signs (scleral and ear pigment, black urine, dark cartilage seen intra-operatively). It rewards candidates who can move smoothly from biochemistry to imaging to management.
- Dark urine: turns black on standing or with alkali
- Ochronosis: blue-grey pigment in sclera, ear, skin
- Arthropathy: spine-first secondary osteoarthritis
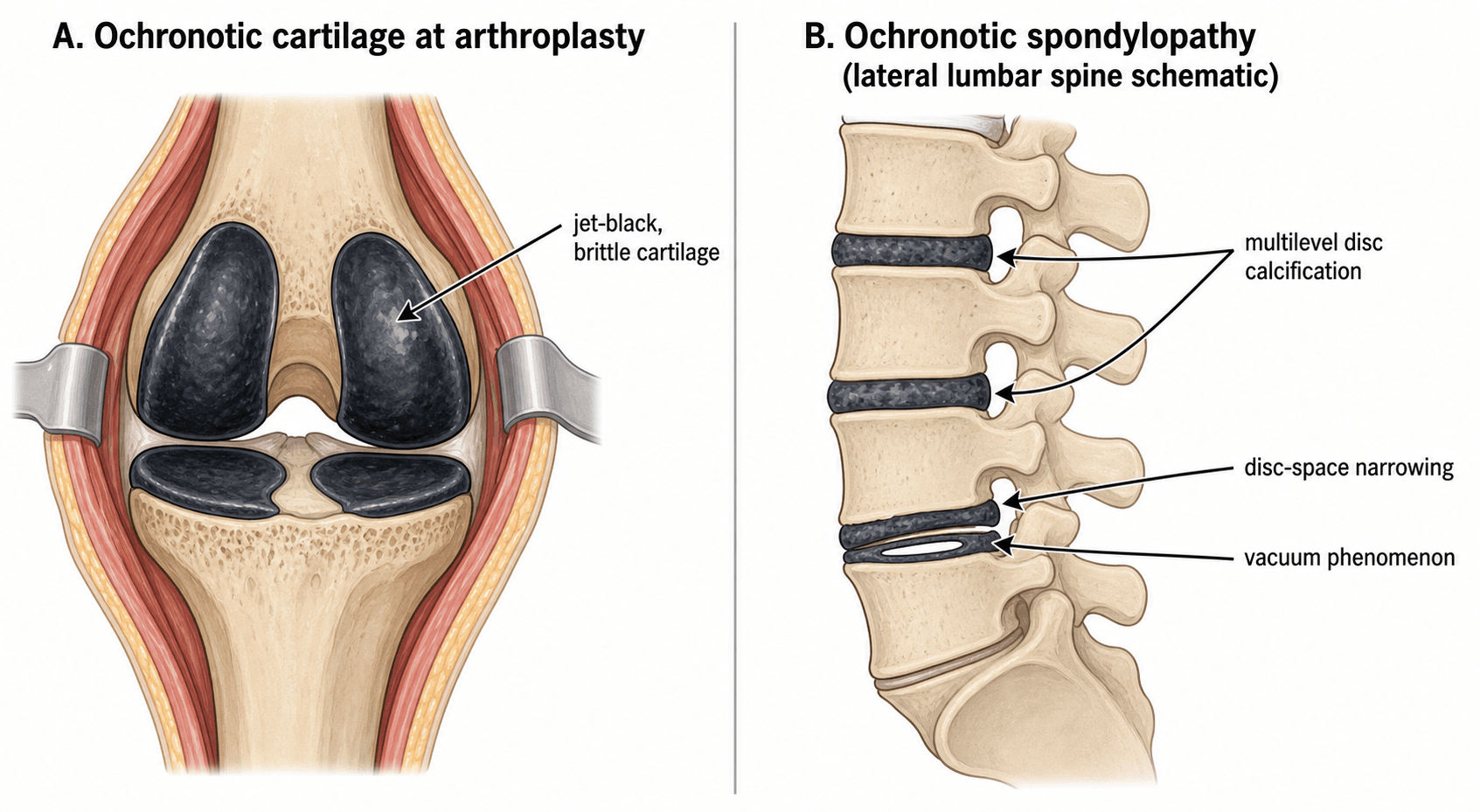
- Intra-operative: jet-black cartilage at arthroplasty
- Sclera: slate-blue pigment (between cornea and canthus)
- Pinna: blue-grey, thickened, leathery ear cartilage
- History: stained nappies/underwear since childhood
Endogenous vs Exogenous Ochronosis
The whole topic uses "ochronosis" as a synonym for alkaptonuria, but the word actually describes the blue-black tissue pigmentation itself, which has two quite different causes. An examiner who asks "is all ochronosis alkaptonuria?" wants this distinction.
