Benign Adipocytic Tumor | Most Common Soft Tissue Mass | Excellent Prognosis
- Most common soft tissue tumor in adults (50% of all benign masses)
- Superficial lipomas rarely transform to sarcoma (less than 1%)
- Deep or rapidly growing lipomas require MRI to exclude liposarcoma
- Simple excision curative for superficial lesions; recurrence less than 5%
- Histology shows mature adipocytes without atypia or lipoblasts
- “Deep lipomas have higher recurrence and require imaging to exclude malignancy
- “Atypical lipomatous tumor (ALT) is well-differentiated liposarcoma by another name
- “Multiple lipomas suggest familial lipomatosis or Madelung disease
- “Intramuscular lipomas infiltrate and have 20% recurrence after marginal excision
Deep location, size greater than 5cm, rapid growth are red flags for liposarcoma. MRI shows thick septations, nodularity, and contrast enhancement in malignant lesions.
Superficial (subcutaneous), deep (subfascial), intramuscular - location determines recurrence risk and need for imaging. Deep lesions require MRI to rule out well-differentiated liposarcoma.
Conventional, spindle cell, pleomorphic, hibernoma - most are conventional mature fat. Atypical features (lipoblasts, MDM2 amplification) indicate liposarcoma.
Observation vs simple excision - asymptomatic superficial lipomas can be observed. Symptomatic, deep, or atypical lesions require excision with marginal margins.
LARGELipoma Red Flags (Suspect Liposarcoma)
Hook:LARGE lipomas need imaging - think liposarcoma until proven otherwise!
Overview and Epidemiology
Lipomas are benign tumors of mature adipose tissue and represent the most common soft tissue neoplasm in adults. They are the largest single diagnostic category among benign soft tissue tumors (16% of an AFIP pathology archive of 18,677 benign lesions; up to roughly half of masses in some clinical referral series) and have an estimated incidence of about 1 per 1000 individuals. Most lipomas are solitary, slow-growing, and superficial (subcutaneous), presenting as soft, mobile masses that are asymptomatic.
Lipomas are the single most common reason for referral to soft tissue tumor clinics. The key clinical challenge is distinguishing benign lipoma from well-differentiated liposarcoma (atypical lipomatous tumor) in deep-seated lesions.
- Age: Peak incidence 40-60 years
- Gender: Equal male and female distribution
- Location: 80% trunk and extremities
- Multiplicity: 5-10% have multiple lipomas
- Familial lipomatosis: Autosomal dominant
- Madelung disease: Multiple symmetric lipomas, alcohol-related
- Gardner syndrome: Lipomas with colonic polyposis
- Proteus syndrome: Hamartomatous overgrowth
Pathophysiology and Anatomy
Anatomical Locations
Lipomas can arise in any location where adipose tissue is present. The distribution and behavior varies by anatomical site.
- Frequency
- 40%
- Anatomical Considerations
- Subcutaneous fat layer, superficial
- Clinical Significance
- Easily accessible, low recurrence
- Frequency
- 25%
- Anatomical Considerations
- Superficial or within muscle compartments
- Clinical Significance
- Intramuscular type more common in thigh
- Frequency
- 20%
- Anatomical Considerations
- Thigh most common, often intramuscular
- Clinical Significance
- Higher recurrence for intramuscular type (20%)
- Frequency
- 10%
- Anatomical Considerations
- Spindle cell variant common posteriorly
- Clinical Significance
- Cosmetically sensitive area
- Frequency
- Under 5%
- Anatomical Considerations
- Deep to abdominal cavity
- Clinical Significance
- High risk of being atypical lipomatous tumor
Tissue Biology
Lipomas arise from mature adipocytes with clonal chromosomal abnormalities. Despite being benign, they represent true neoplasms rather than simply excess fat.
- Arise from mesenchymal adipocyte precursors
- Clonal chromosomal aberrations (12q13-15 in 60-70%)
- Encapsulated by thin fibrous pseudocapsule
- Distinct from normal adipose tissue (neoplastic)
- Soft consistency allows compression through small incisions
- Pseudocapsule provides natural dissection plane
- Intramuscular type infiltrates between muscle fibers
- Deep lesions may compress adjacent neurovascular structures
Histology and Pathophysiology
Cellular Composition
Lipomas are composed of mature adipocytes identical to normal subcutaneous fat. The key histological feature is encapsulation by a thin fibrous pseudocapsule, allowing easy enucleation during surgery. Unlike normal fat, lipomas have clonal chromosomal aberrations (12q13-15 rearrangements in 60-70% of cases) indicating neoplastic origin.
