Long Thoracic Nerve Anatomy
Long thoracic nerve → serratus anterior palsy. The whole scapula, especially the inferior angle and medial border, moves medially (toward the spine) and lifts off the chest. Worse on forward elevation / wall push-up. This is the more common neurogenic winging.
Spinal accessory nerve → trapezius palsy. The scapula translates laterally and downward with drooping of the shoulder. Worse on arm abduction. Distinguishing the two clinically is the classic exam task.
Medial = serratus; Lateral = trapeziusScapular winging: medial versus lateral
Hook:Medial winging = serratus (long thoracic), worse on forward push; Lateral winging = trapezius (spinal accessory), worse on abduction. Nail this dichotomy first.
Overview
The long thoracic nerve is the tidiest nerve in the upper-limb syllabus: one nerve, one muscle, one sign. It is purely motor (C5–C7), supplies only serratus anterior, and its failure produces the unmistakable medial scapular winging that examiners love as a spot diagnosis. Its exam value comes from three linked ideas — the anatomy that explains its vulnerability (a long, superficial course down the chest wall), the clinical sign and how to elicit and distinguish it (medial vs lateral winging, wall push-up), and the staged management (most recover, surgery is reserved). Build the topic around "why this nerve is so easily injured and how its single sign is told apart from trapezius winging."
Origin & Course
Root Origin
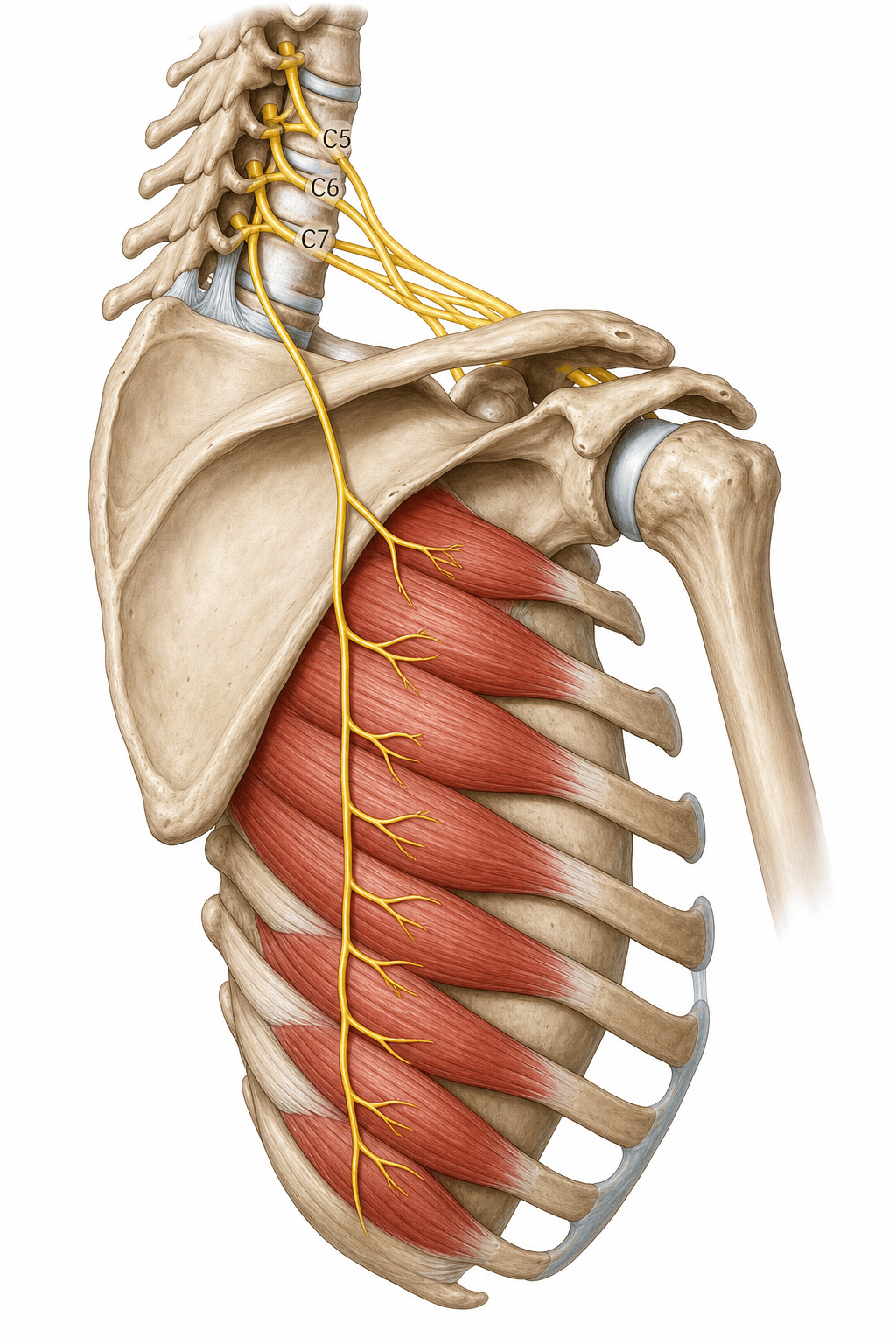
- The long thoracic nerve is a pure motor nerve arising from the anterior (ventral) rami of C5, C6 and C7.
- The C5 and C6 contributions typically pierce the scalenus medius muscle; the C7 contribution usually joins distal to the muscle.
- It arises in the root of the brachial plexus (proximal to the trunks), which is why it can be spared or selectively involved independently of the rest of the plexus.
Mnemonic: "C5, 6, 7 raise your arms to heaven" - serratus anterior upward-rotates the scapula to allow overhead elevation.
Innervation: Serratus Anterior Function
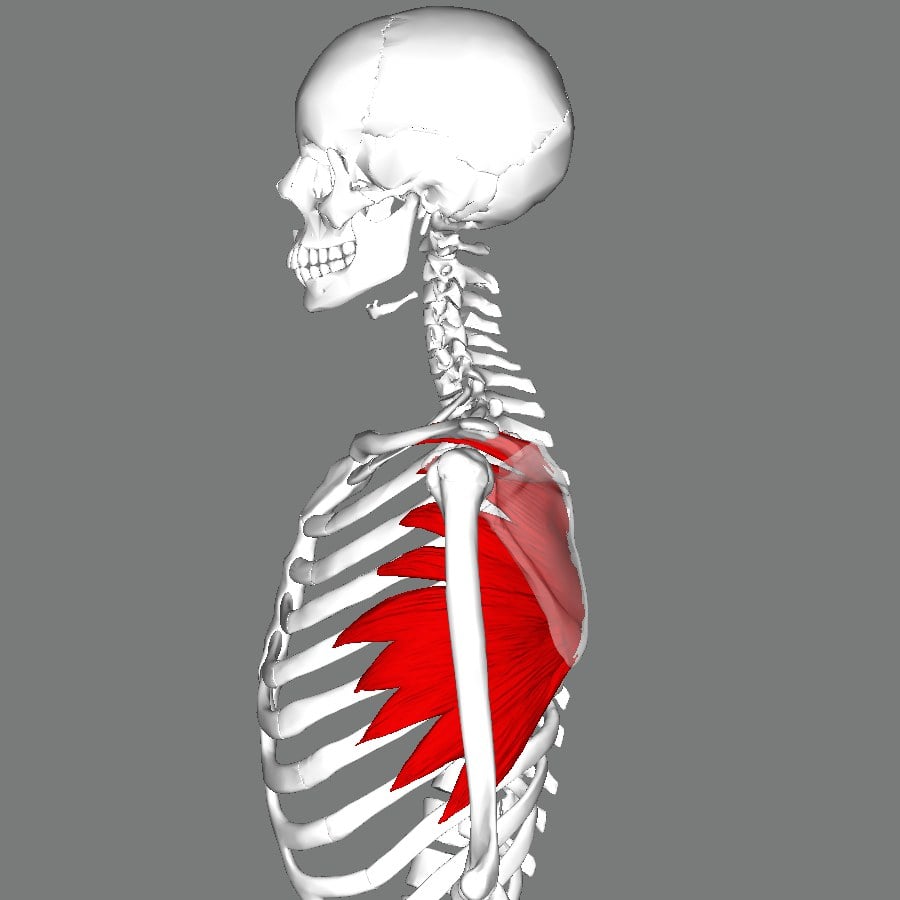
Serratus anterior is the only muscle supplied by the long thoracic nerve. It originates from the upper ribs and inserts along the costal surface of the medial border of the scapula. Its actions are essential for overhead function.
