Physeal Stress Fracture | Repetitive Rotational Stress | Mandatory Rest | Growth Arrest Rare
- Definition: Stress fracture of the proximal humeral physis (Salter-Harris Type I equiv)
- Mechanism: Repetitive rotational stress during late cocking/acceleration phases
- Imaging: X-ray shows physeal widening, sclerosis, and fragmentation
- Treatment: STRICT REST from throwing is the only effective treatment
- Return to Sport: Gradual program only after symptom-free and X-rays normalize
- Complication: Premature physeal closure with humeral length discrepancy (rare)
- “Classic patient is an 11-16 year old male pitcher
- “Pain is localized to the proximal humerus (lateral shoulder), not the cuff
- “Comparison views are essential to detect subtle widening
- “Must differentiate from rotator cuff tendonitis (uncommon in this age)
- “Pitch count limits are the key to prevention
Shoulder pain in a skeletal immature thrower is Little League Shoulder until proven otherwise. Rotator cuff pathology is extremely rare in this age group. Do not diagnose "strain" without X-rays.
Comparison views of the contralateral shoulder are mandatory. The widening of the physis can be subtle and physiological asymmetry exists, but significant widening suggests pathology.
Complete cessation of throwing is required. Simply "reducing pitch count" or "playing other positions" is insufficient. Continued stress leads to growth arrest.
Evaluate mechanics. Poor trunk rotation, scapular dyskinesis, or core weakness often predisposes to shoulder overload. Rehabilitation must address the entire chain.
- Age
- 11-16 (Physis open)
- Key Feature
- Widened PROXIMAL physis, TTP lateral shoulder
- Management
- Strict throwing rest (3mo)
- Age
- 12-18 (Hypermobile)
- Key Feature
- Positive sulcus sign, generalized laxity
- Management