Endogenous (metabolic) ochronosis is the alkaptonuria described throughout this topic: a systemic, autosomal recessive HGD deficiency in which homogentisic acid polymerises and deposits in cartilage, discs, sclera, valves and tendons, producing the systemic ochronotic arthropathy.
Exogenous (acquired) ochronosis is a localised, skin-limited pigmentation with normal HGA and no arthropathy, caused by chronic external exposure to certain chemicals - most importantly long-term topical hydroquinone (skin-lightening / bleaching creams), and historically phenol, resorcinol, picric acid and some antimalarials. The chemical inhibits local homogentisic acid oxidase in the dermis, so HGA polymerises and deposits as identical-looking pigment, but only in the treated skin.
- Endogenous (alkaptonuria)
- Inherited HGD deficiency (systemic)
- Exogenous (acquired)
- Chronic topical hydroquinone (or phenol/resorcinol)
- Endogenous (alkaptonuria)
- Markedly raised; urine blackens
- Exogenous (acquired)
- Normal; urine normal
- Endogenous (alkaptonuria)
- Systemic: cartilage, discs, sclera, valves, tendons
- Exogenous (acquired)
- Localised to the skin exposed to the agent (e.g. face)
- Endogenous (alkaptonuria)
- Yes - the defining orthopaedic burden
- Exogenous (acquired)
- No
- Endogenous (alkaptonuria)
- Nitisinone + supportive/arthroplasty
- Exogenous (acquired)
- Stop the offending agent; cosmetic/dermatological
For the orthopaedic surgeon the practical point is the reverse: the systemic, arthropathy-causing ochronosis you meet at the operating table is essentially always the endogenous, alkaptonuric form - but knowing that a skin-limited, HGA-negative exogenous variant exists is the higher-mark answer.
"Ochronosis" = the blue-black pigment, not the disease. Endogenous ochronosis = alkaptonuria (raised HGA, systemic, arthropathy). Exogenous ochronosis = chronic topical hydroquinone (and historically phenol/resorcinol) causing skin-limited pigment with normal HGA and no joint disease. The arthropathy is always the endogenous form.
Mechanism, Pathophysiology and Core Concepts
The Tyrosine Degradation Pathway
Phenylalanine and tyrosine are catabolised through a sequential enzymatic pathway. Ochronosis is caused by a block at a single step.
Sequence:
- Phenylalanine to tyrosine (phenylalanine hydroxylase)
- Tyrosine to 4-hydroxyphenylpyruvate (tyrosine aminotransferase)
- 4-hydroxyphenylpyruvate to homogentisic acid (HGA) (4-hydroxyphenylpyruvate dioxygenase, HPPD)
- HGA to maleylacetoacetate (the BLOCKED step in AKU) - requires homogentisate 1,2-dioxygenase (HGD)
- Maleylacetoacetate eventually to fumarate and acetoacetate
The deficient enzyme is HGD (chromosome 3q13), an autosomal recessive defect. With HGD absent, HGA cannot be opened to maleylacetoacetate and accumulates massively.
