Flexor-Pronator Origin Tendinopathy | 50% Ulnar Nerve Involvement | Conservative First Line
CLINICAL SEVERITY GRADING
Critical Must-Knows
- Flexor-pronator origin pathology - pronator teres and FCR most commonly affected
- 50% have ulnar nerve symptoms - must assess cubital tunnel and exclude UCL injury
- Conservative treatment first line - 90% success rate with PT, NSAIDs, activity modification
- Golfer's elbow test - resisted wrist flexion/pronation reproduces medial elbow pain
- Surgical technique - debride degenerative tissue, preserve ulnar nerve, may need transposition
Clinical Pearls
- "Medial epicondylitis is 5-10 times less common than lateral epicondylitis
- "Pain worse with wrist flexion and forearm pronation (golfer's elbow test)
- "Must exclude UCL injury in overhead athletes (valgus stress test)
- "Ulnar nerve symptoms present in 50% - document preoperatively
Clinical Imaging
Imaging Gallery




Critical Medial Epicondylitis Exam Points
Flexor-Pronator Origin
The pathology is at the flexor-pronator mass origin on the medial epicondyle. Pronator teres and flexor carpi radialis are most commonly affected. This is a degenerative tendinopathy, not inflammatory tendinitis.
Ulnar Nerve Assessment
50% of patients have concurrent ulnar neuritis. Always assess for cubital tunnel syndrome with Tinel's, elbow flexion test, and nerve conduction studies if symptoms present. May need ulnar nerve decompression at surgery.
Differential Diagnosis
Must exclude UCL injury in overhead athletes (valgus stress, milking maneuver). Also consider: cubital tunnel syndrome, medial elbow OA, referred cervical pain, flexor/pronator muscle strain.
Conservative First
90% respond to conservative treatment within 6-12 months. This includes activity modification, PT (eccentric strengthening), NSAIDs, bracing, and corticosteroid injection. Surgery only after 6 months of failed conservative care.
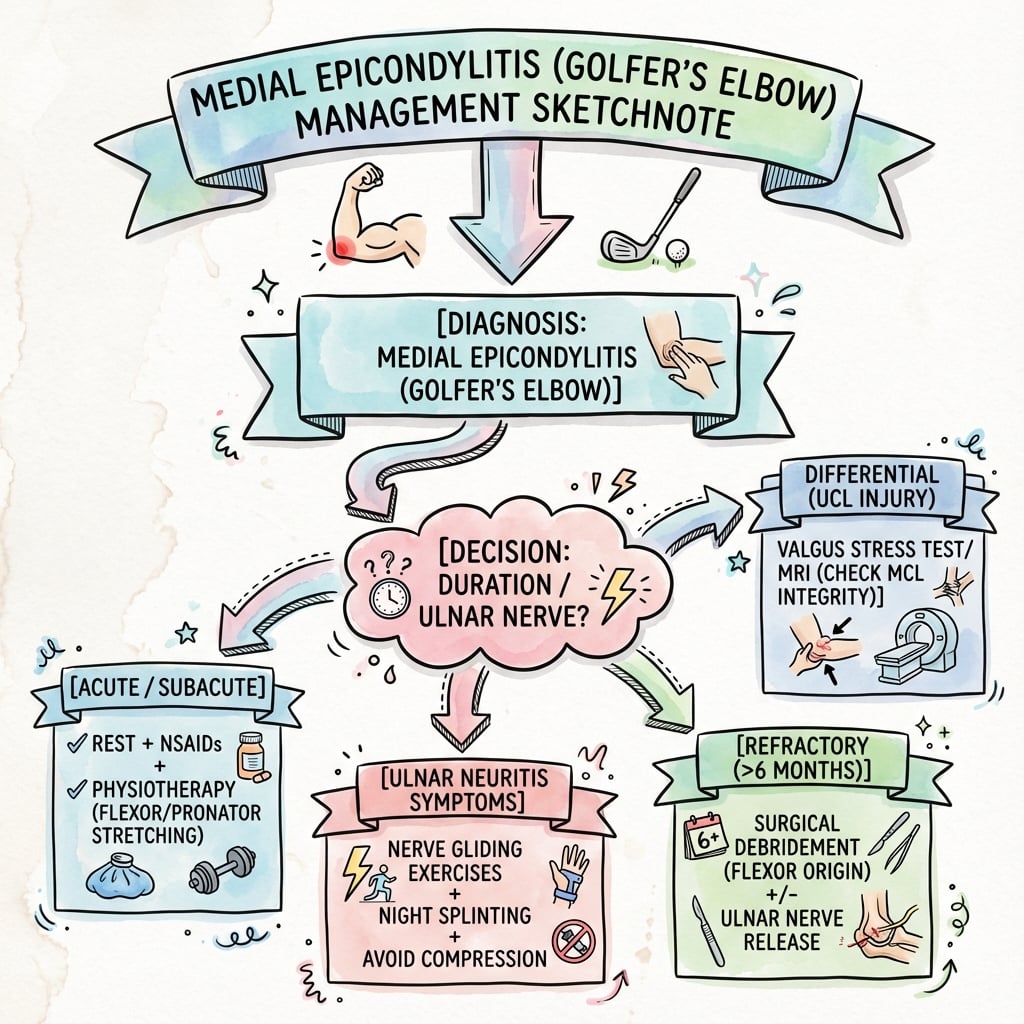
Quick Decision Guide - Management Pathway
| Patient Scenario | Clinical Features | Treatment | Key Pearl |
|---|---|---|---|
| Recreational athlete, 3 months symptoms | Mild pain, normal strength, no nerve symptoms | Conservative: PT, activity modification, NSAIDs | 90% resolve - be patient, avoid early surgery |
| Golfer, 6 months symptoms, persistent | Moderate pain, some weakness, no nerve symptoms | Corticosteroid injection + continued PT | Maximum 2-3 injections due to tendon weakening risk |
| Manual laborer, 12 months, refractory | Severe pain, weakness, failed conservative | Surgical debridement + repair | Screen for ulnar nerve - may need decompression |
| Overhead athlete with ulnar nerve symptoms | Medial pain + paresthesias, positive Tinel's | Assess UCL, consider NCS, surgical if indicated | UCL injury requires different treatment - valgus stress test |
