Malignant Adipocytic Tumor | Most Common Adult Sarcoma | Variable Prognosis by Subtype
- Most common soft tissue sarcoma in adults (24% of all sarcomas)
- Well-differentiated liposarcoma (atypical lipomatous tumor) has excellent prognosis in extremity
- MDM2 amplification distinguishes well-differentiated liposarcoma from lipoma
- Dedifferentiated liposarcoma has high metastatic potential (15-30%)
- Wide excision with negative margins is cornerstone of treatment
- “Atypical lipomatous tumor and well-differentiated liposarcoma are same entity, different names by location
- “Myxoid liposarcoma is radiosensitive unlike other sarcomas
- “Retroperitoneal liposarcomas have worse prognosis than extremity due to margins
- “Round cell variant of myxoid has worse prognosis and higher metastatic rate
Clinical Imaging
Imaging Atlas



Well-differentiated (best), myxoid (intermediate), dedifferentiated/pleomorphic (worst) - Subtype determines prognosis and treatment. Five-year survival ranges from 80% for well-differentiated extremity lesions to 30% for pleomorphic.
MDM2 amplification for well-differentiated, FUS-DDIT3 fusion for myxoid - Molecular testing is diagnostic. MDM2 positive distinguishes atypical lipomatous tumor from benign lipoma. FUS-DDIT3 confirms myxoid subtype.
Wide excision with 1-2cm margins - Margin status is most important prognostic factor. Positive margins lead to 30-50% local recurrence. Re-excision mandatory if margins positive.
Radiation for high-grade, chemotherapy for dedifferentiated/pleomorphic - Myxoid liposarcoma is uniquely radiosensitive. Doxorubicin-based chemotherapy for high-grade subtypes.
WDMPLiposarcoma WHO Subtypes (Prognosis Order)
Hook:WDMP - prognosis goes from Well (best) to Pleomorphic (worst) in alphabetical order!
Overview and Epidemiology
Liposarcoma is the most common soft tissue sarcoma in adults, accounting for 20-24% of all adult sarcomas. Unlike lipoma (benign adipocytic tumor), liposarcoma demonstrates malignant potential with capacity for local recurrence and distant metastasis. The tumor arises from primitive mesenchymal cells rather than mature adipocytes, explaining its variable differentiation and behavior.
Atypical lipomatous tumor (ALT) versus well-differentiated liposarcoma (WDLS): These are the SAME entity. Extremity/superficial lesions are called ALT due to negligible metastatic potential. Deep-seated retroperitoneal lesions are called WDLS due to higher recurrence risk from incomplete excision. Both show MDM2 amplification.
- Age: Peak 50-65 years (median 55)
- Gender: Slight male predominance (M:F 1.2:1)
- Location: 75% extremity or trunk, 25% retroperitoneum
- Hereditary: Rare Li-Fraumeni syndrome cases
- Extremity: 60% (thigh most common)
- Retroperitoneum: 20% (worse prognosis)
- Trunk: 15%
- Head/neck: 5% (rare)
Pathophysiology and Anatomy
Anatomical Distribution
Liposarcomas arise from mesenchymal precursors and can develop in any location with adipose tissue. Location significantly impacts surgical approach and prognosis.
| Location | Frequency | Anatomical Considerations | Prognosis Impact |
|---|---|---|---|
| Thigh (anterior/posterior) | 40% | Deep compartments, femoral vessels/nerve proximity | Best prognosis, limb salvage greater than 95% |
| Retroperitoneum | 20% | Large at diagnosis, organ displacement, IVC/aorta adjacent | Worse prognosis, 40% recurrence |
| Trunk/shoulder | 15% | Variable depth, chest/abdominal wall | Intermediate prognosis |
| Arm/forearm | 15% | Smaller compartments, neurovascular proximity | Good, smaller tumors |
| Head/neck | 5% | Rare, complex anatomy | Variable by site |
Tumor Biology
- Arises from mesenchymal stem cells (not mature adipocytes)
- Clonal chromosomal aberrations (MDM2, FUS-DDIT3)
- Variable differentiation determines subtype
- Can dedifferentiate over time (worse prognosis)
- Respects fascial boundaries initially
- Intramuscular spread along muscle fibers
- Eventually breaks through compartments
- Retroperitoneal tumors infiltrate adjacent organs
Classification Systems
WHO 2020 Classification of Liposarcoma
| Subtype | Frequency | Key Features | Molecular Marker | 5-Year Survival |
|---|---|---|---|---|
| Well-differentiated (ALT) | 40-45% | Mature fat with atypical cells, thick septa | MDM2/CDK4 amplification | 80-90% (extremity) |
| Dedifferentiated | 10-15% | High-grade non-lipogenic within well-diff | MDM2+ with high-grade areas | 30-40% |
| Myxoid | 25-30% | Myxoid matrix, lipoblasts, arborizing vessels | FUS-DDIT3 fusion | 70% |
| Round cell (high-grade myxoid) | 5% | greater than 5% round cells in myxoid background | FUS-DDIT3 fusion | 40% |
| Pleomorphic | 5-10% | High-grade, pleomorphic lipoblasts | Complex karyotype | 30% |
Classification determines treatment approach and prognosis.
