Orthopaedic Antibiotic Therapy
Take deep cultures (and blood cultures) before starting antibiotics whenever the patient is stable. Blind early antibiotics can sterilise the surface and leave deep cultures negative, so you lose the chance to target therapy. The exception is sepsis, where you cannot delay treatment.
Antibiotics are an adjunct to surgery, not a replacement. Pus must be drained, dead bone (a sequestrum) excised, and an infected implant debrided or removed. An antibiotic cannot penetrate a sequestrum or a mature biofilm.
Bacteria on implants form a biofilm that resists antibiotics and immune cells. For susceptible staphylococcal implant infection, add rifampicin to a partner drug - it penetrates biofilm and kills slow-growing organisms. Never use rifampicin alone (rapid resistance).
Choose agents that reach bone: clindamycin, fluoroquinolones, rifampicin, fusidic acid and linezolid penetrate well. Glycopeptides such as vancomycin penetrate less well, which matters when oral switch or deep cure is the goal.
Overview
This topic is about using antibiotics to treat established orthopaedic infection - osteomyelitis, septic arthritis, and prosthetic joint or other implant infection. It is the opposite side of the coin to surgical prophylaxis: prophylaxis prevents infection in clean tissue before contamination, whereas here the infection is already present and the goal is to eradicate it.
Three ideas run through everything that follows and are the threads examiners pull on. First, antibiotics are an adjunct to surgery - dead bone and infected implants must be dealt with surgically, because no drug penetrates a sequestrum or a mature biofilm. Second, the right drug means an agent that covers the likely organism (usually Staphylococcus aureus) and actually reaches bone. Third, biofilm on implants changes the rules: it is the reason implant infection is so hard to clear, the reason rifampicin is added for susceptible staphylococci, and the reason an implant sometimes has to be removed.
Principles: How Antibiotics Work in Bone Infection
To clear a bone or joint infection an antibiotic has to do three things: reach the infected tissue at an adequate concentration, remain active against the organism, and keep working in the hostile environment of infected bone (low oxygen, dead tissue, biofilm).
Why bone is a difficult place to treat:
- Poor blood supply: chronically infected, sclerotic bone and any dead fragment (a sequestrum) have little or no blood flow, so the drug simply cannot get there. This is the single biggest reason chronic osteomyelitis needs surgery.
- Biofilm: bacteria on implant surfaces and dead bone secrete a protective matrix. Inside it they grow slowly and tolerate antibiotic concentrations many times higher than would kill free-floating bacteria.
- Intracellular survival: Staphylococcus aureus can survive inside osteoblasts and other cells, providing a reservoir that ordinary antibiotics reach poorly.
Bone penetration of common agents:
- Bone penetration
- Good
- Typical role in bone or joint infection
- Staph and anaerobe cover, useful oral switch
- Bone penetration
- Good
- Typical role in bone or joint infection
- Gram-negative cover and the usual rifampicin partner
- Bone penetration
- Good (penetrates biofilm)
- Typical role in bone or joint infection
- Added for susceptible staph implant infection - never alone
- Bone penetration
- Good
- Typical role in bone or joint infection
- Oral options against resistant gram-positives
- Bone penetration
- Moderate
- Typical role in bone or joint infection
- First-line for methicillin-susceptible S. aureus (MSSA)
- Bone penetration
- Lower
- Typical role in bone or joint infection
- MRSA cover but less reliable bone levels
Bone and joint infection means weeks of antibiotics, so the safety and interaction profile is examinable in its own right:
- Rifampicin is a potent hepatic enzyme (cytochrome P450) inducer — it lowers the effect of warfarin, the oral contraceptive pill (counsel on alternative contraception) and many other drugs, can be hepatotoxic, and turns secretions orange (staining tears and contact lenses).
- Fluoroquinolones (the rifampicin partner) cause tendinopathy and tendon rupture — classically the Achilles, especially in the elderly, in renal impairment, or with concurrent steroids — plus QT prolongation and CNS effects.
- Linezolid causes reversible myelosuppression (especially thrombocytopenia) beyond about two weeks, peripheral and optic neuropathy with prolonged use, and is a monoamine-oxidase inhibitor (serotonin syndrome risk with SSRIs).
- Aminoglycosides (gentamicin) are nephrotoxic and ototoxic (relevant both systemically and from high-dose local elution); vancomycin is nephrotoxic and needs therapeutic level monitoring; clindamycin is the classic cause of Clostridioides difficile colitis.
- A prolonged (often outpatient, OPAT) course therefore needs monitoring of the full blood count, renal and liver function, and drug levels.