FLEXORFLEXOR - Flexor-Pronator Origin Anatomy
| F | Flexor carpi radialis Most commonly affected tendon |
| L | Location: medial epicondyle Common origin on anterior aspect |
| E | Eight muscles total PT, FCR, PL, FCU + 4 deep flexors |
| X | eXclude UCL injury Valgus stress test in athletes |
| O | Overuse mechanism Repetitive wrist flexion/pronation |
| R | Relation to ulnar nerve 50% have concurrent neuritis |
| F | Flexor carpi radialis Most commonly affected tendon | E | Eight muscles total PT, FCR, PL, FCU + 4 deep flexors | O | Overuse mechanism Repetitive wrist flexion/pronation |
| L | Location: medial epicondyle Common origin on anterior aspect | X | eXclude UCL injury Valgus stress test in athletes | R | Relation to ulnar nerve 50% have concurrent neuritis |
Hook:FLEXOR muscles flex from the medial epicondyle - remember the ulnar nerve is nearby!
GOLFERGOLFER - Clinical Assessment
| G | Golfer's elbow test Resisted wrist flexion reproduces pain |
| O | Origin tenderness Point tenderness at medial epicondyle |
| L | Loss of grip strength Weakness compared to contralateral side |
| F | Forearm pronation painful Resisted pronation reproduces symptoms |
| E | Exclude ulnar nerve Tinel's, elbow flexion test, NCS |
| R | Rule out UCL injury Valgus stress, milking maneuver |
| G | Golfer's elbow test Resisted wrist flexion reproduces pain | L | Loss of grip strength Weakness compared to contralateral side | E | Exclude ulnar nerve Tinel's, elbow flexion test, NCS |
| O | Origin tenderness Point tenderness at medial epicondyle | F | Forearm pronation painful Resisted pronation reproduces symptoms | R | Rule out UCL injury Valgus stress, milking maneuver |
Hook:GOLFER's elbow - think of the golf swing (wrist flexion, pronation) causing overload
CONSERVECONSERVE - Conservative Treatment Protocol
| C | Cease aggravating activities Activity modification, relative rest |
| O | Oral NSAIDs Anti-inflammatory medication |
| N | Nerve assessment Screen for ulnar neuritis |
| S | Strengthening exercises Eccentric PT program |
| E | Equipment modification Brace, counterforce strap |
| R | Rest and ice Acute symptom control |
| V | Very patient approach 6-12 months for resolution |
| E | Evaluate injection Corticosteroid if persistent after 3 months |
| C | Cease aggravating activities Activity modification, relative rest | S | Strengthening exercises Eccentric PT program | V | Very patient approach 6-12 months for resolution |
| O | Oral NSAIDs Anti-inflammatory medication | E | Equipment modification Brace, counterforce strap | E | Evaluate injection Corticosteroid if persistent after 3 months |
| N | Nerve assessment Screen for ulnar neuritis | R | Rest and ice Acute symptom control |
Hook:CONSERVE your tendon - 90% heal without surgery if you're patient!
