Frond-Like Fatty Synovial Proliferation
- LIPOMA ARBORESCENS is a rare BENIGN intra-articular lesion characterised by VILLOUS (frond-like, 'tree-like'/arborescent) proliferation of MATURE ADIPOSE tissue that REPLACES the synovial lining; it is best regarded as a reactive/benign change rather than a true lipomatous neoplasm.
- It MOST COMMONLY affects the KNEE - particularly the SUPRAPATELLAR POUCH - and presents with chronic, usually PAINLESS, joint SWELLING with a recurrent EFFUSION (sometimes with clicking, intermittent swelling or mild discomfort), typically without redness or warmth.
- It is frequently ASSOCIATED with CHRONIC synovial IRRITATION or INFLAMMATION - osteoarthritis, rheumatoid arthritis, or prior trauma - supporting a reactive aetiology, although a primary/idiopathic form also occurs; recognising the association prompts attention to any underlying joint disease.
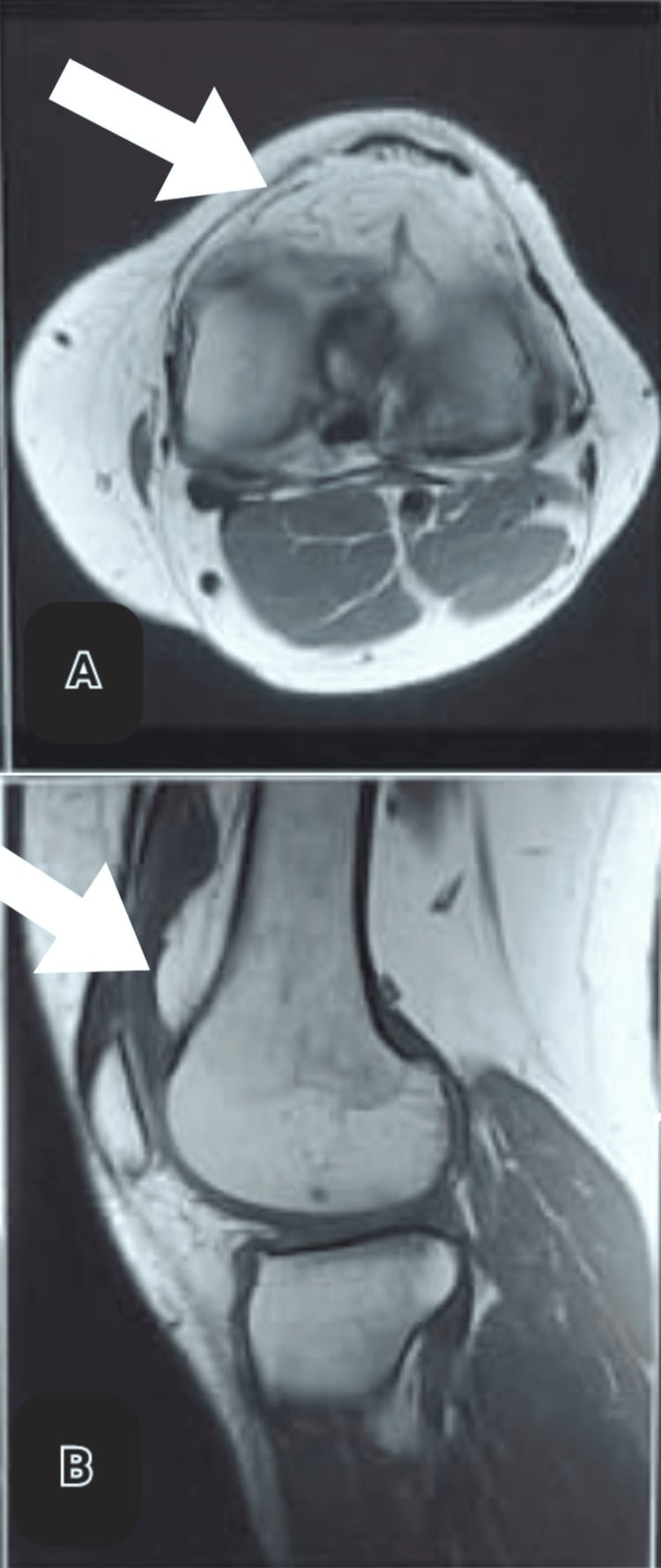
- MRI is the GOLD STANDARD for diagnosis and is near-pathognomonic: it shows FROND-LIKE synovial projections that follow FAT signal on all sequences (hyperintense on T1-weighted images) and SUPPRESS on fat-saturated sequences, accompanied by a joint effusion - this fatty frond pattern is the key.