Histology and Molecular Pathology
WHO Classification (2020)
The WHO classifies liposarcoma into four main subtypes based on histological and molecular features. This classification has direct prognostic and therapeutic implications.
| Subtype | Frequency | Molecular Marker | 5-Year Survival |
|---|---|---|---|
| Well-differentiated (ALT) | 40-45% | MDM2/CDK4 amplification | 80-90% (extremity) |
| Myxoid/Round cell | 30-35% | FUS-DDIT3 fusion (t12;16) | 70% (myxoid), 30% (round cell) |
| Dedifferentiated | 10-15% | MDM2+ with high-grade areas | 30-40% |
| Pleomorphic | 5-10% | Complex karyotype, no specific marker | 30% |
Molecular Diagnostics
Well-Differentiated Liposarcoma
MDM2 amplification is the diagnostic hallmark of well-differentiated and dedifferentiated liposarcoma.
Testing methods:
- FISH (fluorescence in situ hybridization): Gold standard
- Immunohistochemistry: Screening tool (MDM2 and CDK4 overexpression)
- Next-generation sequencing: Can detect amplification
Clinical significance:
- Positive MDM2 confirms diagnosis (distinguishes from lipoma)
- Negative MDM2 excludes well-differentiated/dedifferentiated subtype
- Helps guide surgical planning (wide margins required)
MDM2 testing is essential for any deep or large fatty tumor to distinguish benign lipoma from atypical lipomatous tumor.
Diagnostic errors to avoid:
- Pleomorphic lipoma (benign with bizarre nuclei) versus pleomorphic liposarcoma: MDM2 negative in benign variant
- Spindle cell lipoma versus spindle cell liposarcoma: Clinical and molecular distinction essential
- Myxoid liposarcoma versus myxofibrosarcoma: FUS-DDIT3 testing differentiates
- Well-differentiated liposarcoma versus lipoma: MDM2 amplification is key
MFMolecular Markers for Liposarcoma Diagnosis
Hook:MF = Molecular Fingerprints - MDM2 for Well-differentiated, FUS for myxoiD!
Differential Diagnosis
A fatty or deep soft tissue mass has a broad differential. The clinical task is to separate benign lesions safely managed by observation or simple excision from malignancies requiring formal staging and wide excision. Molecular testing (MDM2/CDK4, FUS-DDIT3) resolves most difficult cases.
| Lesion | Distinguishing Features | Imaging / Molecular Clue | Why It Matters |
|---|---|---|---|
| Benign lipoma | Soft, mobile, often superficial, stable size | Uniform fat signal, thin septa (under 2mm), MDM2 negative | Simple excision adequate; do NOT over-treat |
| Well-differentiated liposarcoma / ALT | Deep, large, thick septa or nodules in fat | Thick enhancing septa, nodular non-fatty areas, MDM2/CDK4 amplified | Needs wide excision and surveillance for dedifferentiation |
| Myxoid liposarcoma | Thigh, younger adults, can mimic a cyst | High T2 signal, fluid-like but enhances; FUS-DDIT3 fusion | Radiosensitive; can metastasise to bone/soft tissue, not just lung |
| Myxofibrosarcoma | Elderly, superficial, infiltrative 'tails' | Myxoid signal but FUS-DDIT3 negative; curvilinear tails on MRI | High local recurrence; needs generous margins |
| Spindle cell / pleomorphic lipoma (benign) | Posterior neck, shoulder, back in older men | CD34 positive, RB1 loss, MDM2 negative | Benign mimic of pleomorphic liposarcoma |
| Undifferentiated pleomorphic sarcoma | Deep, rapidly enlarging high-grade mass | No lipogenic differentiation, complex karyotype | Overlaps with pleomorphic/dedifferentiated liposarcoma |
When a deep fatty tumour cannot be confidently called benign on imaging, MDM2 amplification by FISH is the decisive test: positive supports well-differentiated/dedifferentiated liposarcoma, negative argues for lipoma or another mimic. CDK4 co-amplification adds specificity.