SURGERYSURGERY - Surgical Indications and Technique
| S | Six months failed conservative Minimum duration before considering surgery |
| U | Ulnar nerve protection Identify, protect, consider transposition |
| R | Remove degenerative tissue Debride abnormal tendon origin |
| G | Grip the bone Decorticate epicondyle for healing |
| E | Excise and repair Debride and reattach tendon to bone |
| R | Rehabilitation early Begin gentle ROM at 2 weeks |
| Y | Year for full recovery 12 months to return to sport/work |
| S | Six months failed conservative Minimum duration before considering surgery | G | Grip the bone Decorticate epicondyle for healing | Y | Year for full recovery 12 months to return to sport/work |
| U | Ulnar nerve protection Identify, protect, consider transposition | E | Excise and repair Debride and reattach tendon to bone | ||
| R | Remove degenerative tissue Debride abnormal tendon origin | R | Rehabilitation early Begin gentle ROM at 2 weeks |
Hook:SURGERY is a last resort - protect the ulnar nerve and be prepared for long rehab
Overview and Epidemiology
Medial epicondylitis, commonly known as golfer's elbow, is a degenerative tendinopathy of the flexor-pronator muscle origin at the medial epicondyle of the humerus. Despite the name, it affects a wide range of individuals beyond golfers.
Pathophysiology:
- Degenerative process, not inflammatory (tendinosis, not tendinitis)
- Repetitive microtrauma to flexor-pronator origin
- Angiofibroblastic degeneration with collagen disorganization
- Mucoid degeneration and microtearing
- Failed healing response
Terminology Matters
Modern understanding recognizes this as tendinosis (degenerative) rather than tendinitis (inflammatory). Histology shows angiofibroblastic hyperplasia, not inflammatory cells. This is why rest and anti-inflammatories alone often fail.
Risk factors and demographics:
Occupational Risk
- Manual laborers (carpenters, plumbers)
- Repetitive gripping and lifting
- Forceful wrist flexion activities
- Computer work (prolonged typing)
Athletic Risk
- Golf (improper swing mechanics)
- Baseball (pitchers - valgus overload)
- Tennis (heavy topspin forehand)
- Racquet sports (wrist-heavy strokes)
- Weightlifting (heavy deadlifts, rows)
Natural history:
- Most cases (90%) resolve with conservative treatment within 6-12 months
- Chronic cases (more than 12 months) more likely to require intervention
- Bilateral involvement in 10-20% of cases
- Recurrence rate 5-10% after successful treatment
Anatomy and Pathophysiology
Flexor-pronator origin anatomy:
The common flexor origin arises from the anterior aspect of the medial epicondyle and comprises:
Superficial layer (4 muscles):
- Pronator teres (PT) - most commonly affected, medial head origin
- Flexor carpi radialis (FCR) - most commonly affected tendon
- Palmaris longus (PL) - absent in 15% of population
- Flexor carpi ulnaris (FCU) - has dual origin (humeral and ulnar heads)
Deep layer (4 muscles):
- Flexor digitorum superficialis (FDS)
- Flexor digitorum profundus (FDP)
- Flexor pollicis longus (FPL)
- Pronator quadratus (PQ)
Pronator Teres and FCR - Key Structures
The pronator teres (medial head) and flexor carpi radialis are the primary structures involved in medial epicondylitis. The PT is the most medial and superficial muscle, making it vulnerable to overuse. FCR has the most robust tendinous origin and bears significant loads during wrist flexion.
Ulnar collateral ligament (UCL):
- Lies deep to the flexor-pronator mass
- Anterior bundle is primary valgus stabilizer
- Origin: anteroinferior aspect of medial epicondyle
- Insertion: sublime tubercle of ulna
- Critical to differentiate UCL injury from medial epicondylitis in overhead athletes
Ulnar nerve anatomy:
Ulnar Nerve Anatomical Relations
| Structure | Location | Clinical Significance |
|---|---|---|
| Cubital tunnel | Posterior to medial epicondyle | Site of compression in 50% of medial epicondylitis patients |
| Arcade of Struthers | 8-10cm proximal to medial epicondyle | First potential compression site |
| Osborne's ligament | Roof of cubital tunnel (FCU aponeurosis) | Common site of compression, thickened in chronic cases |
| Deep flexor-pronator aponeurosis | Between humeral and ulnar heads of FCU | Third compression zone distal to tunnel |
Pathophysiology
Mechanism of Tendinosis Development
Medial epicondylitis is fundamentally a tendinosis (degenerative) rather than tendinitis (inflammatory). The pathophysiology involves a failed healing response to repetitive microtrauma.