Critical histological differences:
- Lipoma: Mature adipocytes, no atypia, no lipoblasts
- Well-differentiated liposarcoma: Lipoblasts, nuclear atypia, MDM2/CDK4 amplification (FISH positive)
- Deep lipomas greater than 5cm should be biopsied or have MDM2 testing to exclude liposarcoma
Histological Variants
- Histological Features
- Mature adipocytes, thin capsule
- Clinical Behavior
- Benign, less than 5% recurrence
- Treatment
- Simple excision
- Histological Features
- Fat with spindle cells and collagen
- Clinical Behavior
- Benign, posterior neck/shoulder common
- Treatment
- Simple excision
- Histological Features
- Bizarre nuclei (degenerative atypia)
- Clinical Behavior
- Benign despite atypia, posterior neck
- Treatment
- Excision, rule out liposarcoma
- Histological Features
- Infiltrates muscle fibers
- Clinical Behavior
- Higher recurrence (20%), thigh common
- Treatment
- Wide excision
- Histological Features
- Brown fat (multivacuolated cells)
- Clinical Behavior
- Benign, highly vascular on imaging
- Treatment
- Excision if symptomatic
Classification Systems
By Anatomical Location
- Location
- Above muscle fascia
- Characteristics
- 90% of lipomas, easily mobile, typical exam
- Recurrence Risk
- Under 5%
- Location
- Below fascia, not within muscle
- Characteristics
- May compress adjacent structures, MRI needed
- Recurrence Risk
- 5-10%
- Location
- Within muscle fibers
- Characteristics
- Infiltrates muscles, difficult complete excision
- Recurrence Risk
- 15-20%
- Location
- Between muscle groups
- Characteristics
- May involve neurovascular bundles
- Recurrence Risk
- 10-15%
Classification by location determines the need for imaging, surgical approach, and expected recurrence risk.
Clinical Assessment
History
- Painless mass: Most common presentation (80%)
- Cosmetic concern: Visible lump, especially facial/neck
- Mechanical symptoms: Compression of adjacent structures
- Duration: Usually years (slow growth)
- Rate of growth: Rapid growth concerning for sarcoma
- Pain: Lipomas typically painless; pain suggests angiolipoma or malignancy
- Family history: Multiple lipomas may be familial
- Trauma history: Some patients report preceding trauma (no causal link proven)
Physical Examination
Examination Sequence
Look for:
- Size and location of mass
- Skin changes (rarely present in lipomas)
- Multiple masses (familial lipomatosis)
Characteristic findings:
- Soft, doughy consistency
- Mobile (moves with skin, not muscle)
- Non-tender unless angiolipoma variant
- Lobulated surface
- Slip sign positive (slips under fingers)
Muscle contraction test:
- Superficial lipomas become more prominent with muscle relaxation
- Deep lipomas become less prominent or fixed with muscle contraction
- This simple test guides need for imaging
Concerning features on examination:
- Fixed to deep structures
- Firm or hard consistency
- Rapid enlargement
- Size greater than 5cm
- Deep to fascia
- Associated neurovascular symptoms
These findings warrant MRI imaging to exclude liposarcoma.
Investigations
Imaging Protocol
Superficial (Subcutaneous) Approach
Indications for imaging:
- Size greater than 5cm
- Atypical examination findings
- Deep location suspected
Ultrasound (first-line for superficial lesions):
- Hyperechoic mass with fine internal echoes
- Parallel orientation
- Thin or absent capsule
- No internal vascularity on Doppler

Outcome: Most superficial lipomas under 5cm do not require imaging before excision.