Clinical Assessment
History
- Painless mass: Most common (70-80%)
- Growing mass: Noticed over months
- Pain: 20-30% (compression of nerves/vessels)
- Functional impairment: Large masses affecting movement
- Rapid growth: Over weeks to months
- Systemic symptoms: Weight loss, malaise
- Large size: Greater than 10cm
- Deep location: Retroperitoneal or intramuscular
Physical Examination
Examination Approach
Observe:
- Size (measure in cm)
- Location (superficial vs deep)
- Skin changes (rare except for large tumors)
- Asymmetry of limb
Assess:
- Consistency (firm to hard; unlike soft lipomas)
- Mobility (deep lesions fixed to fascia/muscle)
- Tenderness (usually non-tender)
- Fixation to skin or deep structures
Document:
- Distal pulses
- Sensory and motor function
- Nerve compression signs
- Vascular compression (venous congestion)
Palpate regional lymph nodes (nodal metastasis rare in sarcomas but check baseline)
Lymph node involvement uncommon in liposarcoma (less than 5% except for myxoid round cell variant).
Investigations and Staging
Imaging Protocol
MRI (Investigation of Choice)
MRI is the gold standard for local staging of soft tissue sarcomas.
Protocol:
- T1-weighted: Anatomical detail, fat signal
- T2-weighted with fat suppression: Tumor extent, edema
- Post-contrast T1 with fat suppression: Enhancement pattern
- Include entire muscle compartment plus joint above and below
Features of Liposarcoma:
| Subtype | MRI Characteristics |
|---|---|
| Well-differentiated | Predominantly fat signal with thick septa (greater than 2mm), nodular areas |
| Dedifferentiated | Mixed fat and solid enhancing areas (high-grade component) |
| Myxoid | High T2 signal (myxoid matrix), minimal fat, lacy enhancement |
| Pleomorphic | Heterogeneous, minimal fat, irregular enhancement, necrosis |
MRI guides biopsy planning and surgical approach.
Biopsy
Critical rules:
- Core needle biopsy (14-16 gauge) is preferred over incisional biopsy
- Biopsy tract must be excisable at definitive surgery (plan incision)
- Avoid contaminating neurovascular structures or adjacent compartments
- Request MDM2 or FUS-DDIT3 testing on biopsy specimen
- Never perform excisional biopsy for suspected sarcoma (risks seeding, inadequate margins)
Referral to sarcoma center before biopsy is ideal for optimal outcomes.
Staging System
| Stage | Grade | Size/Depth | 5-Year Survival |
|---|---|---|---|
| IA | Low (G1) | Superficial or deep, any size | 90% |
| IB | Low (G1) | Deep, greater than 5cm | 80% |
| II | Low (G1) | Deep, greater than 10cm | 75% |
| IIIA | High (G2-3) | Superficial/deep, under 5cm | 60% |
| IIIB | High (G2-3) | Deep, 5-10cm or greater than 10cm | 50% |
| IV | Any | Metastatic disease | 15-20% |
MBCPMLiposarcoma Staging Workup
Hook:MBCPM = Must Be Checked Pre-Management - complete staging before surgery!
Management
Treatment Algorithm
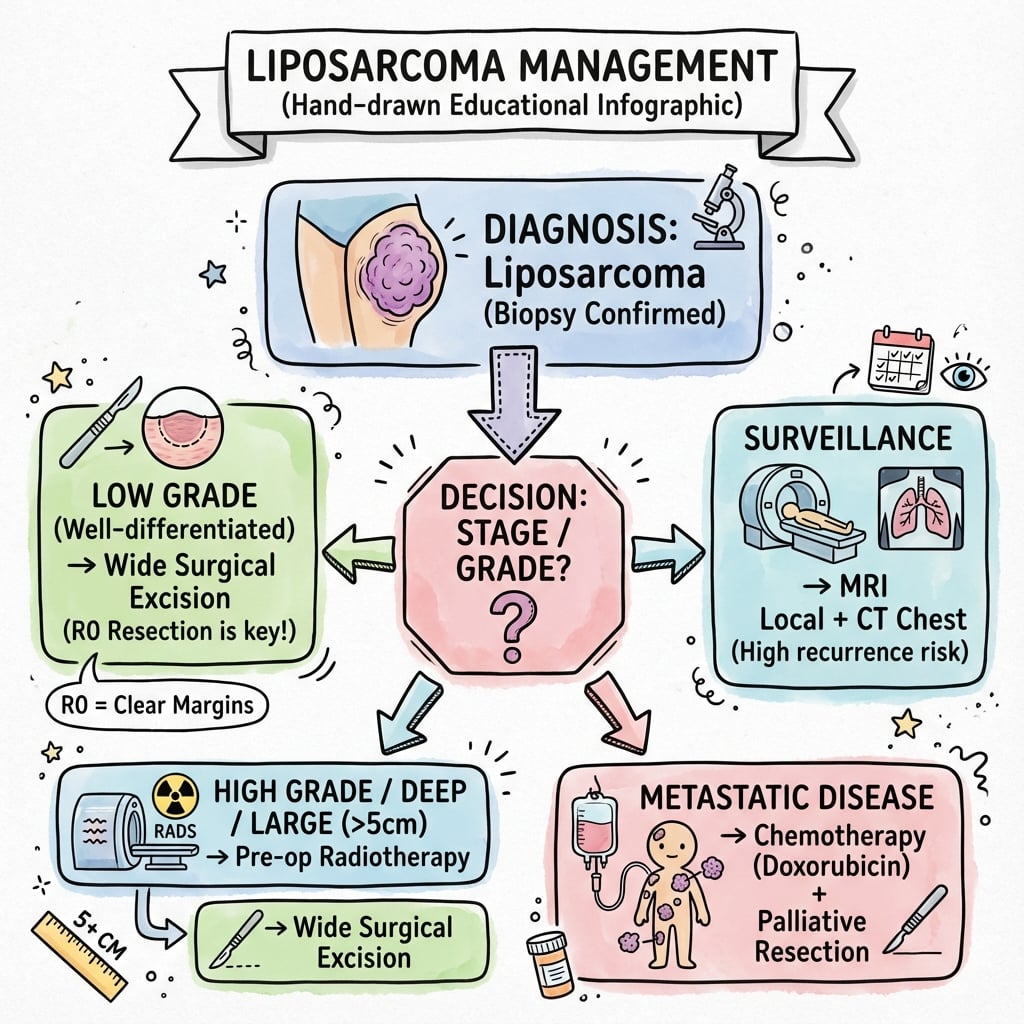
| Subtype/Stage | Primary Treatment | Adjuvant Therapy | Prognosis |
|---|---|---|---|