Phase 1: Microtrauma
- Repetitive eccentric loading during wrist flexion
- Microtears in tendon substance
- Pronation forces add torsional stress to the common flexor origin
Phase 2: Failed Healing Response
- Angiofibroblastic degeneration
- Disorganized collagen (Type III replaces normal Type I)
- Neovascularization and nerve ingrowth (neoinnervation is the source of chronic pain)
- Substance P and CGRP upregulation in degenerate tissue
Phase 3: Chronic Tendinosis
- Mucoid degeneration with grey, friable tissue
- Tendon thickening and structural weakness
- Potential for partial or complete tearing
- Loss of normal hierarchical collagen structure
Histopathology:
- NOT inflammatory - absence of inflammatory cells
- Hypercellular fibroblast proliferation
- Ground substance accumulation (mucoid change)
- Disorganized collagen fibers without normal crimp pattern
- Focal necrosis in severe cases
Why PT vs Surgery?
Physiotherapy focuses on eccentric strengthening to stimulate collagen remodeling and restore Type I collagen architecture. This works in 90% because the tendon retains healing capacity if mechanical overload is removed. Surgery is reserved for true failed healing when conservative measures cannot stimulate repair.
Classification and Severity Grading
Nirschl Classification (Most Common)
Clinical staging based on pain severity and functional limitation:
| Phase | Symptoms | Functional Impact | Treatment |
|---|---|---|---|
| Phase 1 | Mild pain after activity, self-limiting | No impact on sport or work | Activity modification, ice |
| Phase 2 | Pain during activity, doesn't limit performance | Minimal impact, able to continue | PT, NSAIDs, activity modification |
| Phase 3 | Pain during and after activity | Limits performance in sport/work | PT, injection consideration |
| Phase 4 | Pain during activity, unable to perform | Significant functional limitation | Aggressive conservative, injection |
| Phase 5 | Pain at rest and with activity | Unable to work or participate in sport | Consider surgical debridement |
Nirschl Phases Guide Treatment
Phases 1-3 respond well to conservative treatment. Phase 4 may need injection. Phase 5 (persistent symptoms at rest) is the surgical indication after 6 months of failed conservative care. The key is that pain progresses from post-activity to during-activity to at-rest.
Clinical Presentation and Assessment
History:
Symptom Pattern
- Location: Medial elbow pain radiating into forearm flexors
- Character: Aching, burning, worse with use
- Timing: Worse with gripping, lifting, wrist flexion
- Progression: Initially post-activity, then during activity, finally at rest
- Night pain: Suggests severe or chronic tendinosis
Functional Impact
- Weakness: Grip strength reduced, difficulty opening jars
- Activities: Pain with golf swing, throwing, racquet sports
- Work: Difficulty with keyboard, tools, heavy lifting
- Daily living: Trouble shaking hands, turning doorknobs
Physical examination:
Systematic Examination
Look: Swelling rare, assess carrying angle, look for muscle atrophy (chronic cases or if ulnar neuropathy)
Point tenderness: Maximum tenderness 5-10mm distal and anterior to medial epicondyle (flexor-pronator origin). Compare to UCL (more posterior and distal).
Active and passive: Usually full ROM. Pain at terminal extension (stretches flexors). Pronation/supination should be compared to contralateral side.
Grip strength: Reduced compared to contralateral (Jamar dynamometer objective measurement). Resisted wrist flexion: Reproduces pain (golfer's elbow test). Resisted pronation: Reproduces pain (pronator teres).
Golfer's elbow test: Elbow extended, forearm supinated, resist wrist flexion (reproduces medial elbow pain - POSITIVE). UCL stress: Valgus stress at 30 degrees flexion (should be negative unless concurrent UCL injury). Milking maneuver: Pull thumb with elbow flexed (valgus stress - assess UCL in overhead athletes).
Ulnar nerve: Tinel's at cubital tunnel, elbow flexion test (60 seconds), intrinsic muscle strength (first dorsal interosseous, abductor digiti minimi). Median nerve: Assess for pronator syndrome (rare association). Vascular: Radial pulse, capillary refill.
