Low Back Pain — Assessment & Non-operative Management
- Cauda equina syndrome is the emergency you must not miss - saddle anaesthesia + bladder/bowel/sexual dysfunction + bilateral leg signs. Urinary retention with overflow is the classic LATE sign; ask and examine in every significant LBP/leg-pain patient and never reassure away new urinary symptoms. Urgent MRI + decompression.
- Do NOT image routine non-specific LBP - degenerative findings are near-universal and correlate poorly with pain; routine imaging worsens outcomes (anxiety, incidentalomas, over-treatment). Image only for red flags, progressive deficit, or persistent radicular pain in a surgical candidate.
- Triage first (non-specific / radicular / red-flag) - this single step, not a structural diagnosis, drives investigation and management.
- AVOID routine opioids - limited benefit, real harms; NSAIDs are first-line. Avoid bed rest (harmful) - keep the patient active.
- Yellow flags (psychosocial) predict CHRONICITY, not serious disease - screen them (e.g. STarT Back) and address early; don't confuse them with red flags.
- Don't offer surgery for non-specific (non-radicular) LBP - reserve surgery/injections for carefully selected refractory radicular/structural cases.
Overview & Epidemiology
Low back pain is one of the leading causes of disability worldwide and a daily clinical problem - and an exam staple because the skill tested is judgement (triage, knowing when NOT to image, avoiding opioid/surgery overuse), not a structural diagnosis.
- Near-universal lifetime experience; a leading global contributor to years lived with disability and to health-care cost.
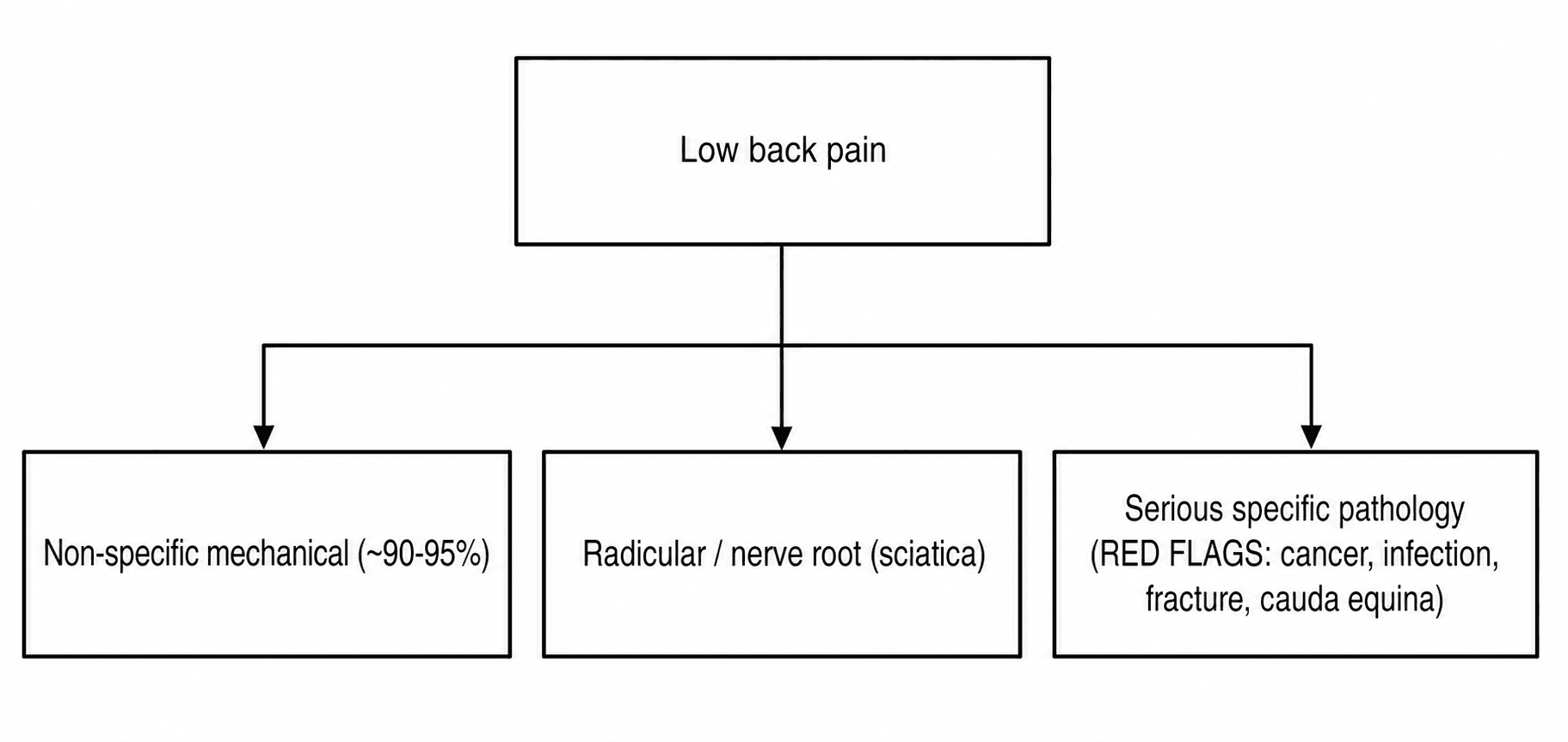
- ~90-95% is 'non-specific' mechanical pain with no identifiable pathoanatomical cause; a minority is radicular; only a small fraction is serious specific pathology.
- Favourable natural history for most acute episodes - many need little formal care - but a substantial minority become chronic and disabling, predicted by yellow flags.
- Why it's examinable: the triage, the red-flag/cauda-equina safety net, the do-not-over-image rule, and the opioid/surgery-overuse problem are all high-yield governance points.