- Rehabilitation (cuff/scapula)
- Age
- Any age
- Key Feature
- Acute trauma history, visible deformity
- Management
- Immobilization vs Surgery
- Age
- Usually over 18 (Adults)
- Key Feature
- Positive Neer/Hawkins (Rare in kids)
- Management
- PT, rarely surgery in kids
WIDENWIDEN - Radiographic Findings
Hook:WIDEN reminds you of the classic physeal changes seen on X-ray
Overview and Epidemiology
Little League Shoulder (Proximal Humeral Epiphysiolysis) is an overuse injury affecting the proximal humeral growth plate in skeletally immature throwing athletes.
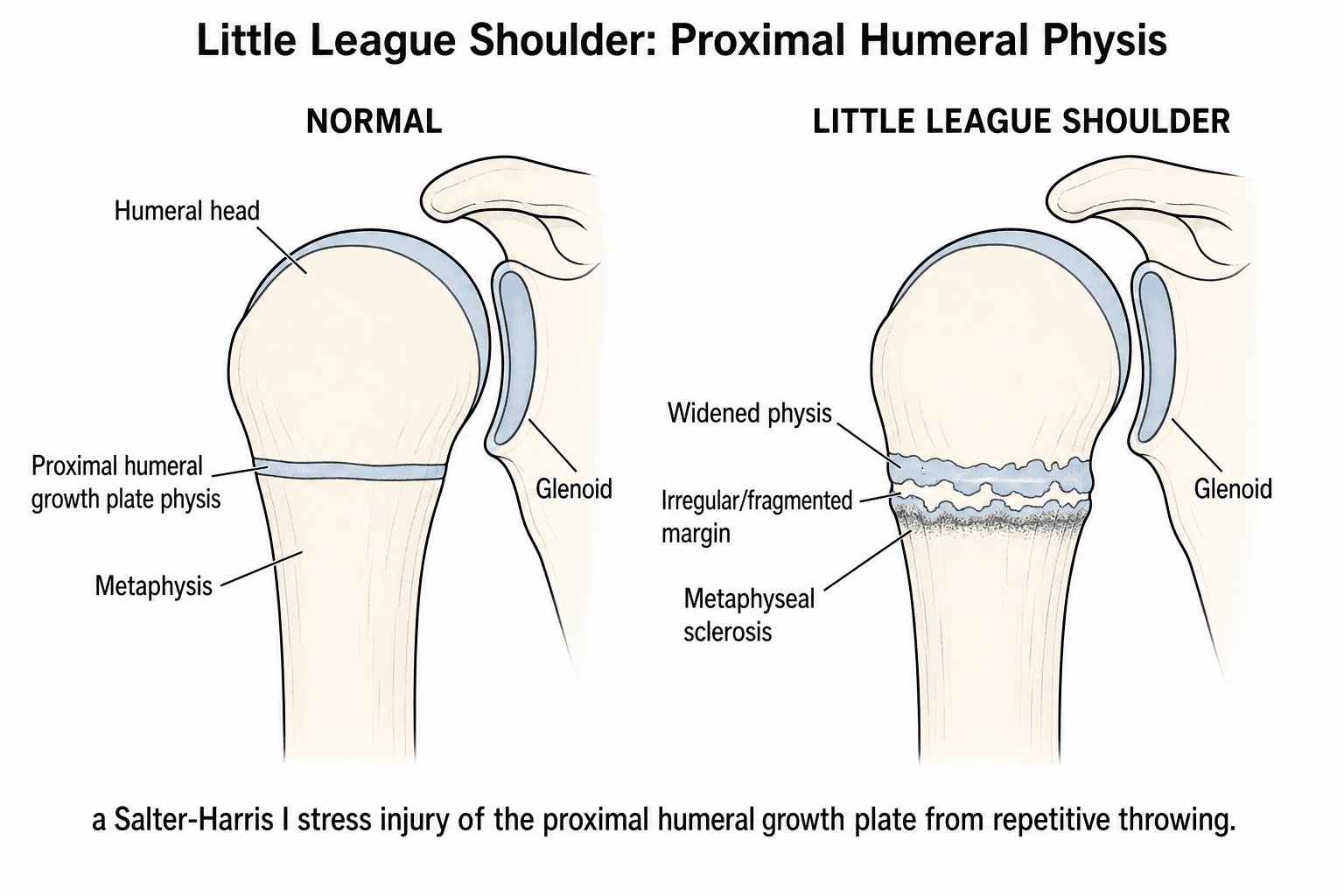
- Essentially a Salter-Harris Type I stress fracture of the proximal humerus physis
- Occurs due to repetitive rotational shear and distraction forces
- The physis (growth plate) is the "weak link" in the kinetic chain of the young athlete
- The proximal humerus contributes 80% of longitudinal growth of the arm
- Rapid growth spurts increase susceptibility as the physis widens and weakens
- Age: mean 13.1 years (range 8-16); skeletally immature with an open proximal humeral physis.
- Gender: strongly male-predominant (93 of 95 patients male) but not exclusive to males.
- Sport: 97% baseball players (86% pitchers, 8% catchers); ~3% tennis players. Reported in other overhead athletes (volleyball, cricket).
- Associated findings: glenohumeral internal rotation deficit (GIRD) in ~30%; concomitant elbow pain in ~13%.
- Trend: diagnosed with increasing frequency, attributed to early sport specialisation and year-round play (Ina et al. 2026; Heyworth et al. 2016).
- Mechanism: repetitive overhead throwing generating high rotational torque at the physis (Sabick et al. 2005).
The adult equivalent of this rotational stress is internal impingement or SLAP lesions. In children, the bone/physis fails before the ligaments or labrum.