- Reaction
- Makes HGA (upstream)
- Status in AKU
- Active
- Therapeutic Relevance
- Target of nitisinone - block it to reduce HGA
- Reaction
- Breaks down HGA
- Status in AKU
- Deficient - the primary defect
- Therapeutic Relevance
- The missing enzyme
This pathway logic is what makes nitisinone rational therapy.
Classification and Patterns of Involvement
There is no single named "classification" of ochronosis, but examiners expect you to organise the disease by system involvement and by the typical sequence in which sites are affected.
- Typical Finding
- Disc calcification, narrowing, vacuum phenomena, ankylosis
- Timing
- Earliest
- Clinical Note
- Most disabling; precedes peripheral disease
- Typical Finding
- Ochronotic OA of knee greater than hip greater than shoulder
- Timing
- After spine
- Clinical Note
- Black cartilage seen at arthroplasty
- Typical Finding
- Relatively spared early
- Timing
- Late
- Clinical Note
- Helps distinguish from ankylosing spondylitis
- Typical Finding
- Aortic valve pigment, calcification, stenosis
- Timing
- Mid-late
- Clinical Note
- Needs echocardiographic surveillance
- Typical Finding
- Embrittlement, spontaneous rupture (e.g. Achilles)
- Timing
- Variable
- Clinical Note
- Pigmented tissue at repair
- Typical Finding
- Blue-grey ochronotic pigment
- Timing
- From 4th decade
- Clinical Note
- Visible spot-diagnosis signs
- Typical Finding
- Stones (HGA-related)
- Timing
- Variable
- Clinical Note
- Can be the presenting feature
Both can cause a stiff, fused spine, but the mechanisms differ. AKU: HLA-B27 negative, dense disc calcification, early sparing of the sacroiliac joints, black urine. Ankylosing spondylitis: HLA-B27 associated, syndesmophytes/bamboo spine, early bilateral sacroiliitis, no urinary colour change.
Clinical Presentation
Age and Mode of Presentation
- Infancy/childhood: dark-staining urine (nappies, underwear) - often the only sign and frequently missed.
- Fourth decade onward: insidious low back pain and stiffness; progressive large-joint pain.
- Spot signs: scleral and ear pigment, blue-grey skin over sweat-gland-rich areas, dark cerumen.
Musculoskeletal Features
- Axial: chronic low back pain, reduced spinal mobility, loss of lumbar lordosis, progressive stiffening toward ankylosis.
- Peripheral: large-joint osteoarthritis (knee most common), effusions, mechanical symptoms from cartilage fragments.
- Tendon: spontaneous rupture (classically the Achilles) due to embrittlement.
Extra-articular Features
- Cardiac: aortic valve pigmentation, stenosis and aortic root involvement; coronary and valvular calcification.
- Genitourinary: renal and prostatic calculi.
- Ophthalmic/cutaneous: scleral pigment, pigmented pinna, skin discolouration.
A patient presenting with severe, early, spine-dominant osteoarthritis plus a heart murmur or renal stones should prompt consideration of ochronosis. The aortic valve disease can be clinically important and warrants echocardiographic assessment.
Investigations
Confirming the Diagnosis
The diagnosis is biochemical and centres on demonstrating homogentisic acid.
- Elevated urinary homogentisic acid (HGA): the diagnostic test; quantified by gas chromatography-mass spectrometry.
- Urine darkening: classic bedside clue - urine turns black on standing or on alkalinisation (oxidation of HGA).
- Serum HGA and tyrosine: measurable; tyrosine becomes especially relevant when monitoring nitisinone therapy.
- HGD gene analysis: confirms the autosomal recessive defect; many pathogenic variants described worldwide.
Adding alkali (or simply leaving the sample to stand and oxidise) turns alkaptonuric urine black. It is a memorable demonstration but quantitative urinary HGA is the definitive test.
Biochemistry, not imaging, makes the definitive diagnosis.
DUOAlkaptonuria Diagnostic Triad
Hook:The DUO of pigment plus arthropathy on a background of dark urine = alkaptonuria.