Biofilm and the Role of Rifampicin
Biofilm is the central concept in implant-associated infection. Within hours of contamination, bacteria attach to the implant surface and to dead bone and begin to secrete an extracellular matrix. The bacteria inside this biofilm are metabolically slow, physically shielded from antibiotics and immune cells, and can tolerate drug concentrations that would easily kill the same organism floating free. This is why a biofilm-coated implant usually cannot be sterilised by antibiotics alone and often has to be removed.
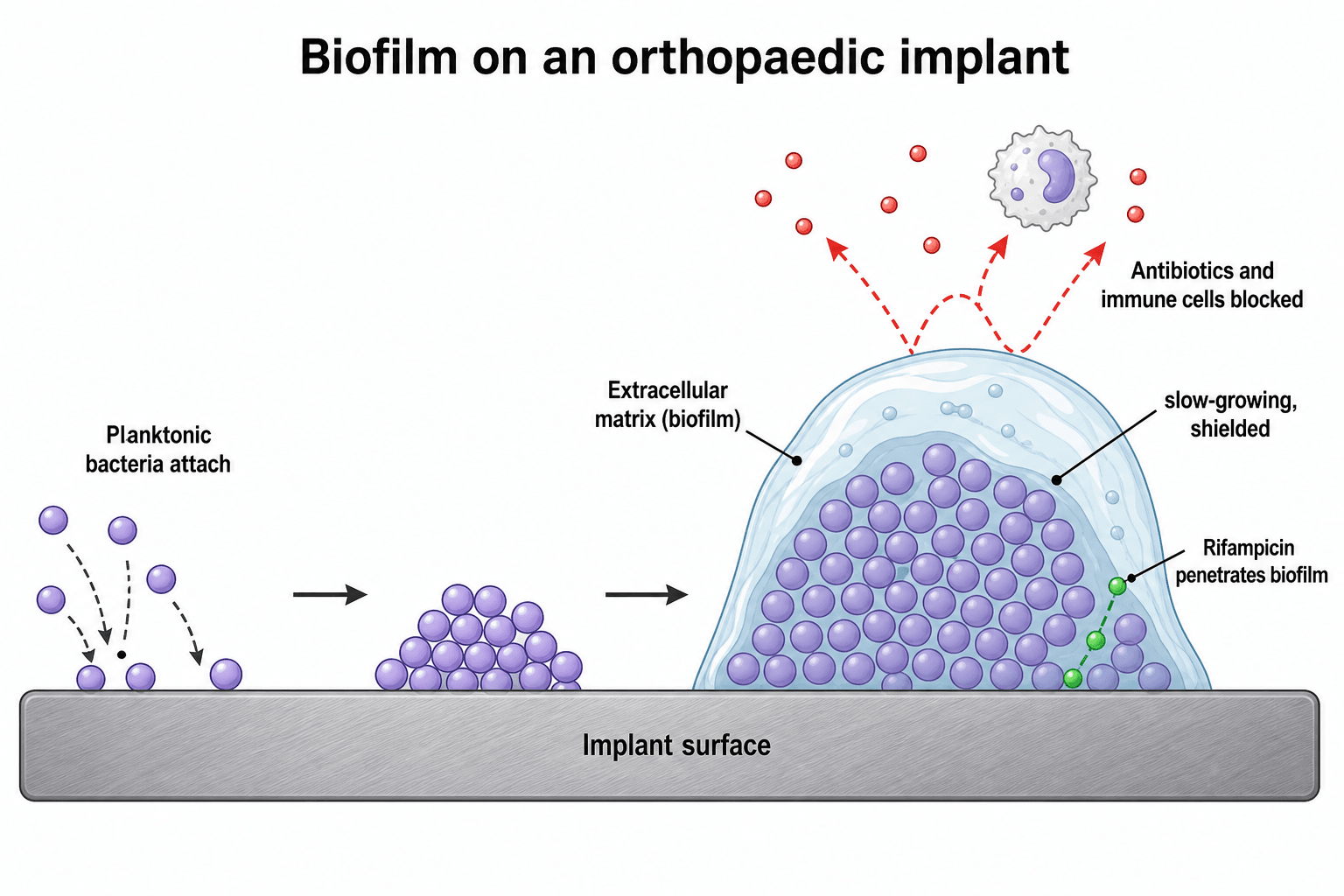
Rifampicin is special because it penetrates biofilm and kills slow-growing, adherent staphylococci that other drugs miss. The catch is that staphylococci develop resistance to rifampicin very quickly if it is used on its own, so it is always combined with a partner drug (commonly a fluoroquinolone such as ciprofloxacin or levofloxacin). The classic indication is a stable, susceptible staphylococcal implant infection of short duration that is being managed with debridement and implant retention (DAIR).