- Benign Lipoma
- Usually under 5cm
- Well-Differentiated Liposarcoma
- Often greater than 10cm
- Benign Lipoma
- Homogeneous fat signal
- Well-Differentiated Liposarcoma
- Heterogeneous with non-fat areas
- Benign Lipoma
- Thin (under 2mm) or absent
- Well-Differentiated Liposarcoma
- Thick (over 2mm) nodular
- Benign Lipoma
- None
- Well-Differentiated Liposarcoma
- Present in non-fat components
- Benign Lipoma
- Superficial common
- Well-Differentiated Liposarcoma
- Deep (intramuscular, retroperitoneal)
Histological Diagnosis
- Deep lipoma with atypical imaging features
- Size greater than 5cm with thick septations
- Clinical suspicion of malignancy
- Core needle biopsy (14-16 gauge) adequate for most cases
- MDM2 amplification testing distinguishes atypical lipomatous tumor from lipoma
- Excisional biopsy for small superficial lesions
Imaging: Unusual Locations
Deep lipomas can occur in unexpected locations such as the hand, causing compression symptoms.




Management
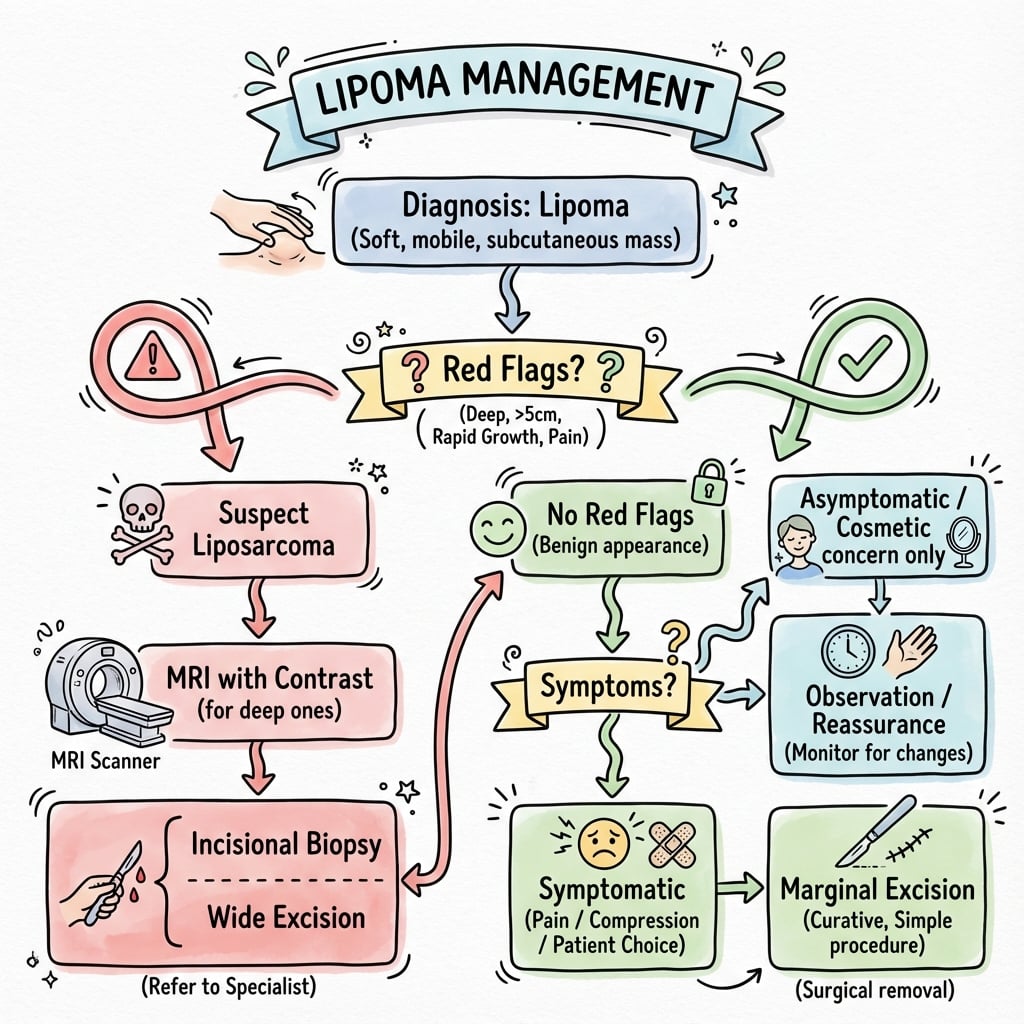
Treatment Algorithm
- Management
- Observation
- Rationale
- Benign natural history, no malignant potential
- Follow-up
- Annual clinical exam or as needed
- Management
- Simple excision
- Rationale
- Curative with low recurrence (under 5%)
- Follow-up
- No routine follow-up needed
- Management
- MRI then excision
- Rationale
- Rule out liposarcoma before surgery
- Follow-up
- Histology confirmation, recurrence monitoring
- Management
- Biopsy then wide excision
- Rationale
- Liposarcoma likely, need margin clearance
- Follow-up
- MDT discussion, oncology referral
Conservative Management
- Asymptomatic superficial lipoma
- Small size (under 5cm)
- Stable over time
- Patient preference
- Annual clinical examination
- Patient education on red flag symptoms (rapid growth, pain)
- Repeat imaging not routinely required unless symptoms change
Surgical Management
Superficial Lipoma Excision
Indications:
- Symptomatic lipoma (pain, cosmetic concern)
- Superficial location
- Size typically under 5cm
Technique:
Surgical Steps
- Directly over the mass or along skin tension lines
- Incision length approximately 50% of tumor diameter
- Dissect to tumor pseudocapsule
- Blunt dissection along capsule plane
- Tumor usually shells out easily