| Well-differentiated, extremity | Wide excision (1-2cm margins) | None (low grade) | Excellent (80-90% 5-year) |
| Myxoid, localized | Wide excision | Radiation (radiosensitive) | Good (70% 5-year) |
| Dedifferentiated/pleomorphic | Wide excision | Radiation + chemotherapy | Poor (30-40% 5-year) |
| Retroperitoneal (any grade) | Complete resection + organs | Radiation (consider preop) | Variable (50% 5-year) |
Surgical Management
Extremity Liposarcoma Resection
Goal: Complete excision with negative margins (R0 resection)
Margin definition:
- Negative margin: Greater than 1mm clear tissue
- Wide margin: 1-2cm of normal tissue (goal for extremity sarcomas)
- Marginal: Tumor capsule or pseudocapsule (inadequate)
- Intralesional: Tumor violation (unacceptable)
Surgical Principles
- Review MRI with radiology and surgical team
- Identify neurovascular structures at risk
- Plan incision along biopsy tract (excise entire tract)
- Mark margins on skin based on MRI
- Excise biopsy tract en bloc with tumor
- Dissect along fascial planes (preserve compartment barriers)
- Achieve 1-2cm margin in all dimensions if feasible
- Protect critical neurovascular structures (accept closer margins if necessary)
- Remove tumor with surrounding cuff of normal tissue
- Mark specimen margins with sutures for pathologist
- Send frozen section if margin status uncertain
- Document neurovascular preservation
- Soft tissue coverage: Primary closure, flap, skin graft
- Functional reconstruction: Tendon transfers if muscle resected
- Drain placement for large dead spaces
- Limb salvage in over 95% of extremity sarcomas
Reconstruction planning is essential before resection.
Adjuvant Radiotherapy
| Indication | Timing | Dose | Benefit |
|---|---|---|---|
| High-grade extremity sarcoma | Preoperative or postoperative | 50 Gy (preop) or 60-66 Gy (postop) | Reduces local recurrence from 30% to 10% |
| Myxoid liposarcoma | Postoperative (radiosensitive) | 50-60 Gy | Excellent local control, superior to other subtypes |
| Positive margins (R1) | Postoperative | 66 Gy to margin | Improves local control but re-excision preferred |
| Retroperitoneal sarcoma | Preoperative (consider) | 50-50.4 Gy | Controversial benefit, reduces tumor size |
Myxoid liposarcoma is uniquely radiosensitive among soft tissue sarcomas. Radiotherapy produces excellent local control and may achieve near-complete pathological response. This is attributed to FUS-DDIT3 fusion affecting DNA repair mechanisms. Radiation is standard adjuvant therapy for myxoid subtype.
Chemotherapy
Indications:
- High-grade liposarcoma (dedifferentiated, pleomorphic, round cell myxoid)
- Metastatic disease
- Neoadjuvant for large/unresectable tumors
Regimens:
- Doxorubicin + ifosfamide: Standard first-line (response rate 25-30%)
- Trabectedin: Active in myxoid liposarcoma (response rate 50% for myxoid subtype)
- Eribulin: Second-line option for dedifferentiated liposarcoma
Well-differentiated liposarcoma does not respond to chemotherapy.