Differential Diagnosis
The topic differentiates ochronosis from ankylosing spondylitis, but each of its three cardinal signs - calcified discs, dark urine and blue-grey pigment - has its own differential that the examiner can probe. Working through them is what separates a safe candidate from a memorised one.
- Differential to consider
- CPPD (chondrocalcinosis), haemochromatosis arthropathy, DISH, ankylosing spondylitis, prior discitis
- Discriminator
- Ochronosis = HGA-positive + black urine; CPPD = calcium pyrophosphate crystals (see pseudogout-cppd-disease); haemochromatosis = iron studies, hook osteophytes 2nd/3rd MCP (see haemochromatosis-arthropathy); DISH = flowing anterior ossification, preserved discs
- Differential to consider
- Alkaptonuria, porphyria, haematuria, myoglobinuria, melanuria (metastatic melanoma), bile pigment, drugs/food (rifampicin, methyldopa, metronidazole, levodopa, beetroot)
- Discriminator
- Alkaptonuria darkens slowly on standing/alkali and is HGA-positive; myoglobin/haemoglobin are dipstick-positive for blood; porphyria darkens on light exposure
- Differential to consider
- Ochronosis, argyria (silver), minocycline pigmentation, amiodarone, chrysiasis (gold), Addison's, haemochromatosis
- Discriminator
- Ochronosis spares the conjunctiva-free sclera in a wedge between cornea and canthus and the ear cartilage; drug causes follow exposure history; Addison's = mucosal/palmar-crease pigment with low cortisol
- Differential to consider
- Ochronosis, haemochromatosis, CPPD, acromegaly, avascular necrosis, post-traumatic OA
- Discriminator
- Look for the systemic clues (urine, pigment, iron studies, growth features) - 'OA too young, too severe, too symmetric' is the trigger to look deeper
Do not stop at "not ankylosing spondylitis". For calcified discs think CPPD and haemochromatosis; for dark urine think porphyria, myoglobinuria and melanuria; for blue-grey pigment think argyria, minocycline and Addison's. The unifying discriminator for ochronosis is a raised urinary homogentisic acid - everything else fails that test.
Management
Management has two arms: disease-modifying metabolic therapy to reduce HGA, and supportive/orthopaedic care for established connective-tissue damage that pigment has already caused.
Nitisinone (HGA-lowering therapy)
Nitisinone inhibits 4-hydroxyphenylpyruvate dioxygenase (HPPD), the enzyme upstream of the block. By preventing HGA formation it dramatically reduces the substrate that drives ochronosis.
- Efficacy: in the SONIA 2 randomised trial, 10 mg daily reduced 24-h urinary HGA by ~99.7% at 12 months and slowed clinical disease progression (lower cAKUSSI score at 48 months) versus no treatment.
- Dose-response: SONIA 1 showed a clear dose-dependent fall in urinary HGA across 1-8 mg, with ~99% reduction at 8 mg.
- Caveat - acquired tyrosinosis: blocking HPPD raises tyrosine in serum and tissues, risking corneal keratopathy (potentially sight-threatening) and prompting attention to diet.
Nitisinone is highly effective at lowering HGA but causes hypertyrosinaemia/tyrosinosis. Patients require tyrosine monitoring, ophthalmic vigilance for keratopathy, and often dietary protein modification to mitigate the tyrosine rise.
The drug treats the cause but introduces a new metabolic problem to manage.
Complications
Progressive disc calcification, narrowing and ankylosis cause chronic back pain, loss of spinal mobility and, rarely, neurological compromise.
Premature, severe osteoarthritis of large joints (knee, hip, shoulder) often requiring multiple arthroplasties.
Aortic valve pigmentation, stenosis and root involvement; valvular and vascular calcification needing surveillance and sometimes replacement.
Embrittled tendons (classically Achilles) can rupture spontaneously; tissue is pigmented and friable at repair.
Renal and prostatic calculi related to HGA, occasionally the presenting feature.