Pathophysiology and Mechanisms
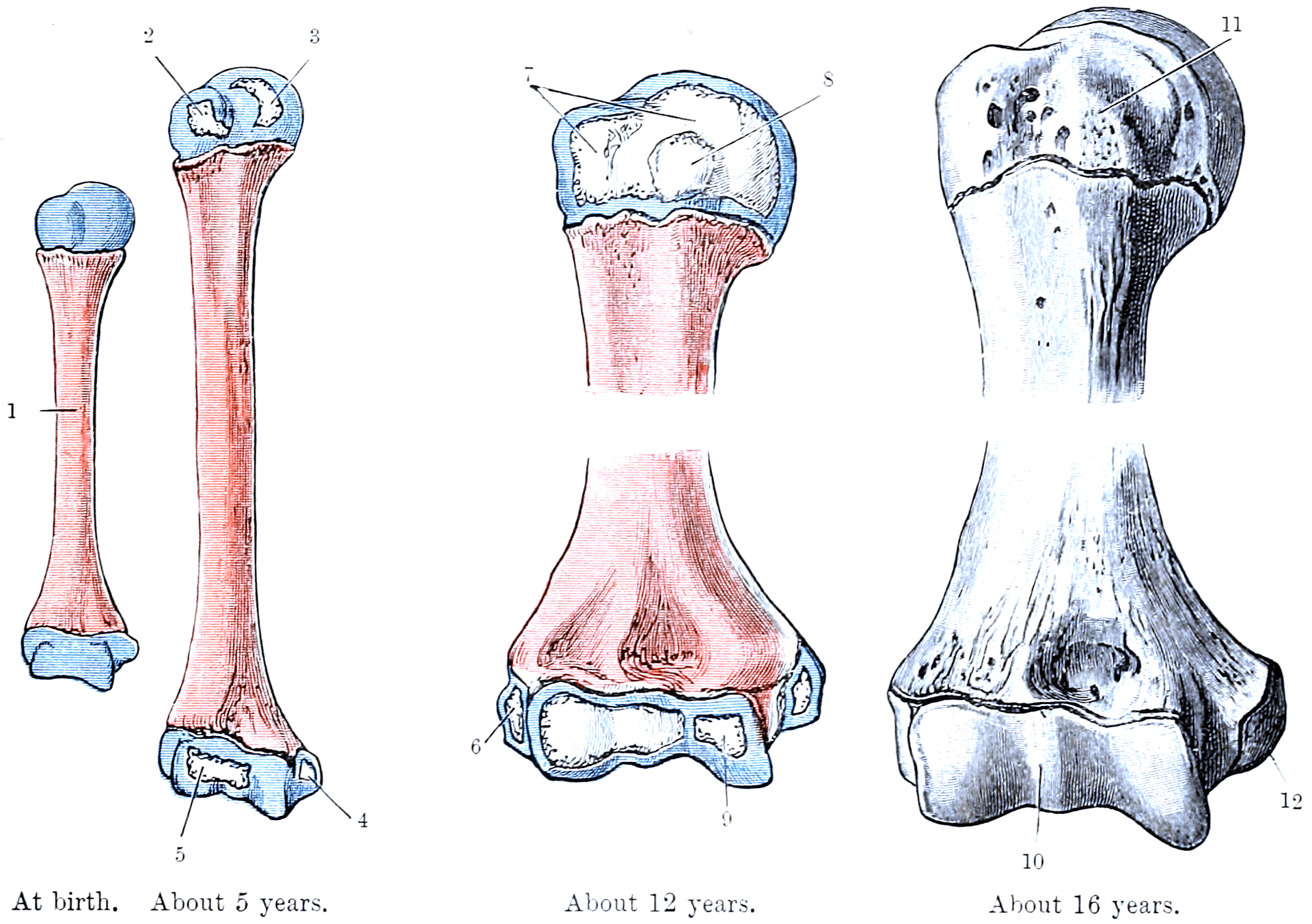
- Ossification centers:
- Head (appears 6 months)
- Greater Tuberosity (appears 3 years)
- Lesser Tuberosity (appears 5 years)
- Coalescence: Centers merge at age 5-7 to form single epiphysis
- Physeal Closure: Typically closes at age 14-17 (females earlier) or 16-19 (males)
- Contributes 80% of humeral length
- Late Cocking Phase: Maximal external rotation places rotational shear stress across the physis.
- Deceleration Phase: Distraction forces pull the epiphysis.
- The physis is weaker against shear and tension than compression.
- Repetitive microtrauma leads to widening of the hypertrophic zone of the physis, failure of calcification, and eventual stress fracture.
- The proximal humeral epiphysis is supplied by the arcuate artery (ascending branch of the Anterior Humeral Circumflex Artery).