Rifampicin is the "biofilm" answer in the viva, but two qualifiers must always come with it: it is only added once a partner drug is established and the wound is dry (to avoid selecting resistance), and it is only worth using when the implant is stable and the infection is caught early. A loose implant or long-standing infection usually needs removal, not rifampicin.
Systemic antibiotics are only half the story in implant and bone infection; local delivery achieves very high concentrations at the site with low systemic levels:
- Antibiotic-loaded PMMA (bone cement) — antibiotic powder mixed into polymethylmethacrylate as beads/chains, a cement mantle, or an articulating or static spacer in two-stage revision; it elutes a high early "burst" then a long low-level tail.
- Only heat-stable, powdered antibiotics can be used (the cement polymerises with an exothermic reaction): gentamicin, tobramycin and vancomycin are the standard choices; liquid or heat-labile agents are unsuitable.
- High antibiotic loading weakens the cement, so heavily loaded "high-dose" cement is used for spacers and beads (infection control) rather than for load-bearing structural fixation.
- PMMA is non-absorbable — it is itself a foreign body that can host biofilm and usually has to be removed; biodegradable carriers that do not need removal (calcium sulphate beads, gentamicin-collagen sponges, bioactive glass) are alternatives.
- In two-stage revision the infected implant is removed and replaced with an antibiotic spacer; after an interval of systemic antibiotics and confirmed clearance, the definitive implant is reimplanted.
Antibiotic Therapy by Clinical Scenario
Acute (including haematogenous) osteomyelitis
Commonest organism: Staphylococcus aureus. In specific groups think wider - Salmonella and other gram-negatives in sickle cell disease, group B streptococcus and gram-negatives in neonates, Kingella kingae in young children.
Principles:
- Take blood cultures and, where feasible, a bone aspirate or biopsy before antibiotics.
- Start empirical anti-staphylococcal therapy (for example flucloxacillin for MSSA; add MRSA cover such as vancomycin where MRSA is likely), then narrow to the culture.
- Surgery (drainage, debridement) is needed if there is an abscess, a sequestrum, or failure to respond to antibiotics.
- Duration is commonly around 6 weeks total for osteomyelitis, individualised to the organism, the surgery performed, and the clinical and inflammatory-marker response.
Uncomplicated acute haematogenous osteomyelitis in a child, caught early, often responds to antibiotics alone with an early switch from intravenous to oral therapy once the child improves and markers fall. Surgery is reserved for abscess, no response, or a confirmed septic joint.
Clinical Relevance
Antibiotic therapy for infection touches every part of orthopaedic practice and the exam. In trauma, early antibiotics plus debridement halve the early infection rate after open fractures. In arthroplasty, prosthetic joint infection is a feared complication, and the decision to retain (with rifampicin) or remove the implant is a core viva. In paediatrics, acute haematogenous osteomyelitis and septic arthritis are emergencies where prompt, correctly chosen antibiotics after cultures can avoid surgery or growth disturbance. In the basic-science viva, the biofilm concept, bone penetration, and the rifampicin rule are classic asks. Across all of these the same principles apply: culture, source control, the right drug into bone, narrow to the organism, and a defined duration.
Guidelines, Registries and Global Practice
- Staphylococcus aureus is consistently reported as the commonest organism in osteomyelitis, septic arthritis, and prosthetic joint infection across global series, so empirical regimens everywhere are built around reliable anti-staphylococcal cover.
- Local resistance patterns drive empirical choice: where MRSA prevalence is high, empirical regimens add a glycopeptide (such as vancomycin) or another MRSA-active agent until cultures return, then narrow.
- The OVIVA trial has shifted international practice towards earlier oral switch for stable bone and joint infection, reducing prolonged intravenous lines and hospital stay while preserving cure rates.
- The rifampicin combination for stable staphylococcal implant infection, established by the Zimmerli foreign-body infection trial, is embedded in major prosthetic-joint-infection guidance (for example IDSA and European consensus statements) as the basis for the DAIR strategy.
- For open fractures, society guidance worldwide pairs early antibiotics with prompt irrigation, debridement and stabilisation, keeping antibiotic courses short and grade-appropriate rather than open-ended.