Nitisinone-induced hypertyrosinaemia can cause corneal keratopathy and, with very high tyrosine, neurocognitive concerns - hence monitoring.
Clinical Relevance
The Surgeon's Perspective
Ochronosis is the rare metabolic disease that an orthopaedic surgeon is genuinely likely to encounter at the operating table. The first clue is often black cartilage discovered unexpectedly during arthroplasty in a patient labelled as having "primary" osteoarthritis. Recognising this prompts the metabolic diagnosis, family screening and systemic assessment (especially the aortic valve).
Why the Spine Comes First
The intervertebral disc is rich in type II collagen and proteoglycan and has a high collagen turnover environment that favours pigment binding. The result is the characteristic multilevel disc calcification that distinguishes ochronotic spondylopathy from other causes of a stiff spine and predates peripheral disease.
A Model Disease for Metabolic Therapy
AKU is also a teaching example of rational drug design: because the defect is loss of a downstream enzyme, blocking the upstream enzyme (HPPD) with nitisinone reduces the toxic intermediate. The trade-off - accumulation of tyrosine - illustrates the principle that re-routing a metabolic pathway shifts, rather than abolishes, the metabolic burden.
Guidelines, Registries & Global Practice
Ochronosis is a rare disease, so practice is shaped by specialist centres and rare-disease frameworks rather than mainstream arthroplasty guidelines. The biology is universal; access to diagnosis and to nitisinone is not.
Global Epidemiology
- Alkaptonuria is rare worldwide, with an estimated birth prevalence of roughly 1 in 250,000 to 1 in 1,000,000 in most populations.
- Geographic clusters of much higher prevalence exist, notably in Slovakia and parts of the Dominican Republic, reflecting founder effects in the HGD gene.
- Many distinct pathogenic HGD variants have been catalogued internationally (for example, large variant cohorts described in Russia), underpinning genetic confirmation and family screening.
Therapy Access and Regulatory Status
- Position
- Nitisinone lowers HGA by ~99% (SONIA trials)
- Practical Implication
- Mainstay where available; needs metabolic supervision
- Position
- Dedicated AKU services (e.g. UK National Alkaptonuria Centre)
- Practical Implication
- Concentrate expertise, monitoring and dietetics
- Position
- Tyrosine, ophthalmology, dietetics
- Practical Implication
- Mandatory alongside nitisinone
- Position
- Standard arthroplasty principles apply
- Practical Implication
- Plan for multi-joint disease and poor tissue quality
There is broad consensus that HGA-lowering with nitisinone plus structured monitoring is the rational disease-modifying approach, and that end-stage arthropathy is treated with arthroplasty using conventional principles adapted for stiff joints and friable tissue.
Registries & Surveillance
- No large arthroplasty registry isolates ochronotic arthropathy, but national joint registries (NJR, AJRR, AOANJRR, SHAR, NZJR) capture implant survival data that inform implant choice when these patients require replacement.
- Rare-disease registries and dedicated AKU cohorts (linked to the SONIA programme and patient organisations such as the AKU Society) are the principal source of natural-history and treatment-outcome data.
High- vs Limited-Resource Practice Variation
- High-resource settings: access to genetic confirmation, nitisinone with tyrosine/ophthalmic monitoring, dietetics and elective multi-joint arthroplasty.
- Limited-resource settings: diagnosis is often delayed to the arthroplasty table; management relies on analgesia, physiotherapy and replacement when feasible, with limited access to nitisinone.
MCQ Practice Points
Q: Which enzyme is deficient in alkaptonuria? A: Homogentisate 1,2-dioxygenase (HGD) - an autosomal recessive defect causing accumulation of homogentisic acid.
Q: What is the definitive diagnostic test for alkaptonuria? A: Elevated urinary homogentisic acid - the urine also classically turns black on standing or alkalinisation.
Q: What is the hallmark spine radiographic finding in ochronosis? A: Multilevel intervertebral disc calcification with disc-space narrowing and vacuum phenomena.