- The physis acts as a barrier to blood flow from the metaphysis.
- Although damage to the physis can theoretically disrupt supply, avascular necrosis (AVN) is extremely rare in Little League Shoulder because the fracture is usually Type I (slipped) without significant displacement or vessel disruption.
- Throwers normally develop increased humeral retroversion (bony adaptation).
- The proximal humerus "twists" during growth to allow the hand to reach further back in late cocking.
- This results in increased External Rotation (ER) and decreased Internal Rotation (IR).
- Total Arch of Motion (ER + IR) should remain equal to the contralateral side.
- This allows greater external rotation range without checking the capsule.
- In Little League Shoulder, "Opening Up Early" (anterior trunk rotation) causes the arm to lag behind, increasing the torque on the physis beyond its limits.
- Biomechanical analysis often reveals that the pitcher relies too much on the arm and not enough on the legs/trunk ("Arm Thrower").
Classification Systems
Classic Clinical Grading (based on symptoms):
- Symptoms
- Pain only after throwing
- Pathological Correlate
- Physeal irritation
- Management
- Rest 2-4 weeks
- Symptoms
- Pain during throwing
- Pathological Correlate
- Microfractures
- Management
- Rest 6-8 weeks
- Symptoms
- Pain with ADLs
- Pathological Correlate
- Significant widening
- Management
- Rest 3+ months
- Symptoms
- Pain at rest / night
- Pathological Correlate
- Impending/Complete fracture
- Management
- Immobilization
Clinical Relevance:
- Most patients present at Grade II or III.
- Grade IV represents an acute Salter-Harris fracture completion.
Diagnosis is primarily clinical, supported by radiographic findings.
Clinical Presentation and Assessment
History:
- Patient: Young male pitcher (11-16 years)
- Pain: Progressive onset shoulder pain
- Location: Proximal humerus / Lateral shoulder (Deep ache)
- Timing: Initially only with throwing, progresses to ADLs
- Volume: History of high pitch counts, recent increase in play, or "showcase" events
- Mechanics: Often reports fatigue or "dead arm" sensation
Patients often point to the lateral deltoid area (insertion of deltoid or proximal humerus). They rarely point to the AC joint or subacromial space. Pain is deep inside the bone.
Physical Examination:
- Inspection: Usually normal. Mild atrophy in chronic cases.
- Palpation: Maximal tenderness over the proximal humeral physis. This is the hallmark. (Lateral aspect, just below acromion).
- ROM:
- GIRD (Glenohumeral Internal Rotation Deficit) common
- Increased External Rotation (adaptive)
- Strength: Often normal, but pain with resisted abduction/rotation.
- Special Tests:
- Neer/Hawkins: Negative (or false positive due to extensive irritability)
- O'Brien's: Usually negative
- Scapular Dyskinesis: Check for winging/dysrhythmia (predisposing factor)
- Key Differentiating Feature
- Lateral shoulder pain, Widened physis
- Investigation
- X-ray (Comparison)
- Key Differentiating Feature
- Global laxity, Sulcus sign, Atraumatic
- Investigation
- Clinical Exam
- Key Differentiating Feature
- Rare in kids (less than 1%), Overdiagnosed
- Investigation
- Rule out LLS first
- Key Differentiating Feature
- Incidental or pathological fracture
- Investigation
- X-ray (Lytic lesion)
- Key Differentiating Feature
- Night pain, Systemic symptoms, Mass
- Investigation
- MRI / Biopsy
Associated Throwing Injuries to Screen For
Little League shoulder is one node in a wider spectrum of open-physis overuse injuries in the skeletally immature thrower (Ina et al. 2026). Roughly 13% of children with Little League shoulder have concurrent elbow pain (Heyworth et al. 2016), so the whole arm must be examined end to end — never clear the shoulder and ignore the elbow.