Pathophysiology: why triage, not a structural hunt
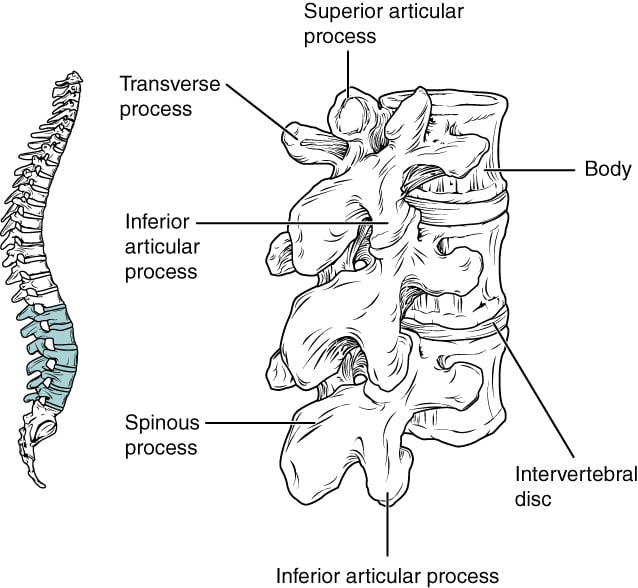
The lumbar spine has many potential pain sources — the vertebral bodies and intervertebral discs, the zygapophyseal (facet) joints, the sacroiliac joints, and the surrounding muscles, ligaments and neurovascular structures. Because of this, and because imaging has low specificity (degenerative changes are near-universal with age and correlate poorly with pain), most low back pain cannot be ascribed to a single pathoanatomical cause and is labelled non-specific. The useful approach is therefore diagnostic triage and a biopsychosocial understanding of why pain becomes disabling — not a structural diagnosis.
Red flags — don't miss serious pathology
- Red-flag features
- Age over 50 or under 20, history of cancer, unexplained weight loss, night/rest pain, pain not relieved by lying down, systemic illness
- Red-flag features
- Fever/rigors, IV drug use, immunosuppression, recent infection/procedure, night sweats
- Red-flag features
- Significant trauma; or minor trauma with osteoporosis, prolonged steroids, or older age
- Red-flag features
- Saddle anaesthesia, bladder dysfunction (retention/overflow incontinence), bowel incontinence, sexual dysfunction, bilateral leg pain/weakness
- Red-flag features
- Age under 45, insidious onset, morning stiffness over 30 minutes, improves with exercise not rest, night pain, alternating buttock pain
Cauda equina syndrome — from a massive central disc herniation or other compression of the lumbosacral nerve roots — presents with saddle anaesthesia, bladder dysfunction (urinary retention with overflow incontinence is the classic late sign), bowel incontinence, bilateral leg symptoms and sexual dysfunction. It demands urgent MRI and emergency surgical decompression, because delay risks permanent bladder/bowel/sexual dysfunction and weakness. Ask about and examine for these features in every patient with significant low back/leg pain — and never reassure away new urinary symptoms.