Q: What is the mechanism of nitisinone in alkaptonuria? A: Inhibition of 4-hydroxyphenylpyruvate dioxygenase (HPPD), the upstream enzyme, reducing production of homogentisic acid.
Q: Which feature distinguishes ochronotic spondylopathy from ankylosing spondylitis? A: Dense disc calcification with early sacroiliac sparing and HLA-B27 negativity (versus syndesmophytes and early sacroiliitis in AS).
Q: What is the main metabolic side effect of nitisinone therapy? A: Hypertyrosinaemia (acquired tyrosinosis), which can cause sight-threatening corneal keratopathy and requires monitoring.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“During a total knee replacement for presumed primary osteoarthritis you encounter jet-black, brittle articular cartilage. The examiner asks how you interpret and act on this.”
“A 45-year-old presents with chronic back pain and a stiff spine. Radiographs show dense calcification of multiple intervertebral discs. The examiner asks you to characterise and differentiate the findings.”
“An examiner asks you to explain, from biochemistry to clinical trial, how alkaptonuria can be disease-modified and why the treatment is not without cost.”
Biochemistry
- **Defect**: HGD deficiency (autosomal recessive)
- **Accumulates**: Homogentisic acid (HGA)
- **Pigment**: HGA polymer binds collagen (ochronosis)
Clinical / Imaging
- **Triad**: dark urine, pigmentation, arthropathy
- **Spine first**: disc calcification + vacuum sign
- **Spot signs**: scleral/ear pigment, black cartilage
Management
- **Diagnose**: urinary HGA (definitive)
- **Disease-modify**: nitisinone (inhibits HPPD)
- **Caveat**: tyrosinaemia/keratopathy; arthroplasty for end-stage
Evidence Base
SONIA 2: Nitisinone Reduces HGA and Slows Progression
- 138 patients aged 25+ randomised 1:1 to nitisinone 10 mg daily or no treatment over 4 years
- Urinary HGA at 12 months fell by 99.7% with nitisinone versus control
- cAKUSSI clinical severity score rose significantly less with nitisinone at 48 months (adjusted difference -8.6 points)
- Well tolerated with no treatment-related deaths; supports nitisinone as a disease-modifying therapy
SONIA 1: Dose-Dependent HGA Lowering by Nitisinone
- 40 patients randomised to no treatment or nitisinone 1, 2, 4 or 8 mg daily for 4 weeks
- Clear dose-response: 24-h urinary HGA fell progressively across doses
- The 8 mg dose reduced urinary HGA by ~98.8% from baseline
- Tyrosine rose at all doses but no serious adverse events over 4 weeks
References
-
Ranganath LR, Psarelli EE, Arnoux JB, et al. Efficacy and safety of once-daily nitisinone for patients with alkaptonuria (SONIA 2): an international, multicentre, open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2020. PMID 32822600.
-
Ranganath LR, Milan AM, Hughes AT, et al. Suitability Of Nitisinone In Alkaptonuria 1 (SONIA 1): a randomised, open-label, dose-response study. Ann Rheum Dis. 2014. PMID 25475116.
-
Rajkumar N, Soundarrajan D, Dhanasekararaja P, Rajasekaran S. Clinical and radiological outcomes of total joint arthroplasty in patients with ochronotic arthropathy. Eur J Orthop Surg Traumatol. 2020. PMID 32172376.
-
Khedr M, Cooper MS, Hughes AT, et al. Nitisinone causes acquired tyrosinosis in alkaptonuria. J Inherit Metab Dis. 2020. PMID 32083330.
-
Mistry JB, Bukhari M, Taylor AM. Alkaptonuria. Rare Dis. 2013. PMID 25003018.
-
Grosicka A, Kucharz EJ. Alkaptonuria. Wiad Lek. 2009. PMID 20229718.
-
Soltysova A, Kuzin A, Samarkina E, Zatkova A. Alkaptonuria in Russia. Eur J Hum Genet. 2021. PMID 34504318.