- Site / pathology
- Proximal humeral physis (Salter-Harris I stress injury)
- Key clue
- Lateral/proximal humeral tenderness, physeal widening
- Site / pathology
- Traction apophysitis, sometimes acute avulsion, of the medial epicondyle from repetitive valgus
- Key clue
- Medial elbow pain and tenderness; can avulse acutely with a 'pop'
- Site / pathology
- Lateral-compartment compression/shear of the capitellum
- Key clue
- Lateral elbow pain, effusion, loss of extension; can shed loose bodies
- Site / pathology
- Medial elbow ligament under valgus load (more in the older, closing-physis adolescent)
- Key clue
- Medial pain on valgus stress, loss of velocity/control
- Site / pathology
- Soft-tissue/labral analogue of LLS in the adult or older thrower
- Key clue
- Posterior shoulder pain in abduction–external rotation
GIRD, scapular dyskinesis and a poor kinetic chain predispose to all of these, so the rehabilitation that protects the shoulder also protects the elbow. Lateral elbow pain, a mechanical block or an effusion should trigger dedicated elbow radiographs to exclude capitellar OCD, which — unlike Little League shoulder — can require surgery and can end a throwing career if missed.
Investigations
Plain Radiographs (Mandatory):
- Views: AP (Internal/External Rotation), Axillary Lateral.
- Must order COMPARISON VIEWS of the contralateral shoulder.
Key radiographic signs ("WIDEN"):
- Widening of the proximal humeral physis
- Sclerosis of the metaphyseal margin
- Fragmentation or cystic changes lateral metaphysis
- Demineralization
- Periosteal reaction (rare, implies healing fracture)
- Usually not necessary if X-rays are diagnostic.
- Indicated if:
- X-rays normal but high clinical suspicion (early stress reaction)
- Unusual presentation (rule out tumor/infection)
- Assessing healing/return to sport (sometimes)
- Findings:
- Physeal edema (high T2 signal)
- Metaphyseal edema usually extending into shaft
- Periosteal edema
- Rarely indicated. Avoid radiation in children.
Management Algorithm

The Cornerstone: COMPLETE REST.
Phase 1: Rest (0-3 Months)
- Goal: Healing of physis.
- Restriction: NO THROWING. Absolute ban on pitching, fielding, or even recreational throwing.
- sling usually not needed unless Grade IV pain.
- Activities: Cardio, Core, Legs permitted immediately.
Phase 2: Rehabilitation (Months 1-3)
- Initiated once pain-free at rest.
- Scapularstabilizers: Serratus anterior, Trapezius.
- Rotator Cuff: High repetition, low weight.
- Core mechanics: Kinetic chain integration (Hip-Shoulder separation).
- GIRD correction: Sleeper stretches (gentle). Focus on posterior capsule flexibility without stressing the anterior structures.
- Lower Extremity: Lunges, single-leg stability. A stable base reduces the requirement for arm velocity generation.
Progression Checklist:
- No pain with Activities of Daily Living (ADLs)
- Full Range of Motion (comparable to contralateral side)
- Symmetrical Scapular Kinesis (No winging)
- Core strength baseline met (e.g., plank hold greater than 60s)
Phase 3: Return to Throwing (Month 3-6)
- Criteria:
- Complete resolution of pain
- Full ROM
- Normal strength
- X-rays show healing (optional but recommended)
- Interval Throwing Program: Gradual progression (e.g., 45ft to 60ft to 90ft).
- Mechanics coaching is essential to prevent recurrence.
- Focus on leg drive and trunk rotation to spare the shoulder.
Returning to throwing before physeal healing leads to rapid recurrence and significantly increases risk of growth arrest. The minimum timeline is usually 3 months.
RESTREST - Management Principles
Hook:REST emphasizes that active treatment (PT) supplements the primary treatment (Time)
Surgical Technique
- The periosteum is thick and intact, preventing displacement.
- Remodeling potential is massive in the proximal humerus (80% of growth).
- Even significant angulation remodeling corrects over time.
- Acute Displaced Fracture: Salter-Harris I/II with greater than 50% displacement or angulation greater than 40 degrees (older child).
- Failed Reduction: Interposition of biceps tendon (rare).
- Open Fracture.
- Multi-trauma.
Operative intervention is a salvage procedure and carries higher risks.