Beyond "ask about saddle/bladder symptoms," the assessment is objective and staged:
- Examine: perianal (S2–S4) sensation, resting anal tone and voluntary anal squeeze, and the bulbocavernosus / anal-wink reflex; assess the bladder with a post-void residual (bladder ultrasound scan) — a high residual supports a neurogenic, retentive bladder.
- Classify by bladder status (it drives prognosis): CES-incomplete (CES-I) = neurogenic urinary symptoms (altered sensation of voiding/fullness, hesitancy, poor stream) but preserved voluntary control — the better-prognosis group; CES-with-retention (CES-R) = painless urinary retention with overflow incontinence (an established neurogenic bladder) — the worse-prognosis group.
- Act on it: suspected CES needs an urgent (out-of-hours) MRI and, if confirmed, emergency decompression as early as possible — outcome worsens with delay and CES-I does better than CES-R, so the goal is to operate before CES-I progresses to retention. (Detailed operative management lives in the dedicated Cauda Equina topic.)
Whereas red flags flag serious disease, YELLOW FLAGS are psychosocial factors that predict chronic pain and disability: fear-avoidance beliefs, catastrophising, depression/anxiety, job dissatisfaction, low expectation of recovery, and reliance on passive coping. Identifying these early (e.g. with a tool such as STarT Back) lets you target more intensive, psychologically informed care to those at high risk — a core part of modern low-back-pain management.
Clinical Presentation
- Non-specific mechanical (~90-95%): activity-related, paraspinal/axial pain, no identifiable pathoanatomical cause, no neurology
- Radicular (sciatica): dermatomal leg pain ± paraesthesiae/weakness, positive straight-leg-raise/femoral-stretch, often a single nerve root
- Serious specific pathology: flagged by RED FLAGS (below) - cancer, infection, fracture, cauda equina, inflammatory
- Characterise pain (onset, mechanical vs inflammatory vs night/rest), and screen RED and YELLOW flags in every patient
- Neurological exam of the lower limbs (power, reflexes, sensation, SLR/femoral stretch)
- Always ask about saddle sensation and bladder/bowel/sexual function (cauda equina)
- Note psychosocial context (work, mood, beliefs, recovery expectation)
- L4 (typically the L3/4 disc): knee extension (quadriceps), the knee (patellar) reflex, sensation over the medial leg to the medial malleolus; provoked by the femoral stretch test.
- L5 (typically the L4/5 disc): great-toe/ankle dorsiflexion (EHL, tibialis anterior) and hip abduction (gluteus medius — a Trendelenburg gait), no routine reflex, sensation over the lateral leg and dorsum of the foot / first web space; provoked by SLR.
- S1 (typically the L5/S1 disc): ankle plantarflexion/eversion (gastrocnemius — toe-walking), the ankle (Achilles) reflex, sensation over the posterolateral leg, lateral foot and sole; provoked by SLR.