Golfer's Elbow Test - The Diagnostic Test
The golfer's elbow test is performed with the elbow extended, forearm supinated, and the examiner resisting active wrist flexion while palpating the medial epicondyle. A positive test reproduces the patient's medial elbow pain. This is highly specific for medial epicondylitis. Compare to lateral epicondylitis where resisted wrist extension reproduces lateral pain.
Investigations
Investigation Protocol
Medial epicondylitis is a clinical diagnosis. History and physical examination (golfer's elbow test positive, point tenderness at flexor origin) are usually sufficient. Imaging is not routinely required for diagnosis.
AP and lateral elbow X-rays. Usually normal. May show calcification in chronic cases (at flexor-pronator origin). Rule out bony pathology (arthritis, loose bodies, fracture). Stress views if UCL injury suspected.
MRI with and without contrast. Indications: Diagnostic uncertainty, suspected UCL injury, surgical planning, failed conservative treatment. Findings: Increased signal in flexor-pronator origin on T2/STIR, tendon thickening, partial tearing. Can assess UCL integrity.
NCS/EMG for ulnar nerve. Indications: Positive Tinel's, elbow flexion test, intrinsic weakness. Findings: Reduced conduction velocity across cubital tunnel, denervation in ulnar-innervated muscles if chronic. Guides need for cubital tunnel release.
Dynamic ultrasound. Operator-dependent. Can show tendon thickening, hypoechoic regions (degeneration), neovascularization on Doppler. Useful for guided injection. Less detail than MRI for UCL assessment.
MRI findings in medial epicondylitis:
T1-Weighted
- Normal to slightly low signal intensity
- Tendon thickening
- Loss of normal striated appearance
- Partial tearing appears as focal signal abnormality
T2-Weighted / STIR
- Increased signal intensity at flexor-pronator origin (edema, degeneration)
- Fluid signal if partial tear
- Peritendinous edema in acute exacerbations
- Bone marrow edema in chronic cases (stress reaction)
When to Order MRI
Order MRI if: (1) Diagnostic uncertainty (cannot distinguish from UCL injury), (2) Overhead athlete with medial pain (assess UCL), (3) Failed 3-6 months conservative treatment and considering surgery (surgical planning), (4) Suspected complete tendon rupture (rare but needs repair). MRI is not needed for typical medial epicondylitis responding to conservative care.
Imaging findings:
| Modality | Normal | Medial Epicondylitis | Complete Tear (Rare) |
|---|---|---|---|
| X-ray | Normal bone | May have calcification | Normal or calcification |
| Ultrasound | Fibrillar pattern | Hypoechoic, thickened, neovascularity | Tendon discontinuity |
| MRI T2 | Low signal | High signal at origin | High signal, tendon gap |
Management Algorithm
Conservative Treatment Protocol (First Line - 90% Success)
Goal: Reduce pain, restore function, promote tendon healing through eccentric strengthening and load management.
6-12 Month Conservative Protocol
Symptom control:
- Activity modification (avoid aggravating activities)
- Relative rest (not immobilization)
- Ice 15-20 minutes TDS
- NSAIDs (oral or topical) for 2 weeks
- Counterforce brace (below elbow, 2-3cm distal to epicondyle)
- Gentle ROM exercises (wrist flexion/extension, pronation/supination)
Physiotherapy program:
- Eccentric strengthening (key intervention - wrist flexion eccentrics)
- Isometric strengthening
- Stretching (wrist extensors and flexors)
- Progressive loading
- Activity modification continues
- Return to light activities as tolerated
Gradual return to activity:
- Continue eccentric program
- Sport-specific training (golf swing mechanics, throwing program)
- Progressive resistance exercises
- Gradual return to work activities
- Monitor symptoms
Consider injection:
- If persistent symptoms after 3 months of PT
- Corticosteroid injection (methylprednisolone 40mg + local anesthetic)
- Maximum 2-3 injections (tendon weakening risk)
- Platelet-rich plasma (PRP) alternative (less evidence but safer)
- Continue PT after injection
Eccentric Strengthening - The Key
Eccentric exercises are the cornerstone of tendinopathy rehabilitation. For medial epicondylitis, the patient performs wrist flexion with the affected hand, then uses the unaffected hand to extend the wrist (eccentric lowering against resistance). This stimulates collagen remodeling and tendon healing. Perform 3 sets of 15 repetitions, twice daily. Pain during exercise is acceptable; pain lasting more than 24 hours means reduce load.