Complications
- Mechanism
- Returning too early
- Outcome
- Prolonged rest needed
- Mechanism
- Chronic continued stress
- Outcome
- Humeral length discrepancy
- Mechanism
- Adaptive bone remodeling
- Outcome
- Usually functional/asymptomatic
- Mechanism
- Posterior capsule tightness
- Outcome
- Increased risk of recurrence
Growth Arrest:
- The most feared complication.
- Continued throwing through pain leads to bar formation.
- Result: Shortened humerus or varus deformity.
- Usually humerus shortening is well tolerated functionally but cosmetically apparent.
Postoperative Care and Rehabilitation
(Refer to the Management section, Nonoperative Protocol)
- 0-4 Weeks: Sling immobilization. Pendulums only.
- 4 Weeks: Pin removal (if K-wires used). Start Active Assist ROM.
- 6-12 Weeks: Strengthening phases.
- Return to Sport: Delayed compared to stress fracture (often 6 months+).
Outcomes and Prognosis
- Excellent with rest and physiotherapy.
- Mean time to symptom resolution 2.6 months; mean time to return to competition 4.2 months.
- Recurrent symptoms in 7% at a mean of 7.6 months after diagnosis.
- Key determinant: patient/parent compliance with throwing rest; GIRD increases recurrence risk and should be corrected before return.
- Premature physeal closure / growth arrest is reported but rare in the published series.
- Adaptation of humeral retroversion (a normal throwing adaptation) persists.
- Nonoperative (Rest + PT)
- High (the large majority return)
- Continuation of Throwing
- Poor (pain persists)
- Nonoperative (Rest + PT)
- mean ~2.6 months (Heyworth 2016)
- Continuation of Throwing
- Chronic worsening
- Nonoperative (Rest + PT)
- mean ~4.2 months (Heyworth 2016)
- Continuation of Throwing
- N/A
- Nonoperative (Rest + PT)
- ~7%; higher with uncorrected GIRD (Heyworth 2016)
- Continuation of Throwing
- High (growth-arrest risk)
- Nonoperative (Rest + PT)
- Usually equal
- Continuation of Throwing
- Shortening possible if growth arrest
Counseling for Growth Arrest:
- Although rare (less than 1%), premature closure can occur if warnings are ignored.
- Resultant shortening is usually 1-2cm if near skeletal maturity.
- If young (e.g., 10-12 years), shortening can be significant (5cm+).
Pitch-Count Guidelines (Pitch Smart)
Because overuse and fatigue — not pitch type — are the dominant modifiable risks (Olsen et al. 2006; Fleisig et al. 2011), age-based pitch counts with mandatory rest days are the cornerstone of both prevention and safe return. The widely used USA Baseball / MLB Pitch Smart limits are examinable; representative daily maxima are:
- Approx. max pitches/day
- About 50
- Rest
- Rest days scale with the day's count (see below)
- Approx. max pitches/day
- About 75
- Rest
- Rest days scale with count
- Approx. max pitches/day
- About 85
- Rest
- Rest days scale with count
- Approx. max pitches/day
- About 95
- Rest
- Rest days scale with count
- Approx. max pitches/day
- About 95
- Rest
- Rest days scale with count
- Approx. max pitches/day
- About 105
- Rest
- Rest days scale with count
The rest-day rule scales with the day's pitch count rather than being fixed. For a 13–14-year-old, for example, roughly: 1–20 pitches need no rest day, 21–35 need one, 36–50 need two, 51–65 need three, and 66 or more need four days off. Additional sport-agnostic principles:
- No pitching on consecutive days in the youngest age groups.
- An annual off-season of roughly four months with no competitive throwing.
- Avoid the dual pitcher–catcher role (it multiplies total throws; Fleisig et al. 2011).
- Do not exceed about 100 innings pitched in a calendar year — exceeding this raised serious-injury risk roughly 3.5-fold (Fleisig et al. 2011).
- Never pitch through arm fatigue or pain, the single strongest behavioural risk factor (Olsen et al. 2006).
"How many pitches can a 13-year-old throw?" — about 95 in a day, with a rest-day count that rises with the day's workload (four days off after 66 or more pitches), no more than about 100 innings in a year, and a genuine off-season. These limits exist precisely to prevent the cumulative physeal overload that causes Little League shoulder.