- Minimal bleeding due to avascular plane
- Check for complete excision
- Minimal dead space (lipomas compress)
- Subcuticular closure for cosmesis
Outcomes:
- Recurrence rate less than 5%
- Same-day discharge
- Return to activities within 1-2 weeks
Simple excision remains the treatment of choice for symptomatic superficial lipomas.
Special Considerations
Familial lipomatosis or syndromic:
- Excise symptomatic lesions only
- Genetic counseling if autosomal dominant pattern
- Screen for associated conditions (Gardner syndrome)
Higher recurrence risk:
- Intramuscular and intermuscular types
- Wide excision preferred over enucleation
- Counsel about 20% recurrence despite surgery
Surgical Technique
Superficial Lipoma Excision - Step by Step
Standard Excision Protocol
Position based on lesion location:
- Limb lesions: supine with arm/leg extended
- Back lesions: prone or lateral decubitus
- Ensure adequate lighting and access
Local anesthesia (1% lidocaine with adrenaline):
- Infiltrate around lipoma circumferentially
- Field block for larger lesions
- General anesthesia rarely needed (deep lesions only)
Direct incision over maximum prominence:
- Length approximately 50% of tumor diameter (lipomas compress)
- Follow skin tension lines where possible
- Incise through skin and subcutaneous tissue to capsule
Blunt dissection along pseudocapsule:
- Use finger or blunt instrument
- Lipoma shells out with minimal bleeding
- Maintain capsule integrity (reduces spillage)
- Rarely need sharp dissection
Inspect cavity, achieve hemostasis:
- Minimal dead space naturally (cavity collapses)
- Drain not required for superficial lesions
- Close subcutaneous tissue with absorbable sutures
- Subcuticular or interrupted skin closure
Deep Lipoma Technique Pearls
- Pre-operative MRI mandatory to plan approach
- Identify neurovascular structures before incision
- Consider tourniquet for limb lesions
- Wider exposure than superficial excision
- Aim for 1-2cm margins if liposarcoma possible
- Careful nerve dissection under loupe magnification
- Place drain for large dead space
- Send specimen oriented for margin assessment
SIMPLESurgical Principles for Lipoma Excision
Hook:SIMPLE excision for superficial lipomas - enucleate along pseudocapsule for low recurrence!