- The DIFFERENTIAL of a frond-like/proliferative synovial process includes PIGMENTED VILLONODULAR SYNOVITIS (PVNS - haemosiderin, blooming on gradient-echo MRI, not fatty) and SYNOVIAL (osteo)CHONDROMATOSIS (cartilaginous/calcified loose bodies) - the FAT signal distinguishes lipoma arborescens from these.
- MANAGEMENT is SYNOVECTOMY (open or arthroscopic), the treatment of choice; coexisting joint pathology (e.g. osteoarthritis) is addressed in the SAME single-stage procedure, and a symptomatic effusion is relieved by removing the abnormal synovium.
- KNOW HOW THIN THE OUTCOME EVIDENCE ACTUALLY IS. The best available synthesis is a systematic review of the UPPER LIMB: 21 studies reporting 22 lesions in just 21 PATIENTS, mean age 48.5 years. All had satisfactory outcomes after excision and synovectomy with NO recurrences - but at a mean follow-up of only 21 MONTHS, with some patients followed for as little as 2 MONTHS, and the authors state plainly that there are NO evidence-based guidelines and that LONG-TERM outcome data are UNAVAILABLE. So 'excellent outcome, low recurrence' is a fair summary of short-term series, not a durable guarantee - and no comparable synthesis exists for the KNEE, which is the joint most often affected.
- SYNOVECTOMY IS NOT RISK-FREE. In that review one of the 22 procedures was complicated by postoperative CELLULITIS (4.55 percent). With a benign, often painless lesion, the operation's morbidity belongs in the consent discussion rather than being presented as a procedure with only upside.
- “Lipoma arborescens = benign VILLOUS frond-like ('tree-like') proliferation of MATURE FAT replacing the synovium; commonest in the KNEE (suprapatellar pouch). Chronic, usually PAINLESS swelling + effusion.
- “MRI is the gold standard/near-pathognomonic: frond-like synovial projections of FAT signal (T1-bright) that SUPPRESS on fat-sat, with effusion. Often associated with chronic synovial irritation (OA/RA/trauma).
- “Differential: PVNS (haemosiderin, blooms on gradient-echo) and synovial chondromatosis (loose bodies) - the FAT signal distinguishes lipoma arborescens. Treatment = SYNOVECTOMY, with coexisting joint pathology addressed in the same single-stage procedure.
- “Qualify the outcome claim: the best synthesis is 21 UPPER-LIMB patients with NO recurrences but a mean follow-up of only 21 MONTHS (as short as 2), and the authors say long-term data are unavailable and no guidelines exist. One of 22 procedures (4.55%) developed cellulitis. No cohort reports knee-specific outcomes.
Chronic, usually painless knee swelling + effusion with frond-like synovial projections of fat signal on MRI (T1-bright, suppress on fat-sat) = lipoma arborescens.
PVNS = haemosiderin (blooms on gradient-echo), not fatty. Synovial chondromatosis = cartilaginous/ calcified loose bodies. The fat signal is the discriminator.
Imaging Beyond MRI, and the Solitary-Lipoma Distinction
- Radiograph. Usually normal or shows only a nonspecific joint effusion / soft-tissue fullness, and may reveal underlying osteoarthritis.
- Ultrasound. A useful first-line/bedside test: a frond-like, hyperechoic synovial mass with an effusion that characteristically does not compress or change shape with probe pressure (the fronds sway within the fluid).
- CT. Shows fat-attenuation intra-articular fronds - confirming the fatty nature where MRI is unavailable.
- MRI (confirmatory). The frond-like projections follow fat on every sequence (T1-bright) and suppress on fat-saturated sequences, with an effusion - near-pathognomonic.