- Protraction of the scapula (draws it forward around the chest wall - the "boxer's punch").
- Upward rotation of the scapula (with the trapezius force couple), which swings the glenoid upward to permit full arm elevation above 90 degrees.
- Scapulothoracic stabilisation - holds the medial border and inferior angle flat against the chest wall.
When serratus anterior fails, the scapula loses its anchor and upward-rotation contribution, producing both medial winging and loss of full overhead elevation.
Clinical: Long Thoracic Nerve Palsy
Presentation
- Medial scapular winging - prominence of the inferomedial scapula, accentuated by forward elevation or pushing against a wall.
- Difficulty elevating the arm overhead and a feeling of shoulder-girdle fatigue/weakness.
- Periscapular pain and aching are common, particularly early.
- May follow trauma, surgery (axillary dissection), heavy/repetitive activity, or a viral/neuralgic amyotrophy prodrome.
The classic spontaneous long thoracic palsy is neuralgic amyotrophy (Parsonage-Turner syndrome / idiopathic brachial plexus neuritis), and examiners expect its pattern, not just the name:
- Course: abrupt, severe neuropathic shoulder/arm pain for days to a few weeks, and as the pain subsides patchy flaccid weakness and wasting appears. It is frequently multifocal in an upper-trunk distribution — the long thoracic, suprascapular, axillary and anterior interosseous nerves are characteristically involved — so look beyond the serratus.
- Triggers: an antecedent viral infection, immunisation, recent surgery, or strenuous exercise in many cases (it can be familial — hereditary neuralgic amyotrophy).
- Imaging: high-resolution MRI/ultrasound may show hourglass-like nerve constrictions or torsion — relevant because these sometimes need surgery if recovery stalls.
- Management: largely supportive with analgesia and physiotherapy; early oral corticosteroids may shorten the painful phase. Recovery is usually good but slow (often 1-3 years) and incomplete in a minority — which is why this group is observed before any nerve surgery.
Before attributing winging to a nerve, exclude the static/structural and muscular causes — EMG alone is not enough, so always get a scapular radiograph (± CT):
- Scapular osteochondroma is the classic trap — a benign exostosis on the ventral (costal) surface of the scapula produces a fixed pseudo-winging with a snapping/grinding scapula and a palpable prominence, typically in a younger patient; it is cured by excision, not physiotherapy or nerve surgery.
- Traumatic muscular avulsion/detachment of serratus, trapezius or rhomboids gives a non-neurogenic winging (the under-recognised cause flagged by Didesch & Tang).
- The three neurogenic types: Type I medial (serratus / long thoracic), Type II lateral (trapezius / spinal accessory), Type III rhomboid (dorsal scapular) — a subtler medial-type winging.
- Voluntary/habitual (pseudo) winging and glenohumeral/scapulothoracic pathology causing protective splinting round out the differential.
So the work-up is examination → scapular imaging to exclude a structural lesion → EMG to confirm and localise a neurogenic palsy.

Management
Management is staged and depends on cause, duration and electrodiagnostic findings:
- Observation and physiotherapy first: most isolated long thoracic nerve palsies - especially neuralgic amyotrophy or traction injuries - recover spontaneously over months. Scapular stabilisation and range-of-motion physiotherapy are the mainstay, with recovery often awaited for up to two years.