Complications
Intraoperative Complications
- Incidence
- Rare (under 1%)
- Prevention
- Hemostasis during dissection
- Management
- Direct pressure, cautery, rarely requires intervention
- Incidence
- 1-2% (higher for deep lipomas)
- Prevention
- Identify nerves preoperatively (MRI), careful dissection
- Management
- Nerve exploration if deficit, neurolysis vs repair
- Incidence
- 5-10% (intramuscular type)
- Prevention
- Wide dissection for infiltrative lesions
- Management
- Re-excision if symptomatic recurrence
Postoperative Complications
- Incidence
- 5-10%
- Risk Factors
- Large dead space, inadequate compression
- Management
- Aspiration, compression dressing, rarely requires drainage
- Incidence
- Under 2%
- Risk Factors
- Poor sterility, diabetes, immunosuppression
- Management
- Antibiotics, drainage if abscess forms
- Incidence
- Under 5% superficial; 15-20% intramuscular
- Risk Factors
- Incomplete excision, infiltrative type
- Management
- Re-excision with wider margins
- Incidence
- Variable
- Risk Factors
- Location, patient factors, surgical technique
- Management
- Scar revision if significant cosmetic concern
Postoperative Care
Standard Recovery Protocol
Postoperative Timeline
Wound care:
- Pressure dressing for 24-48 hours
- Ice application to reduce swelling
- Standard analgesia (paracetamol ± NSAID)
- Limb elevation if applicable
Activity:
- Light activities permitted immediately
- Avoid heavy lifting or stretching wound
- Keep wound dry for 48 hours
- Shower after 48 hours, no baths for 2 weeks
Follow-up:
- Suture removal at 7-14 days (location dependent)
- Check for seroma, hematoma, infection
- Histology results review
- Counsel on prognosis based on final pathology
Return to activities:
- Full activities by 2-4 weeks for superficial
- Sports and heavy work at 4-6 weeks
- Scar massage to optimize cosmesis
- No further follow-up needed if benign confirmed
Specific Considerations
- Postoperative Modification
- Consider drain for 24-48 hours
- Rationale
- Reduce seroma risk
- Postoperative Modification
- Restrict activity for 4 weeks, physio referral
- Rationale
- Muscle healing, prevent hematoma
- Postoperative Modification
- Document neurovascular status postoperatively
- Rationale
- Medicolegal protection, early detection of deficit
- Postoperative Modification
- MDT referral, possible re-excision
- Rationale
- Atypical lipomatous tumor needs wider margins
Postoperative complications are infrequent after superficial lipoma excision but monitoring for seroma and infection should be routine.
Prognosis and Outcomes
Outcome by Location
- Recurrence Rate
- Under 5%
- Complications
- Minimal; seroma, scar
- Prognosis
- Excellent; curative with simple excision
- Recurrence Rate
- 5-10%
- Complications
- Nerve injury risk 1-2%
- Prognosis
- Excellent if benign confirmed; watch for liposarcoma
- Recurrence Rate
- 15-20%
- Complications
- Higher nerve injury, incomplete excision
- Prognosis
- Good but recurrence common; wide excision recommended
Prognostic Factors
Factors associated with higher recurrence:
- Intramuscular or infiltrative subtype
- Incomplete excision (marginal excision for infiltrative lesions)
- Size greater than 10cm
- Deep location with complex anatomy
Superficial lipomas have excellent prognosis with simple excision and recurrence under 5%.
Multiple Lipomas: the Lipomatosis Syndromes
The topic lists "familial lipomatosis", "Madelung disease", "Gardner syndrome" and "Proteus syndrome" among risk factors and devotes a whole viva to the multiple-lipoma patient, but never develops these entities - and recognising them changes surveillance and counselling.
- Familial multiple lipomatosis. Autosomal-dominant development of many (tens to hundreds) discrete, encapsulated subcutaneous lipomas, typically sparing the head and neck, appearing from early adulthood. The lesions are ordinary lipomas; management is selective excision of symptomatic ones only with genetic counselling - the number, not the biology, is the issue.
- Benign symmetric lipomatosis (Madelung disease / Launois-Bensaude). Non-encapsulated, diffuse, symmetric fat deposits around the neck, shoulders and upper trunk ("horse-collar"/Madelung collar), classically in middle-aged men with a history of alcohol excess. Because the fat is unencapsulated and infiltrative it is not simply enucleated; the important hazard is airway and mediastinal compression, so it is managed by debulking/liposuction with airway vigilance. Note this is distinct from Madelung deformity of the wrist - same eponym, unrelated condition.
- Adiposis dolorosa (Dercum disease). Multiple PAINFUL subcutaneous lipomas, usually in peri-/postmenopausal women, often with obesity - the pain (not the mass) dominates and is difficult to treat.