- Distinguish from a solitary intra-articular lipoma. A true intra-articular lipoma is a single, encapsulated fatty mass; lipoma arborescens is a diffuse, villous fatty replacement of the synovium - both are fat-signal, but the architecture differs.
Q: What do the non-MRI modalities show in lipoma arborescens, and how does it differ from a solitary intra-articular lipoma?
A: Radiographs are usually normal or show a nonspecific effusion (and any underlying OA); ultrasound shows a frond-like hyperechoic synovial mass with an effusion that does not compress with probe pressure; CT shows fat-attenuation fronds. MRI is confirmatory (fat-signal fronds suppressing on fat-sat). It differs from a solitary intra-articular lipoma - a single encapsulated fatty mass - whereas lipoma arborescens is a diffuse villous fatty replacement of the synovium.
Features, Imaging & Differential
Lipoma arborescens is a benign intra-articular villous (frond-like/'tree-like') proliferation of mature fat that replaces the synovial lining - a reactive change rather than a true neoplasm. It most often affects the knee (especially the suprapatellar pouch) with chronic, usually painless swelling and a recurrent effusion, and is frequently associated with chronic synovial irritation (osteoarthritis, rheumatoid arthritis, trauma). MRI is the gold standard and near-pathognomonic: frond-like synovial projections of fat signal (T1-hyperintense) that suppress on fat-saturated sequences, with an effusion. The fat signal distinguishes it from PVNS (haemosiderin, blooms on gradient-echo) and synovial chondromatosis (loose bodies).
- Key MRI feature
- Frond-like FAT-signal synovial projections (suppress on fat-sat)
- Nature
- Benign fatty synovial proliferation
- Key MRI feature
- Haemosiderin - blooming on gradient-echo (low signal)
- Nature
- Benign but locally aggressive proliferative synovitis
- Key MRI feature
- Cartilaginous/calcified loose bodies
- Nature
- Benign cartilaginous metaplasia
Management
- Diagnosis: MRI (frond-like fat-signal synovial projections + effusion) is usually diagnostic; histology confirms mature fat replacing synovium.
- Treatment: synovectomy (open or arthroscopic) - the treatment of choice, with good short-term results and no recurrences in the published upper-limb review, though its mean follow-up was only 21 months and long-term data are unavailable.
- Address coexisting joint pathology (e.g. osteoarthritis, inflammatory arthritis) in the same single-stage procedure - this lesion is usually secondary.
- Consent for the morbidity too: 4.55 percent developed postoperative cellulitis in that review, which matters when operating on a benign and often painless lesion.
- Outcome: symptoms (swelling/effusion) typically resolve after complete excision.
The lesions this must be told apart from have their own pages: PVNS, whose haemosiderin blooms on gradient-echo, and synovial chondromatosis, which produces loose bodies. The fatty lesions it sits alongside are the solitary lipoma and, as the malignant lesion excluded by the absence of lipoblasts and atypia, liposarcoma. Because the secondary form usually accompanies degenerative disease, knee osteoarthritis is often the condition actually being treated alongside it.
The diagnosis of lipoma arborescens is essentially made on MRI, and the key is to recognise the fat signal: the frond-like synovial projections follow fat on all sequences (bright on T1) and suppress on fat-saturated sequences, which, with a joint effusion in a chronically swollen knee, is near-pathognomonic. This recognition matters because the main mimics behave and are treated differently: pigmented villonodular synovitis contains haemosiderin and shows characteristic blooming (low signal) on gradient-echo sequences rather than fat, and is locally aggressive; synovial chondromatosis produces cartilaginous or calcified loose bodies. Correctly identifying lipoma arborescens as a benign fatty synovial proliferation avoids both over-treatment and mis-treatment, while also prompting a look for any associated chronic joint disease (osteoarthritis, rheumatoid arthritis) that may underlie it. The treatment of choice is synovectomy, open or arthroscopic, which when complete resolves the effusion and swelling, with no recurrences reported in the published upper-limb review - though that covered 21 patients at a mean follow-up of 21 months, and one in twenty-two developed a postoperative cellulitis.
Histology, the Name, and Primary versus Secondary
- The name. "Arborescens" is Latin for "tree-like" - describing the branching, frond-like villous synovial projections.