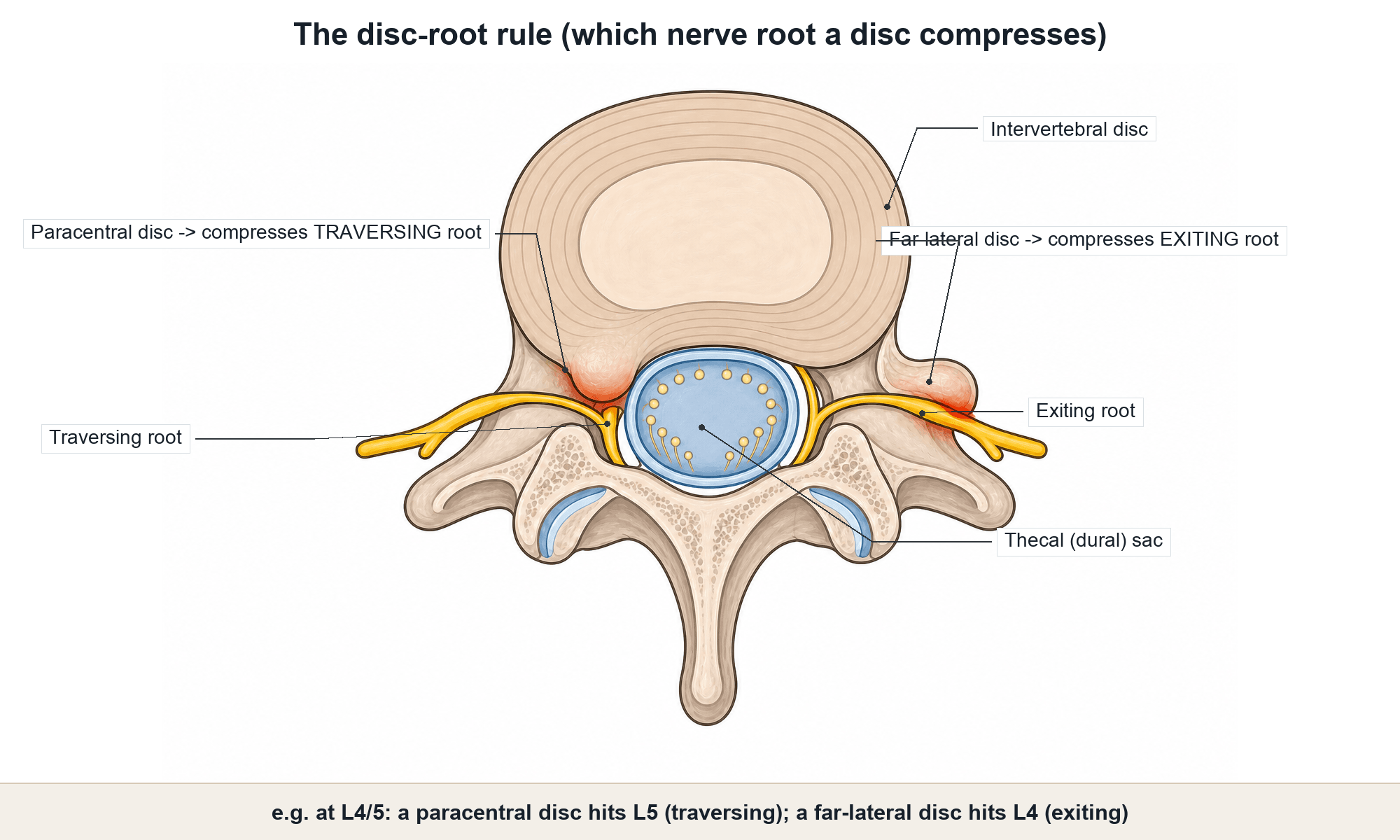
- The disc-root rule: a posterolateral/paracentral disc compresses the TRAVERSING root (so an L4/5 disc hits the L5 root, L5/S1 hits S1); a far-lateral/foraminal disc compresses the EXITING root (L4 at the L4/5 level).
- Provocation tests: the straight-leg-raise (Lasègue) reproduces radicular pain at about 30 to 70° — sensitive but not specific for a lower-lumbosacral root; the crossed SLR (raising the good leg reproduces the affected side's pain) is highly specific for disc herniation; the femoral stretch test examines the upper (L2–L4) roots.
Investigations: mostly NOT imaging
For non-specific low back pain without red flags, routine imaging does NOT improve outcomes and is discouraged: degenerative findings are near-universal, correlate poorly with symptoms, and prompt incidental findings, anxiety and over-treatment. Image when there are RED FLAGS (urgent MRI for suspected cauda equina, infection or malignancy/cord compression), a progressive neurological deficit, or persistent radicular pain in a potential surgical candidate. Blood tests (CRP/ESR, etc.) are directed by the suspected red-flag pathology. The overuse of imaging is a recognised, costly problem.