- Syndromic associations that carry cancer/overgrowth risk. Gardner syndrome (a variant of familial adenomatous polyposis / APC) combines lipomas/fibromas, osteomas, epidermoid cysts and desmoids with near-100% colorectal cancer risk - so multiple lipomas plus osteomas/dental anomalies should trigger colonoscopy/genetics. Proteus syndrome and PTEN-hamartoma (Cowden) syndrome cause asymmetric overgrowth and multiple lipomas with their own tumour-surveillance needs.
Q: A patient has multiple lipomas - which syndromes must you consider and why does it matter? A: Familial multiple lipomatosis (AD, many discrete lipomas - excise symptomatic only); benign symmetric lipomatosis / Madelung disease (middle-aged alcoholic men, unencapsulated "horse-collar" neck/shoulder fat - beware airway compression; distinct from Madelung deformity of the wrist); adiposis dolorosa (Dercum) (painful lipomas, peri-menopausal women); and the cancer-linked syndromes - Gardner (FAP/APC) with osteomas/desmoids and near-100% colorectal cancer (triggers colonoscopy/genetics), and Proteus / PTEN-Cowden with overgrowth and tumour risk.
The Benign 'Atypical-Looking' Lipomas: Spindle-Cell and Pleomorphic Variants
The classification tables flag spindle-cell and pleomorphic lipoma as "benign despite cellularity/atypia" and "must exclude liposarcoma", but never develop this diagnostic trap - benign tumours whose alarming histology is classically mistaken for sarcoma.
- A shared, distinctive biology. Spindle-cell and pleomorphic lipoma are two ends of one benign family with a characteristic male predominance (older men) and a posterior-neck/shoulder/upper-back predilection. They share loss of 13q14 (including the RB1 gene) and are typically CD34-positive - a molecular fingerprint quite different from the MDM2/CDK4 amplification (12q13-15) of atypical lipomatous tumour / well-differentiated liposarcoma.
- Why they alarm the pathologist. Spindle-cell lipoma adds bland spindle cells and ropey collagen to mature fat; pleomorphic lipoma adds bizarre, hyperchromatic multinucleated "floret" giant cells. Those floret cells look atypical enough to be mistaken for pleomorphic or well-differentiated liposarcoma, and the cellularity of spindle-cell lipoma can mimic a spindle-cell sarcoma.
- How they are distinguished - and why it matters. The separation is made by the absence of MDM2/CDK4 amplification (and the presence of RB1 loss/CD34), not by the atypia itself. Getting this right matters enormously: these are entirely benign lesions cured by simple marginal excision with essentially no recurrence or metastatic potential - misdiagnosing one as liposarcoma leads to unnecessary wide resection, radiotherapy and surveillance.
Q: A fatty posterior-neck tumour in an older man shows bizarre floret giant cells / cellular spindle areas - is it a sarcoma? A: Not necessarily - this is the classic picture of pleomorphic / spindle-cell lipoma, a benign family (older men, posterior neck/shoulder) characterised by RB1 (13q14) loss and CD34 positivity and, crucially, the absence of MDM2/CDK4 amplification that defines atypical lipomatous tumour/well-differentiated liposarcoma. Despite alarming histology they are cured by simple marginal excision; confirm with MDM2 testing before ever labelling such a lesion malignant.
FATTYMRI Features of Benign Lipoma
Hook:FATTY on MRI means benign - homogeneous fat signal with thin septa and no enhancement!
Guidelines, Registries & Global Practice
Global Epidemiology
Lipoma is the most common soft tissue tumour worldwide, with an estimated incidence of about 1 per 1000 population per year and no consistent geographic or ethnic predilection. Peak presentation is in the 4th to 6th decades with roughly equal sex distribution; about 5-10% of patients have multiple lesions. Atypical lipomatous tumour / well-differentiated liposarcoma is far rarer (a fraction of the roughly 5 soft tissue sarcomas per 100,000/year) and is concentrated in older adults with deep extremity or retroperitoneal masses.