- Nerve surgery (neurolysis / nerve transfer): for persistent palsy with no reinnervation, neurolysis of the long thoracic nerve can restore serratus function, with good or excellent results in the majority and best outcomes when performed within about 12 months. Nerve transfers (e.g. a branch of the thoracodorsal nerve to the long thoracic nerve) are an option.
- Tendon/muscle transfer (salvage): for established, irreversible palsy, pectoralis major (sternal head) transfer to the inferior scapula (dynamic stabilisation) is the classic reconstruction; scapulothoracic fusion is a salvage for refractory cases or generalised winging.
WINGLong Thoracic Nerve Essentials
Hook:A failed serratus anterior gives a medial WING.
Guidelines, Registries & Global Practice
Global Practice Picture
The diagnosis and staged management of long thoracic nerve palsy are consistent internationally and rest on clinical examination plus electrodiagnostics rather than registries. The universal principles are: recognise the medial-winging pattern, exclude trapezius (lateral) winging and traumatic muscular detachment, allow spontaneous recovery for isolated/neuralgic cases, and reserve surgery for persistent palsy.
Side-by-Side Synthesis
- Long thoracic (serratus)
- Medial (inferomedial to midline)
- Spinal accessory (trapezius)
- Lateral (scapula translates out/down)
- Long thoracic (serratus)
- Forward elevation / wall push-up
- Spinal accessory (trapezius)
- Arm abduction
- Long thoracic (serratus)
- Traction, axillary surgery, neuralgic amyotrophy
- Spinal accessory (trapezius)
- Posterior triangle surgery (e.g. node biopsy)
- Long thoracic (serratus)
- Physiotherapy; await recovery
- Spinal accessory (trapezius)
- Treat cause; physiotherapy
- Long thoracic (serratus)
- Neurolysis/transfer; pec major transfer; ST fusion
- Spinal accessory (trapezius)
- Eden-Lange transfer
Practice Variation
Electrodiagnostic access varies, but the clinical distinction between medial and lateral winging can be made anywhere with a careful examination. Non-operative care is the universal first step; the choice and availability of nerve versus tendon-transfer surgery for persistent cases varies with local expertise.
Evidence Base
Both references were checked against PubMed. Didesch & Tang is the review that frames the whole topic — the medial (serratus/long thoracic) versus lateral (trapezius/spinal accessory) winging dichotomy, plus the under-recognised traumatic-muscular causes. Roulet's 73-case series is the practical surgical evidence: neurolysis of the long thoracic nerve gave good/excellent results in ~82 percent (winging resolved in 63 percent), best within 12 months and in patients without compensatory muscle pain — supporting nerve surgery before resorting to tendon transfer or fusion. Both are low-level (review/Level IV series), as befits a rare condition; the reproducible anatomy and the clinical winging distinction matter more than any single trial.
Anatomy, Etiology, and Management of Scapular Winging
- Comprehensive review of scapular winging anatomy, aetiology, evaluation and treatment
- Medial winging is caused by serratus anterior dysfunction from long thoracic nerve injury; lateral winging by trapezius dysfunction from spinal accessory nerve injury
- Traumatic detachment of serratus anterior, trapezius and rhomboids is an under-recognised cause of winging
- Diagnosis and management differ between neurogenic and traumatic-muscular causes
Neurolysis of the distal segment of the long thoracic nerve for the treatment of scapular winging due to serratus anterior palsy: a continuous series of 73 cases
- Continuous series of 73 patients undergoing neurolysis of the distal segment of the long thoracic nerve for serratus anterior palsy
- Excellent or good outcomes in 82% of cases; winging resolved in 63% and was minimal in a further 31.5%
- Best results in patients without compensatory muscle pain and treated within 12 months of paralysis
- Neurolysis remained useful beyond 12 months and could avoid palliative (transfer/fusion) surgery