Prognosis and Surveillance
Prognostic Factors
| Factor | Favorable | Unfavorable |
|---|---|---|
| Histological subtype | Well-differentiated, myxoid | Dedifferentiated, pleomorphic, round cell |
| Tumor size | Less than 5cm | Greater than 10cm |
| Tumor depth | Superficial | Deep (subfascial) |
| Margin status | Negative (R0) | Positive (R1/R2) |
| Location | Extremity | Retroperitoneum |
| Grade | Low (G1) | High (G2-3) |
Surveillance Protocol
Follow-Up Schedule
- Clinical examination
- MRI of primary site every 6 months
- CT chest every 6 months (high-grade subtypes)
- Clinical examination
- MRI primary site annually
- CT chest annually (high-grade subtypes)
- Clinical examination
- Imaging as clinically indicated
- Well-differentiated may recur late (10+ years)
Surveillance continues indefinitely for well-differentiated/dedifferentiated due to late recurrence risk.
Surgical Technique
Extremity Liposarcoma Excision - Step by Step
Surgical Protocol for Wide Excision
Preparation:
- Review MRI with surgical and radiology team
- Mark tumor extent on skin with MRI guidance
- Identify biopsy tract for en bloc excision
- Plan incision, reconstruction, and contingency for vessels/nerves
Setup:
- Position for optimal access to entire tumor
- Tourniquet for extremity lesions (bloodless field)
- Wide skin flaps to visualize compartment fully
- Identify and protect major neurovascular structures
Excision:
- Excise biopsy tract with tumor (contaminated tissue)
- Dissect along fascial planes with 1-2cm margins
- Accept closer margins on critical structures (vessels, nerves, bone)
- Frozen section if margin uncertain (intraoperative pathology)
Orientation and submission:
- Orient specimen with sutures (superior, lateral, deep)
- Ink margins if concerned about specific areas
- Send to pathology fresh for molecular testing if needed
- Document margin distances from critical structures
Closure options:
- Primary closure if tension-free
- Local flaps or skin grafts for large defects
- Vascular repair if sacrifice was necessary
- Drain placement for dead space management
Limb salvage achieved in greater than 95% of extremity sarcomas.
Intraoperative Considerations
If frozen section shows positive margin:
- Re-excise immediately if feasible
- Document location for postoperative radiation boost
- Accept closer margin on vessels/nerves (radiation can cover)
- Do NOT compromise limb function for marginal gains
When approaching nerve/vessel:
- Preserve if 1mm or more margin achievable
- Sacrifice if tumor encases structure
- Vascular reconstruction possible
- Nerve sacrifice: document for rehab planning
Complications
Perioperative Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Local recurrence | 10% (R0) to 50% (R1) | Positive margins, high grade, retroperitoneal | Re-excision ± radiation, MDT review |
| Distant metastases | 10-30% (high-grade) | Dedifferentiated, pleomorphic, round cell | Systemic chemotherapy, palliative care |
| Wound complications | 10-20% | Preoperative radiation, large resection | VAC therapy, debridement, flap coverage |
| Nerve injury | 5-10% | Proximity to major nerves, sacrifice | Physiotherapy, tendon transfers, orthotics |
| DVT/PE | 5-10% | Lower extremity surgery, prolonged immobility | Prophylaxis, early mobilization, anticoagulation |
Late Complications
Risk factors:
- Groin/axillary dissection
- Postoperative radiotherapy
- Extensive resection
Management: Compression, lymphatic massage, elevation
Effects:
- Skin changes (telangiectasia, thinning)
- Muscle/fascia fibrosis
- Joint stiffness
- Secondary malignancy (rare, 1%)
Prevention: Preoperative RT has lower fibrosis than postoperative
Postoperative Care
Standard Recovery Protocol
Postoperative Management
Inpatient care:
- Wound monitoring (flap viability, drainage)
- DVT prophylaxis (mechanical + pharmacological)
- Pain management (multimodal analgesia)
- Early mobilization with physiotherapy
Ward care:
- Drain management (remove when less than 30ml/24h)
- Wound assessment (infection, dehiscence)
- Progressive mobilization
- Discharge planning when mobile and wound stable
Clinic review:
- Wound check, suture removal
- Final histology and margin review
- MDT discussion of adjuvant therapy
- Radiation planning if indicated
If indicated:
- Radiotherapy (50-66 Gy over 5-7 weeks)
- Chemotherapy for high-grade (doxorubicin-based)
- Continue physiotherapy during adjuvant treatment
Treatment completion marks start of surveillance phase.