Management
- 1Triage firstSort into non-specific (~90-95%), radicular, or red-flag serious pathology. This single step drives investigation and management.
- 2Screen flags and (usually) don't imageScreen RED flags (cancer/infection/fracture/cauda equina/inflammatory) and YELLOW flags (psychosocial). Image only for red flags, progressive deficit, or persistent radicular pain in a surgical candidate.
- 3Educate, reassure, keep activeExplain the favourable natural history; advise staying active and avoiding bed rest. NSAIDs first-line (lowest effective dose, shortest time); AVOID routine opioids; short-term muscle relaxant selectively.
- 4Add exercise/psychological care; stratifyExercise/physiotherapy for all; CBT and multidisciplinary rehabilitation for persistent pain or yellow flags. Use risk-stratified/stepped care (e.g. STarT Back); reserve injections/surgery for carefully selected refractory radicular/structural cases.
For non-specific low back pain (and the initial management of most radicular pain), treatment is non-operative and follows the biopsychosocial model:
- Education and reassurance — the favourable natural history and the value of remaining active.
- Stay active / avoid bed rest — the single most consistent advice.
- Analgesia — NSAIDs first-line (lowest effective dose, shortest time); AVOID routine opioids (limited benefit, real harms); short-term muscle relaxants selectively.
- Non-pharmacological — exercise/physiotherapy, and psychological therapies (CBT) / multidisciplinary rehabilitation for persistent pain or yellow flags.
- Risk-stratified or stepped care (e.g. STarT Back) and timely review.
Refractory cases may be offered selected interventions (epidural steroid injection for radicular pain; radiofrequency/facet injections for proven mechanical pain) or, in carefully selected patients with a clear surgical target, surgery — but the overuse of opioids and surgery is a recognised harm.
Education and reassurance about the favourable natural history, advice to stay active and avoid bed rest - the single most consistent recommendation. ACP: for acute/subacute LBP, start with non-pharmacological options (superficial heat, massage, acupuncture, spinal manipulation).
Complications
- Complication
- Cauda equina → permanent bladder/bowel/sexual dysfunction
- Note
- Delayed decompression risks irreversible deficit - the never-miss emergency
- Complication
- Undiagnosed cancer/infection/fracture
- Note
- Red-flag screening exists precisely to catch these early
- Complication
- Transition to chronic, disabling pain
- Note
- Predicted by YELLOW flags (fear-avoidance, catastrophising, low recovery expectation)
- Complication
- Incidental findings → anxiety, over-treatment, cost
- Note
- Routine imaging of non-specific LBP worsens outcomes
- Complication
- Opioid dependence/harm; unnecessary surgery
- Note
- Opioid and surgery overuse are recognised, widespread harms
The two big errors are opposite: missing serious pathology, and over-medicalising non-specific pain. Screen red flags (never miss cauda equina) AND resist routine imaging, opioids and surgery for non-specific LBP - keep the patient active and address yellow flags.
Mnemonics & Memory Aids
- Triage first: non-specific (~90-95%) / radicular / serious red-flag pathology — this drives everything.
- Red flags: cancer, infection, fracture, cauda equina (emergency), inflammatory (axial SpA).
- Cauda equina = saddle anaesthesia + bladder/bowel/sexual dysfunction + bilateral leg signs → urgent MRI + decompression.
- Don't image routine non-specific LBP (low specificity, incidental findings); image for red flags/progressive deficit/surgical radicular pain.
- Yellow flags (psychosocial) predict chronicity — screen with STarT Back.
- Management: reassure + stay active + NSAIDs (not routine opioids) + exercise/CBT; avoid the overuse of imaging/opioids/surgery.
TUNA FISHRed flags
Hook:TUNA FISH = the low-back-pain RED FLAGS (and don't miss cauda equina among the neurological).
ACTIVEManagement
Hook:Keep them ACTIVE: triage, reassure, stay active, NSAIDs not opioids, image only when it matters.