PITCHPITCH - Risk Factors
Hook:PITCH helps identify modifiable risk factors in history
Guidelines, Registries & Global Practice
Global epidemiology:
- Concentrated in baseball-playing regions (USA, Japan, Latin America, Caribbean, parts of East Asia) where youth pitching volume is high; the largest published cohorts come from US paediatric sports-medicine centres (Heyworth et al. 2016).
- Less common where baseball participation is low, but the same physeal overuse mechanism is seen in other overhead-loading sports: tennis (kick/topspin serve with extreme external rotation), volleyball (spikers/jump servers) and cricket (bowlers, although lumbar spondylolysis is the dominant fast-bowler injury).
- Incidence is reported to be rising, attributed to early single-sport specialisation and year-round play without an off-season (Ina et al. 2026).
Major guidelines and consensus, side by side:
- Core recommendation
- High index of suspicion in skeletally immature throwers; rest-based treatment; adherence to pitch-count and rest guidelines for prevention
- Evidence basis
- Narrative/consensus review
- Core recommendation
- Age-based pitch-count limits and mandatory rest days; avoid pitching through fatigue; limit innings; avoid year-round pitching (~4 months off/year); discourage dual pitcher–catcher roles
- Evidence basis
- Derived from prospective/cohort data (Fleisig 2011; Olsen 2006; Lyman 2002)
- Core recommendation
- Limit single-sport specialisation and total throwing load in skeletally immature athletes to reduce overuse injury
- Evidence basis
- Cohort/observational evidence
- Core recommendation
- Complete cessation of throwing until pain-free, staged return via an interval throwing programme, correct GIRD and kinetic-chain deficits before return
- Evidence basis
- Level III-IV series (Heyworth 2016)
- No dedicated implant registry applies (this is a non-operative, non-implant condition). The relevant high-quality evidence comes from prospective youth-pitcher cohorts: Fleisig et al. 2011 (n=481, 10-year follow-up, 5% serious-injury incidence) and Lyman et al. 2002 (n=476), plus the Heyworth et al. 2016 case series (n=95).
- In high-baseball-volume regions, ultrasound screening of youth pitchers and formal pitch-count enforcement are increasingly used; in low-baseball regions the condition is rare and may be under-recognised, with cricket/tennis/volleyball being the more likely contexts.
- Workload-management frameworks differ by sport (pitch counts in baseball, over/spell limits in cricket, serve volume in tennis) but share the same principle: limit cumulative load on the immature physis and rest at the first sign of arm pain or fatigue.
- Adhere to age-appropriate pitch/over/serve count limits and mandatory rest days.
- Build in an annual off-season (no competitive throwing for roughly 3-4 months).
- Avoid "showcase" events that demand maximal-intensity throwing without a build-up.
- Address fatigue, mechanics and GIRD proactively, since overuse and fatigue are the strongest modifiable risk factors (Olsen et al. 2006).
MCQ Practice Points
Q: Where is the specific site of pathology in Little League Shoulder? A: Proximal Humeral Physis (Growth Plate). Specifically the hypertrophic zone which is weakest against shear stress.
Q: What is the classic X-ray finding? A: Widening of the physis compared to the contralateral side. Also sclerosis and fragmentation.
Q: Which phase of throwing places maximal stress on the proximal humeral physis? A: Late Cocking (Rotational torque) and Deceleration (Distraction).
Q: What is the risk of Avascular Necrosis (AVN) in this condition? A: Extremely Low. Unlike acute femoral neck fractures, the blood supply (arcuate artery) is usually preserved in this stress phenomenon.
Q: What is the adult equivalent of this condition in throwers? A: Internal Impingement (Posterior Superior Glenoid Impingement) and SLAP lesions. In adults, the soft tissue fails; in kids, the physis fails.