Society Guidance, Side by Side
- Imaging threshold
- Any deep soft-tissue mass, or superficial mass over ~5cm, growing or painful → urgent imaging
- Referral / diagnosis emphasis
- Refer indeterminate fatty masses to a sarcoma diagnostic pathway before excision
- Imaging threshold
- MRI for any deep or large (over 5cm) soft-tissue mass
- Referral / diagnosis emphasis
- Biopsy and management of suspected ALT/sarcoma at a reference sarcoma centre; MDM2 testing for ambiguous cases
- Imaging threshold
- Cross-sectional imaging (MRI) for indeterminate or deep lesions
- Referral / diagnosis emphasis
- Core-needle biopsy and multidisciplinary planning before resection of indeterminate fatty tumours
- Imaging threshold
- Not an imaging guideline — defines pathology
- Referral / diagnosis emphasis
- ALT and well-differentiated liposarcoma are one MDM2-amplified entity; terminology depends on site/resectability
Across bodies the consensus is consistent: a small, superficial, clinically typical lipoma needs neither imaging nor referral, while a deep or large (over 5cm) or growing fatty mass should be imaged and, if indeterminate, biopsied — ideally within a sarcoma service — before any excision. Differences are mainly in pathway structure (centralised sarcoma units in the UK/Europe vs more variable referral in some systems) rather than the underlying clinical logic. There is no dedicated implant or device registry for lipoma, as management is excisional rather than implant-based.
High- vs Limited-Resource Practice
- MRI readily available for deep or large lesions
- MDM2 amplification (FISH or equivalent) to confirm ALT/WDL
- Sarcoma multidisciplinary teams direct biopsy-first management
- Ultrasound may be the only modality; reliance on clinical red flags
- Histology available but molecular MDM2 testing often not
- Lower threshold for excisional biopsy of accessible lesions; refer deep/retroperitoneal masses where possible
Consent and Documentation
- Key risks to consent for: recurrence (under 5% superficial, 15-20% infiltrative intramuscular), nerve injury (1-2% for deep lesions), seroma, scar
- Alternatives: observation versus excision; confirm whether the indication is cosmetic or symptomatic
- Pathology: explain that all excised tissue is sent for histology to confirm the benign diagnosis
- Document examination findings including depth assessment (muscle contraction test)
- Clear indication for imaging (size, location, atypical features)
- Informed consent discussing recurrence risk (varies by location)
- If liposarcoma suspected, document referral to sarcoma MDT
- Failure to investigate deep or large lipomas with imaging (missed liposarcoma)
- Inadequate excision leading to recurrence
- Nerve injury during excision of deep lipomas without documentation of preoperative nerve status
Controversies and Areas of Uncertainty
A confidently benign MRI (homogeneous fat, thin septa, no enhancement) has high negative predictive value, but reader accuracy against MDM2/FISH is only about 73% for indeterminate deep masses. Practice varies on whether an "indeterminate" deep fatty mass should go straight to biopsy or to a sarcoma centre for re-imaging.
"Atypical lipomatous tumour" and "well-differentiated liposarcoma" are the same MDM2-amplified entity; the benign-sounding ALT label is preferred for resectable extremity/trunk lesions, while WDL is used for retroperitoneal disease that cannot be widely excised and carries dedifferentiation risk.
Marginal excision yields roughly 23% recurrence versus 0% for wide resection in extremity ALT, but routine wide resection adds morbidity. The threshold for accepting a planned marginal margin (e.g. near nerves) remains debated and is individualised at MDT.
Liposuction, steroid injection and laser-assisted removal are described for selected superficial cosmetic lipomas, but evidence is limited, recurrence is higher, and no tissue margin or histology is obtained — so they are not used where liposarcoma cannot be excluded.
MCQ Practice Points
Q: What is the key histological feature that distinguishes lipoma from well-differentiated liposarcoma? A: MDM2 amplification - Well-differentiated liposarcoma (atypical lipomatous tumor) shows MDM2 and CDK4 amplification on FISH testing, while lipoma does not. Histologically, lipoma shows mature adipocytes without lipoblasts or significant atypia. Lipoblasts and atypical stromal cells suggest liposarcoma.