Memory aids
CLEANEDPrinciples of Treating Bone and Joint Infection
Hook:Get the bone CLEANED - cultures, localise, excise, agent, narrow, enough, decide on the implant.
CFR-LFAntibiotics with Good Bone Penetration
Hook:CFR-LF reach bone: Clindamycin, Fluoroquinolones, Rifampicin, Linezolid, Fusidic acid.
LONGWhen an Implant Cannot Be Saved
Hook:A LONG, loose, old, untreatable, septic implant comes out rather than being retained.

Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
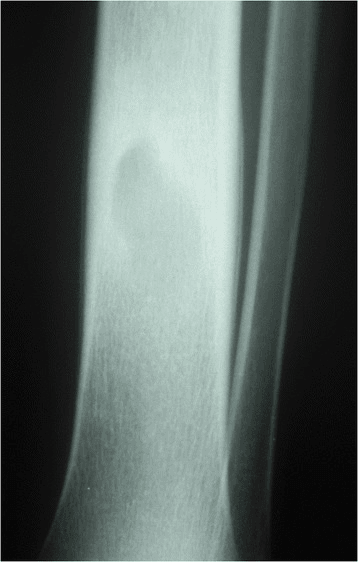
“A 40-year-old man has chronic osteomyelitis of the tibia after a previous open fracture, with a discharging sinus. The examiner asks how you would approach antibiotic treatment.”
“A 70-year-old woman develops a hot, painful hip three weeks after a primary total hip replacement. The wound is healing and the implant looks well-fixed on radiographs. How would you manage the infection and what is the role of rifampicin?”
Core Principles
- Treatment of established infection - an adjunct to surgery, never a substitute
- Cultures (deep and blood) before antibiotics if the patient is stable
- Source control first: drain pus, excise dead bone, debride or remove implant
- Narrow empirical therapy to the cultured organism
The Right Drug
- Cover Staphylococcus aureus empirically (the commonest organism)
- Pick agents that reach bone: clindamycin, fluoroquinolones, rifampicin, linezolid, fusidic acid
- Flucloxacillin for MSSA; vancomycin for MRSA (lower bone penetration)
- Rifampicin for susceptible staph implant infection - always with a partner drug
Biofilm and Implants
- Biofilm shields bacteria from antibiotics and immune cells
- Stable, early, susceptible implant infection: DAIR plus rifampicin combination
- Loose implant, chronic infection, sinus, or resistant organism: remove the implant
- Never give rifampicin alone (rapid resistance)
Duration and Route
- Osteomyelitis: commonly around 6 weeks total, individualised
- Septic arthritis: shorter (often 2 to 4 weeks) once the joint is washed out
- Oral is non-inferior to IV for many bone/joint infections once stable (OVIVA)
- Open fractures: early antibiotics plus urgent debridement, short grade-appropriate course
Evidence Base
Every citation below has been checked against its source record in PubMed. Three trials anchor the topic: OVIVA (oral is non-inferior to IV once stable), the Zimmerli Foreign-Body Infection trial (the evidence base for rifampicin-combination DAIR in stable staphylococcal implant infection), and the Gosselin Cochrane review (early antibiotics roughly halve open-fracture infection, as an adjunct to debridement).
Oral versus Intravenous Antibiotics for Bone and Joint Infection (OVIVA)
- Randomised non-inferiority trial, 1054 adults treated for bone or joint infection at 26 UK centres
- Oral versus intravenous antibiotics for the first 6 weeks after surgery or starting treatment
- Treatment failure at one year: 13.2 percent oral versus 14.6 percent intravenous - oral was non-inferior
- Oral therapy was associated with shorter hospital stay and fewer intravenous-catheter complications
Rifampicin Combination Cures Staph Implant Infection (FBI Study, Zimmerli)
- Randomised, double-blind, placebo-controlled trial in staphylococcal infection of stable orthopaedic implants
- All patients had debridement and a short-duration infection, then ciprofloxacin plus rifampicin or placebo
- Cure without implant removal: 100 percent (12 of 12) with rifampicin versus 58 percent (7 of 12) with placebo
- Established that biofilm-active rifampicin combinations can salvage a retained implant in selected cases
Antibiotics Roughly Halve Early Open-Fracture Infection (Cochrane Review)
- Systematic review pooling 913 participants across randomised and quasi-randomised trials
- Antibiotics reduced early infection versus placebo or no antibiotic (relative risk 0.41)
- Absolute risk reduction about 8 percent, with a number needed to treat of roughly 13
- Insufficient data to judge effects on osteomyelitis, nonunion, amputation or death