Q: What is the earliest finding on MRI before X-rays changes appear? A: Physeal Edema on T2-weighted images. This represents the "pre-slipped" stress reaction phase (Grade I).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old male baseball pitcher presents with 3 weeks of progressive lateral shoulder pain. He has been pitching on two teams this season. Pain is now present during daily activities. Exam shows tenderness lateral shoulder. X-ray shows widening of proximal humeral physis. Diagnosis and Plan?”
“The father of a star 13-year-old pitcher with Little League Shoulder asks if he can just take anti-inflammatories and pitch in the championship next week. 'He has no pain if he takes Advil'. Counseling?”
“A 12-year-old pitcher has 6 weeks of lateral shoulder pain during throwing. Tenderness is over the proximal humerus. Plain radiographs including contralateral comparison views look essentially symmetrical. How do you proceed, and what is your evidence-based reasoning?”
DEMOGRAPHICS
- 11-16 year old Males
- Pitchers most affected
- Rapid growth phase
- Open Proixmal Humeral Physis
- Year-round participation
PATHOLOGY
- Salter-Harris I Stress Fracture
- Proximal Humeral Physis
- Rotational Shear Stress
- Widening of Hypertrophic Zone
- Failure of Calcification
DIAGNOSIS
- Lateral/Deep Shoulder Pain
- TTP Proximal Humerus
- X-Ray: WIDENING of physis
- GIRD often present
- Negative Cuff Signs
MANAGEMENT
- REST (Strict)
- 3 Months Minimum
- Mechanics Rehab
- Return when Pain-free + X-ray healed
- Sequential Return to Throwing
- Pitch Count Adherence
Evidence Base
- Early case description in the orthopaedic literature establishing proximal humeral epiphyseolysis as the lesion underlying 'Little League shoulder'.
- Affected an adolescent male baseball pitcher with widening of the proximal humeral physis on radiographs.
- Symptoms resolved with cessation of throwing.
- 14 elite youth pitchers (mean age 12.1 years) studied during fastball pitching.
- Peak external-rotation torque about the humerus reached 17.7 N.m just before maximal external rotation; a distraction force of ~215 N (~50% body weight) occurred near ball release.
- Shear stress from the high arm-cocking torque is large enough to deform the weak proximal humeral epiphyseal cartilage.
- Rotational (torque) stresses far exceed distraction forces as the dominant mechanism.
- 95 patients (93 male, 2 female; mean age 13.1 years, range 8-16).
- 97% baseball players (86% pitchers); 3% tennis players; GIRD present in 30%.
- Rest recommended in 99%, physical therapy in 79%; mean time to symptom resolution 2.6 months and to return to competition 4.2 months.
- Recurrence in 7% at a mean of 7.6 months; GIRD group had ~3.6x higher odds of recurrence (not statistically significant).
- 95 adolescent pitchers requiring shoulder/elbow surgery vs 45 uninjured controls.
- Injured pitchers threw significantly more months/year, games/year, innings/game, pitches/game and pitches/year.
- Strongest associations with injury were overuse and fatigue; higher pitch velocity and showcase participation also increased risk.
- No significant difference in pitch-type frequency or age at which pitch types were first thrown.
- 476 pitchers aged 9-14 followed for one season; ~50% experienced elbow or shoulder pain.
- Curveball associated with a 52% increased risk of shoulder pain; slider associated with an 86% increased risk of elbow pain.
- Number of pitches per game and per season was significantly associated with elbow and shoulder pain.
- 481 youth pitchers (aged 9-14) followed for 10 years; cumulative incidence of serious injury (surgery or career-ending injury) was 5.0%.
- Pitching more than 100 innings in a single year increased injury risk 3.5-fold (95% CI 1.16-10.44).
- Concomitantly playing catcher trended toward higher risk; the study could not demonstrate that curveballs before age 13 increased risk.
- Contemporary AAOS-published review of throwing injuries in skeletally immature athletes.
- Frames Little League shoulder (proximal humeral epiphysiolysis) alongside internal impingement, Little League elbow, UCL injury and capitellar OCD as a spectrum of open-physis overuse injuries.
- Attributes the rising incidence to early sport specialisation and year-round play without adequate rest.
- Emphasises pitch-count/pitching guidelines and rest as the core of prevention and treatment.