Functional Rehabilitation
| Scenario | Rehabilitation Focus | Expected Outcome |
|---|---|---|
| Standard excision (muscle sparing) | ROM, strengthening, return to activity | Full function 6-12 weeks |
| Muscle resection (single muscle) | Compensatory strengthening, gait training | Good function with adaptation |
| Nerve sacrifice (femoral, sciatic) | Orthotics, tendon transfers, gait retraining | Functional ambulation achievable |
| Post-radiation complications | Gentle ROM, lymphedema management | Variable, may require intensive therapy |
Guidelines, Registries & Global Practice
Global Epidemiology
Liposarcoma is the most common soft tissue sarcoma in adults, representing roughly 20-25% of all soft tissue sarcomas. Soft tissue sarcomas overall have an incidence of approximately 4-5 per 100,000 per year across most high-income populations, so liposarcoma incidence is on the order of 1-2.5 per 100,000 per year. Peak incidence is in the sixth and seventh decades, with a slight male predominance. Well-differentiated and dedifferentiated subtypes are concentrated in the retroperitoneum and deep extremity, while myxoid liposarcoma characteristically affects a younger cohort (median in the 40s) and arises in the thigh.
Side-by-Side Guideline Comparison
| Body / Region | Biopsy | Local Treatment | Radiotherapy Stance |
|---|---|---|---|
| ESMO-EURACAN (Europe) | Image-guided core needle through excisable tract at reference centre | Wide excision with negative margins; MDT-led | Recommended for high-grade, deep, large extremity tumours; not standard for retroperitoneal disease |
| NCCN (US) | Core needle biopsy preferred; coordinate with sarcoma team | Limb-sparing wide resection; amputation rarely needed | Pre- or postoperative radiotherapy for higher-risk extremity sarcoma; selective in retroperitoneum |
| NICE / BSG-BOA (UK) | Refer suspicious lumps (deep, over 5cm, or growing) to sarcoma service before intervention | Planned wide excision at a specialist sarcoma centre | Neoadjuvant or adjuvant radiotherapy for high-risk limb sarcoma per MDT |
| WHO (pathology) | Molecular confirmation: MDM2/CDK4 for ALT-WDLS-DDLS, FUS-DDIT3 for myxoid | Classification drives prognosis and therapy | Subtype (esp. myxoid) informs radiosensitivity expectations |
All major bodies agree on biopsy-before-resection, wide negative margins, and management within a sarcoma MDT. The key area of genuine divergence is retroperitoneal radiotherapy: after the STRASS trial, routine preoperative radiotherapy is no longer recommended for primary retroperitoneal sarcoma, whereas radiotherapy retains a clear role in high-risk extremity disease.
Registry and Reference-Centre Evidence
- Large prospective single-institution databases (e.g. Memorial Sloan Kettering, 801-patient series) underpin the subtype-specific nomograms used worldwide
- National cancer registries (SEER in the US, RARECARE in Europe) confirm liposarcoma as the leading adult soft tissue sarcoma and the rising relative incidence with age
- Outcomes are consistently better when care is delivered at high-volume reference centres
- Well-resourced: routine MRI, MDM2 FISH, intensity-modulated radiotherapy, trabectedin access, and formal sarcoma MDTs
- Limited-resource: reliance on histology and immunohistochemistry where FISH is unavailable; wider use of upfront surgery; constrained access to radiotherapy and modern systemic agents
- Universal principle: any deep or large (over 5cm) lipomatous mass warrants imaging and biopsy before excision, regardless of setting
Process safeguards that protect patients in any health system:
- Pre-biopsy imaging and staging completed before intervention
- Biopsy performed by or in consultation with a sarcoma team, through an excisable tract
- MDT discussion documented before definitive surgery
- Informed consent covering recurrence risk, margin status, and adjuvant therapy
- A defined surveillance plan at discharge
Recurring pitfalls (the "whoops" lesion):
- Unplanned excision of a presumed lipoma without imaging/biopsy (missed liposarcoma)
- Inadequate margins requiring re-excision
- Failure to refer to a sarcoma MDT
- Inadequate surveillance leading to late detection of recurrence
Evidence Base and Key Studies
Subtype-Specific Prognostic Nomogram for Primary Liposarcoma (801 patients)
- 801 patients with primary liposarcoma from a single prospective database (1982-2005)
- Subtype distribution: well-differentiated 46%, dedifferentiated 18%, myxoid 18%, round cell 10%, pleomorphic 8%
- Overall 5-year and 12-year disease-specific survival 83% and 72%
- Independent predictors of survival: age, histologic variant, primary site, tumour burden, and gross margin status
- A liposarcoma-specific nomogram outperformed the generic sarcoma nomogram (concordance 0.83 vs 0.78)