Q: What MRI features suggest liposarcoma rather than benign lipoma? A: Thick septations (greater than 2mm), nodular enhancement, heterogeneous signal - Benign lipomas show homogeneous fat signal identical to subcutaneous fat, with thin (less than 2mm) or no septa, and no contrast enhancement. Liposarcomas have thick irregular septa, non-fat soft tissue components, and enhancement.
Q: What is the recurrence rate after simple excision of intramuscular lipoma? A: 15-20% - Intramuscular lipomas have infiltrative growth and significantly higher recurrence than superficial lipomas (under 5%). Wide excision is preferred when feasible, but infiltrative nature makes complete removal difficult. Superficial lipomas have excellent prognosis with simple enucleation.
Q: What is the most common soft tissue tumor in adults? A: Lipoma - Lipomas account for approximately 50% of all benign soft tissue tumors. They are slow-growing, usually superficial, and present as soft mobile masses. Peak incidence is in the 5th-6th decade with equal gender distribution.
Q: What size cutoff prompts imaging for a clinically suspected lipoma? A: Greater than 5cm - Superficial lipomas under 5cm with typical examination findings do not require imaging. Lesions greater than 5cm, deep location, rapid growth, or atypical features warrant MRI to exclude liposarcoma before excision.
Clinical Imaging
Imaging Atlas
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman presents with a 3cm soft, mobile mass on her upper arm that has been present for 2 years. She is concerned about the cosmetic appearance. On examination, you find a non-tender, doughy mass that slips under your fingers and becomes more prominent when she relaxes her arm. What is your assessment and management?”
“A 55-year-old man presents with a 7cm mass in his thigh that has grown over the past 6 months. MRI shows a predominantly fatty mass with some thick septations and small areas of enhancement. What are your concerns and how would you proceed?”
“A 35-year-old man presents with approximately 15 lipomas scattered over his trunk and arms. He has a family history of similar findings in his father. Several are becoming painful. How would you assess and manage this patient?”
Key Epidemiology
- Most common soft tissue tumor (50% of all benign masses)
- Incidence 1:1000 in population
- Peak age 40-60 years, equal gender distribution
- 5-10% are deep (subfascial or intramuscular)
Classification
- Superficial (subcutaneous) = 90% = simple excision
- Deep (subfascial) = higher recurrence = need MRI
- Intramuscular infiltrative = 15-20% recurrence = wide excision
- Variants: spindle cell, pleomorphic (benign despite atypia), angiolipoma (painful)
Red Flags (LARGE Mnemonic)
- Location deep (subfascial/intramuscular)
- Age over 50 (liposarcoma more common)
- Rapidly growing (weeks to months)
- Greater than 5cm (imaging mandatory)
- Enhancement on MRI (suggests malignancy)
Imaging Pearls
- Superficial under 5cm with typical exam = no imaging needed
- MRI mandatory for deep lipomas (rule out liposarcoma)
- Benign features: homogeneous fat signal, thin septa (under 2mm), no enhancement
- Malignant features: thick septa, nodularity, enhancement, heterogeneous signal
Surgical Principles (SIMPLE Mnemonic)
- Superficial = simple excision (enucleation)
- Intramuscular = wide excision preferred
- Margins not critical if confirmed benign
- Pseudocapsule provides dissection plane
- Large/deep needs MRI first
Complications and Outcomes
- Superficial recurrence under 5%, intramuscular 15-20%
- Nerve injury 1-2% for deep lipomas
- Seroma 5-10%, usually managed conservatively
- Malignant transformation less than 1% (extremely rare)
Evidence Base and Key Studies
Distribution of Benign Soft-Tissue Tumours (AFIP Referral Series)
- 18,677 benign mesenchymal lesions from a 10-year AFIP consultation archive
- Lipoma and lipoma variants were the single most common diagnostic category (16%)
- Roughly two-thirds of benign soft-tissue tumours fall into seven diagnostic groups
- Prevalence varies markedly with patient age and anatomical location
MRI of 126 Consecutive Fatty Masses: Lipoma vs Well-Differentiated Liposarcoma
- MRI was 100% sensitive and 100% NPV for detecting well-differentiated liposarcoma
- MRI was 100% specific for the diagnosis of simple lipoma
- But positive predictive value was only 38% — most 'suspicious' masses were benign
- 64% of lesions called suspicious for liposarcoma were actually benign lipoma variants