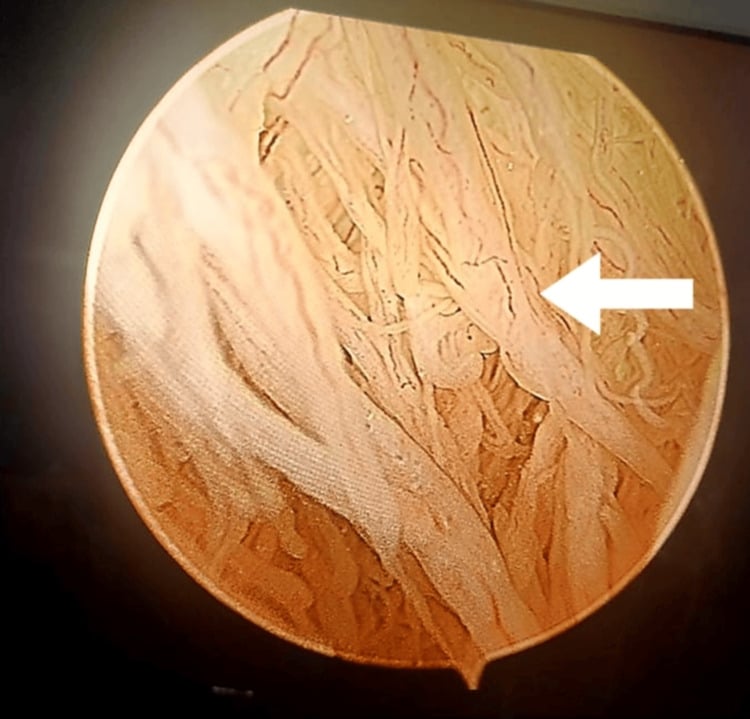
- Histology. The subsynovial connective tissue is diffusely expanded by mature adipocytes beneath a hyperplastic synovial lining, giving the villous/papillary architecture, usually with a chronic inflammatory infiltrate. Crucially there are no lipoblasts and no cytological atypia - which, with the diffuse villous (not encapsulated) pattern, distinguishes it from a liposarcoma and from a solitary intra-articular lipoma.
- Primary versus secondary (Hallel). It is classified as primary/idiopathic (isolated, often a single joint, in younger patients, with no underlying joint disease) or secondary (the commoner form, associated with a chronic joint disorder - osteoarthritis, rheumatoid or other inflammatory arthritis, chronic trauma, sometimes diabetes) - supporting a reactive rather than neoplastic origin.
Q: What does the histology of lipoma arborescens show, and how is it classified?
A: The subsynovial tissue is diffusely infiltrated by mature adipocytes beneath a hyperplastic synovial lining, giving villous ("arborescent"/tree-like) fronds, with a chronic inflammatory infiltrate but no lipoblasts or atypia - distinguishing it from liposarcoma and a solitary intra-articular lipoma. It is classified (Hallel) as primary/idiopathic (isolated, younger, no joint disease) or secondary (commoner, with a chronic joint disorder - OA/RA/trauma), consistent with a reactive origin.
How Much Does 'Excellent Outcome, Low Recurrence' Actually Rest On?
The claim that synovectomy gives excellent results with low recurrence is repeated everywhere, and the best synthesis behind it is a systematic review of 21 studies reporting 22 lesions in 21 patients - all in the upper limb, mean age 48.5 years. Every patient had a satisfactory outcome after open or arthroscopic excision and synovectomy with no recurrence, which is genuinely reassuring. But the mean follow-up was only 21 months, the range extended down to 2 months, and the authors state explicitly that no evidence-based guidelines exist and that long-term outcome data are unavailable. No comparable synthesis exists for the knee - the joint this lesion most often affects. So the defensible statement is that short-term results after complete excision are good, not that recurrence has been shown to be low over time.
One of the 22 procedures in that review was complicated by postoperative cellulitis - 4.55 percent. For a benign, frequently painless lesion, that matters: the operation is being offered to relieve swelling and effusion, not to treat a dangerous disease, so its morbidity belongs in the consent conversation rather than being left out of a list of excellent outcomes.