SBBLCauda equina - act now
Hook:SBBL: Saddle, Bladder, Bowel, Legs - the cauda equina red flags that mean MRI and decompress NOW.
Viva practice
Viva practice
Practise clinical reasoning and management decisions out loud
“How do you approach a patient presenting with low back pain, and what red flags do you specifically screen for?”
“A patient has non-specific low back pain with no red flags. How would you manage them non-operatively, and what would you avoid?”
Exam cheat sheet
Triage
- Non-specific mechanical (~90-95%, no pathoanatomical cause)
- Radicular (sciatica/nerve root)
- Serious specific pathology (red flags)
Red flags
- Cancer (age over 50/under 20, prior cancer, weight loss, night pain), infection (fever, IVDU, immunosuppression)
- Fracture (trauma, osteoporosis/steroids), inflammatory (axial SpA features)
- CAUDA EQUINA = emergency: saddle anaesthesia, bladder/bowel/sexual dysfunction, bilateral leg signs → urgent MRI + decompression
Investigation
- Do NOT image routine non-specific LBP (low specificity, incidental findings, harms)
- Image for red flags, progressive deficit, or persistent radicular pain in a surgical candidate
- Screen yellow flags (psychosocial) - predict chronicity
Non-op management
- Education/reassurance + stay active (avoid bed rest)
- NSAIDs first-line; AVOID routine opioids; exercise/physio; CBT for persistent/yellow flags
- Stepped or risk-stratified care (STarT Back); avoid overuse of imaging/opioids/surgery
Evidence Base
Non-specific low back pain
- Non-specific low back pain is a leading global contributor to disability; guidelines endorse triage to identify the rare serious causes needing work-up or referral.
- Because it has no known pathoanatomical cause, treatment focuses on reducing pain and its consequences - education/reassurance, analgesics, non-pharmacological therapies and timely review; the course is often favourable.
- Two strategies - stepped care and simple risk-stratification; the overuse of imaging, opioids and surgery remains a widespread problem.
Low back pain
- LBP spans overlapping nociceptive, neuropathic, nociplastic and non-specific types; many lumbar structures contribute and imaging/diagnostic injections have low specificity.
- The biopsychosocial model frames LBP as a dynamic social-psychological-biological interaction and should guide interdisciplinary treatment.
- Therapy depends on pain classification - self-care and pharmacotherapy with non-pharmacological methods first; refractory cases have non-surgical and surgical options in selected patients.
Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial
- RCT (851 patients) of stratified primary care (low/medium/high prognostic risk with matched pathways) vs current best practice.
- Stratified care gave significantly better disability (Roland-Morris) at 4 and 12 months, with a QALY gain and cost savings.
- Prognostic screening with matched treatment pathways improves outcomes and value in primary-care back pain.
Noninvasive treatments for acute, subacute, and chronic low back pain: an ACP clinical practice guideline
- Acute/subacute LBP usually improves regardless of treatment - start with NON-pharmacological options (superficial heat, massage, acupuncture, spinal manipulation); if drugs are wanted, NSAIDs or muscle relaxants.
- Chronic LBP: first-line non-pharmacological (exercise, multidisciplinary rehabilitation, CBT, mindfulness, tai chi/yoga, etc.); pharmacological first-line is NSAIDs, with tramadol/duloxetine second-line.
- Opioids only if other treatments fail and benefits outweigh risks, after a risk/benefit discussion.
The triage/treat-the-consequences framework and the imaging/opioid/surgery-overuse caution come from Maher et al. 2017 (DOI); the pain-classification and biopsychosocial framing from Knezevic et al. 2021 (DOI); the risk-stratified-care evidence from the STarT Back RCT, Hill et al. 2011 (DOI); and the non-pharmacological-first/opioid-last treatment hierarchy from the ACP guideline, Qaseem et al. 2017 (DOI). The specific red-flag/yellow-flag lists and the cauda-equina emergency are standard, well-established teaching. (See also our Lumbar Disc Herniation, Lumbar Radiculopathy, Lumbar Spinal Stenosis and Cauda Equina material.)