MDM2/CDK4 Amplification Distinguishes Atypical Lipomatous Tumour from Lipoma
- All atypical lipomatous tumours showed ring chromosomes and 12q13-15 amplification
- MDM2 protein overexpressed in atypical lipomatous tumours but NOT in any ordinary lipoma
- CDK4 overexpression present in 100% of atypical lipomatous tumours (only weak focal staining in 11% of lipomas)
- MDM2 and CDK4 immunohistochemistry increases diagnostic accuracy in distinguishing ALT from lipoma
Trabectedin (Ecteinascidin-743) in Advanced Pretreated Myxoid Liposarcoma
- 51 patients with advanced pretreated myxoid liposarcoma treated in a compassionate-use programme
- Overall RECIST response 51% (2 complete, 24 partial responses)
- Median progression-free survival 14.0 months; 6-month PFS 88%
- Characteristic radiological pattern: tissue-density and enhancement changes preceded tumour shrinkage
- Mechanism linked to the FUS-DDIT3 (DDIT3-FUS) translocation that defines this sarcoma
Radiosensitivity Translates into Excellent Local Control in Extremity Myxoid Liposarcoma
- 88 extremity myxoid liposarcomas compared with 603 other soft tissue sarcomas
- 5-year local recurrence-free survival 97.7% for myxoid vs 89.6% for other subtypes (p=0.008)
- Superior systemic control: 5-year overall survival 93.9% vs 76.4%
- No myxoid liposarcoma patient required amputation as primary management
- Findings support a distinctive radiosensitivity of the myxoid subtype
Preoperative versus Postoperative Radiotherapy in Limb Soft Tissue Sarcoma (landmark RCT)
- 190 patients randomised to preoperative (50 Gy) versus postoperative (66 Gy) radiotherapy
- Acute wound complications higher with preoperative radiotherapy (35% vs 17%, p=0.01)
- Overall survival slightly favoured the preoperative group (p=0.048)
- Trade-off: preoperative radiotherapy gives more early wound complications but a smaller field and lower long-term fibrosis
Dose-Reduced Preoperative Radiotherapy in Myxoid Liposarcoma (DOREMY trial)
- Prospective phase 2 trial; 79 patients with translocation-confirmed myxoid liposarcoma
- Reduced preoperative dose of 36 Gy (vs standard 50 Gy) in 2-Gy fractions
- Extensive pathological treatment response in 91% of resection specimens
- Local control rate 100%; wound complications requiring intervention only 17%
Preoperative Radiotherapy in Retroperitoneal Sarcoma (EORTC STRASS, phase 3 RCT)
- 266 patients with primary retroperitoneal sarcoma randomised to surgery alone versus preoperative radiotherapy (50.4 Gy) plus surgery
- No difference in abdominal recurrence-free survival (HR 1.01, p=0.95)
- Liposarcoma was the predominant histology in the trial cohort
- Higher serious adverse events with radiotherapy (24% vs 10%)
ESMO-EURACAN-GENTURIS Clinical Practice Guidelines: Soft Tissue and Visceral Sarcomas
- Core needle biopsy through a planned, excisable tract before any definitive surgery
- Wide excision with negative margins is the standard local treatment for extremity/trunk disease
- Radiotherapy recommended for high-grade, deep, large extremity sarcomas to improve local control
- Management of all suspected sarcomas at a reference centre with a sarcoma multidisciplinary team
Controversies and Areas of Uncertainty
Liposarcoma management contains several genuinely unsettled questions that examiners use to probe depth of understanding. Acknowledging uncertainty (rather than overstating dogma) is a marker of consultant-level reasoning.
The STRASS trial showed no abdominal recurrence-free survival benefit for routine preoperative radiotherapy. Debate continues over whether specific subgroups (well-differentiated or low-grade liposarcoma) may still benefit, and the STRASS-2 trial is examining the question further. Current consensus: not routine.
The 'compartmental' or extended frontline resection (en-bloc removal of adjacent uninvolved organs) reduces local recurrence in some series but increases morbidity, and high-quality randomised data are lacking. Practice varies between expert centres.
There is no consistent survival benefit from adjuvant chemotherapy across soft tissue sarcoma trials. Its role in high-grade liposarcoma (dedifferentiated, pleomorphic, round-cell myxoid) remains individualised and MDT-driven rather than standard.
The same MDM2-amplified entity is called atypical lipomatous tumour in the limb and well-differentiated liposarcoma in the retroperitoneum. Some argue uniform malignant nomenclature improves follow-up compliance; others favour 'ALT' to avoid over-treatment of indolent limb lesions.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with a 10cm deep mass in his thigh that has grown over 6 months. MRI shows a predominantly fatty mass with thick septations and some solid enhancing areas. What is your differential diagnosis and initial management?”