The same review found that concomitant intra-articular pathology was treated in a single-stage procedure alongside the synovectomy. Since this lesion is so often secondary to osteoarthritis, inflammatory arthritis or old trauma, planning to address the underlying joint at the same sitting - rather than treating the fatty synovium in isolation - is the practical lesson.
Mnemonics & Memory Aids
FRONDS
Hook:FRONDS: Fat-signal, aRborescent fronds, Often chronic irritation, kNee (suprapatellar), Differential PVNS/chondromatosis, Synovectomy (short-term evidence only).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has chronic, painless knee swelling with a recurrent effusion, and MRI shows frond-like fatty projections from the synovium. What is the diagnosis and treatment?”
What it is
- Benign villous (frond-like/'tree-like') proliferation of mature fat replacing synovium
- Reactive change, not a true neoplasm
- Commonest in the knee (suprapatellar pouch)
Presentation & association
- Chronic, usually painless joint swelling with recurrent effusion
- Often associated with chronic synovial irritation (OA, RA, trauma)
- Primary/idiopathic form also occurs
Imaging & differential
- MRI gold standard: frond-like fat-signal projections (T1-bright, suppress on fat-sat) + effusion
- PVNS: haemosiderin, blooming on gradient-echo (not fatty)
- Synovial chondromatosis: cartilaginous/calcified loose bodies
Management
- Synovectomy (open or arthroscopic) - treatment of choice
- No recurrences in the published review, but only 21 upper-limb patients at a mean 21 months' follow-up
- 4.55 percent postoperative cellulitis - consent for the morbidity
- Address associated joint pathology in the same single-stage procedure
Evidence & Key Studies
Lipoma arborescens: a rare synovial lesion unveiled by radiologic imaging
- Lipoma arborescens is a rare benign synovial lesion characterised by villous proliferation of mature adipose tissue within the joint lining, most commonly affecting the knee, and is often linked to chronic irritation or inflammation of the synovium.
- MRI is the gold standard for diagnosis and differentiation, showing characteristic frond-like fatty projections arising from the synovial lining (hyperintense on T1, suppressed on fat-saturated sequences); it should be distinguished from PVNS and synovial chondromatosis.
- Synovectomy is described as the treatment of choice with good outcomes when the lesion is completely excised, and histology confirms villous synovial proliferation with mature adipocytes - though as a single case illustration this report cannot establish recurrence rates or comparative efficacy.
Surgical management of upper limb lipoma arborescens: a systematic review
- PRISMA systematic review of PubMed, Scopus and the Virtual Health Library to September 2021, restricted to histologically confirmed upper-limb lipoma arborescens treated surgically: 21 studies reporting 22 lesions in 21 patients, mean age 48.48 years (range 22 to 77). The authors note that current evidence rests mainly on case reports and case series and that no guidelines exist.
- Open or arthroscopic excision with synovectomy was the usual procedure, and concomitant lesions were treated in a single-stage operation. All patients had satisfactory outcomes with no recurrence, but at a mean follow-up of only 21.14 months (range 2 to 60).
- One patient (4.55 percent) developed postoperative cellulitis. The authors conclude that long-term outcome data are unavailable - so the absence of recurrence in this review describes short-term follow-up in 21 upper-limb patients and cannot be read as a durable recurrence rate, still less one for the knee.
The nature of lipoma arborescens (a benign villous proliferation of mature adipose tissue in the joint lining, commonest in the knee, often linked to chronic synovial irritation/inflammation), MRI as the gold standard with its characteristic frond-like fatty projections (T1-hyperintense, fat-suppressing), the differential from PVNS and synovial chondromatosis, and synovectomy as the treatment of choice come from the cited Davra report, which is a single case illustration and cannot establish outcomes. The recurrence, follow-up, complication and single-stage findings come from the Kalifis systematic review, which covers 21 upper-limb patients with a mean follow-up of 21 months and whose authors state that long-term outcome data are unavailable and no guidelines exist. The suprapatellar-pouch predilection, the painless chronic-swelling presentation and the Hallel primary-versus-secondary classification are standard, well-established teaching. No study gives an incidence or prevalence for this lesion, no cohort reports outcomes for the knee specifically, no trial compares arthroscopic with open synovectomy or either with observation, and no surveillance interval has been validated - so none is quoted here.