“You excised a 12cm deep thigh mass thinking it was a lipoma. Histology returns as dedifferentiated liposarcoma with positive deep margin (tumor 1mm from fascia). The patient is 10 days post-op. How do you proceed?”
“Biopsy of a 15cm calf mass confirms myxoid liposarcoma, FUS-DDIT3 positive. CT staging shows no metastases. The tumor is close to the tibial nerve. The MDT asks for your surgical plan. What do you propose?”
MCQ Practice Points
Q: What molecular marker distinguishes well-differentiated liposarcoma from benign lipoma? A: MDM2 amplification - MDM2 and CDK4 amplification detected by FISH is diagnostic for well-differentiated liposarcoma (atypical lipomatous tumor) and absent in benign lipoma. This testing is essential for any deep or large fatty tumor to guide surgical planning.
Q: Which liposarcoma subtype is most radiosensitive and why? A: Myxoid liposarcoma - This subtype shows unique radiosensitivity attributed to the FUS-DDIT3 fusion protein affecting DNA repair. Radiotherapy achieves excellent local control and may produce near-complete pathological response. This is the only soft tissue sarcoma subtype where radiation is more effective than others.
Q: What is the 5-year survival for extremity well-differentiated liposarcoma after complete excision? A: 80-90% - Extremity well-differentiated liposarcoma (atypical lipomatous tumor) has excellent prognosis with wide excision achieving negative margins. Metastatic potential is less than 2%. In contrast, retroperitoneal well-differentiated liposarcoma has worse prognosis (50% 5-year survival) due to difficulty achieving negative margins and higher recurrence rate.
Q: What is the most important prognostic factor for local recurrence in liposarcoma? A: Surgical margin status - Negative margins (R0 resection) are associated with 10% local recurrence. Positive margins increase recurrence to 30-50%. Re-excision to achieve negative margins significantly improves local control and is mandatory if initial margins positive.
Q: What chromosomal translocation is pathognomonic for myxoid liposarcoma? A: t(12;16) producing FUS-DDIT3 fusion - This translocation is present in 95% of myxoid liposarcomas. Alternative fusion EWSR1-DDIT3 from t(12;22) occurs in 5%. Detection by RT-PCR or FISH confirms diagnosis and has therapeutic implications (radiosensitivity, trabectedin efficacy).
Key Epidemiology
- Most common soft tissue sarcoma in adults (24% of all sarcomas)
- Peak age 50-65 years, slight male predominance
- 75% extremity/trunk, 25% retroperitoneum
- Incidence 2.5 per million per year
WHO Classification (Prognosis)
- Well-differentiated (40-45%) = ALT = MDM2+ = 80-90% 5-year (extremity)
- Myxoid (30-35%) = FUS-DDIT3 = radiosensitive = 70% 5-year
- Dedifferentiated (10-15%) = MDM2+ with high-grade = 30-40% 5-year
- Pleomorphic (5-10%) = poorest prognosis = 30% 5-year
Molecular Markers (MF Mnemonic)
- MDM2 for Well-differentiated/dedifferentiated (FISH gold standard)
- FUS-DDIT3 for Myxoid (t12;16 translocation)
- MDM2 negative excludes well-differentiated/dedifferentiated
- Round cell variant (greater than 5% round cells) worse prognosis
Staging Workup (MBCPM Mnemonic)
- MRI of primary = local staging and surgical planning
- Biopsy (core needle 14-16G) = never excisional biopsy
- CT chest = rule out lung metastases
- PET-CT if myxoid = FDG-avid subtype
- MDT discussion = before definitive treatment
Surgical Principles
- Wide excision with 1-2cm margins (R0 resection goal)
- Excise biopsy tract en bloc with tumor
- Positive margins mandate re-excision (within 2-4 weeks)
- Limb salvage possible in over 95% extremity sarcomas
- Retroperitoneal requires organ resection, accept close margins on vessels
Adjuvant Therapy
- Radiotherapy for high-grade or close/positive margins (reduces recurrence 30% to 10%)
- Myxoid subtype uniquely radiosensitive (preop RT 50 Gy)
- Chemotherapy: Doxorubicin + ifosfamide for high-grade
- Trabectedin highly active in myxoid subtype (50% response)
- Well-differentiated does NOT respond to chemotherapy
Prognosis and Surveillance
- 5-year survival: Well-differentiated extremity 80-90%, myxoid 70%, dediff/pleo 30-40%
- Positive margins increase local recurrence from 10% to 30-50%
- Follow-up: Q3-4mo years 1-2, Q6mo years 3-5, annual after 5 years
- MRI primary site and CT chest (high-grade) per schedule
- Well-differentiated can recur late (10+ years) - indefinite surveillance