Equipment and bracing:
- Counterforce brace: Worn 2-3cm distal to medial epicondyle, reduces load on tendon origin
- Wrist splint: Night splint in neutral position (reduces pain from nocturnal wrist flexion)
- Equipment modification: Lighter golf clubs, larger grip diameter, proper swing mechanics
These equipment modifications help reduce load on the flexor-pronator origin during the healing process.
Surgical Technique - Open Debridement and Repair
Pre-operative Planning
Consent Points
- Infection: 1-2% superficial, less than 1% deep
- Ulnar nerve injury: 2-5% (transient or permanent)
- Stiffness: 5-10% (elbow contracture)
- Recurrence: 10-15% (incomplete debridement)
- Prolonged recovery: 6-12 months to return to sport
- CRPS: Rare (less than 1%) but devastating
Equipment Checklist
- Tourniquet: Upper arm tourniquet (sterile field)
- Instruments: Standard orthopedic tray, rongeur, curette
- Sutures: Non-absorbable for tendon repair (FiberWire, Ethibond)
- Suture anchors: If bone quality poor (elderly, osteoporotic)
- Nerve retractors: Blunt Hohmann, small Richardson
- Magnification: Loupe magnification helpful for ulnar nerve
Patient Positioning
Setup Checklist
Supine on operating table, arm board extended at 90 degrees. Affected arm fully accessible. Head turned away from operative side.
Upper arm tourniquet applied (250-300mmHg for adults). Padding beneath tourniquet. May exsanguinate with Esmarch or gravity elevation (avoid if ulnar nerve symptoms).
Prep and drape: Prep from mid-humerus to fingertips, circumferentially. Free drape the arm to allow elbow flexion/extension intraoperatively. Confirm ulnar nerve palpable (identify before incision).
Surgical Approach
Step-by-Step Open Technique
Landmarks: Medial epicondyle (palpate). Incision: 5-7cm longitudinal incision centered over medial epicondyle, extending distally along flexor-pronator mass. Avoid excessive anterior curve (median nerve). Avoid excessive posterior curve (ulnar nerve). Technique: Sharp dissection through skin and subcutaneous tissue. Ligate or cauterize superficial veins. Identify medial antebrachial cutaneous nerve branches (retract or sacrifice if unavoidable).
Critical step: Identify the ulnar nerve in cubital tunnel before any tendon work. Technique: Palpate posterior to medial epicondyle. Gentle dissection through subcutaneous tissue. Identify nerve in cubital tunnel. Assess nerve for subluxation (over epicondyle with flexion). Assess cubital tunnel for Osborne's ligament thickening. Place vessel loop around nerve for gentle retraction (DO NOT OVER-RETRACT).
Ulnar Nerve - Protect at All Costs
The ulnar nerve is at risk during medial elbow surgery. Identify it early, protect throughout, and assess for need for decompression/transposition. If the nerve is tight, subluxes over the epicondyle, or patient has preoperative ulnar symptoms, perform in situ decompression (release Osborne's ligament and arcade of Struthers) or anterior transposition (subcutaneous or submuscular).
Technique: With ulnar nerve protected, expose flexor-pronator origin on anterior aspect of medial epicondyle.
- Longitudinal incision through tendon origin
- Split pronator teres and FCR at their origin
- May elevate tendon from bone subperiosteally
- Expose underlying bone (medial epicondyle)
- Assess for degenerative tissue (gray, friable, mucoid appearance)
Key step: Remove all degenerative tendon tissue. Technique:
- Identify abnormal tissue (gray, friable, no normal tendon architecture)
- Excise with scalpel or rongeur
- Debride back to healthy, bleeding tendon
- Avoid excessive resection (preserve UCL deep to flexor mass)
- Assess UCL integrity if athlete (should be intact - if torn, different pathology)
Goal: Create bleeding bone bed for tendon healing. Technique:
- Use curette or rongeur to remove cortical bone
- Create multiple small holes (drill or curette)
- Expose cancellous bone (punctate bleeding)
- Avoid excessive bone removal (weakens epicondyle)
Technique: Reattach flexor-pronator mass to medial epicondyle. Options:
- Bone tunnels (traditional): Drill 2-3 holes through epicondyle, pass non-absorbable sutures (FiberWire No. 2), tie over bone bridge
- Suture anchors (modern): Place 2-3 anchors in epicondyle, suture tendon to bone (allows earlier ROM)
- Side-to-side repair: If minimal debridement, repair split tendon edges Goal: Restore anatomic tension, avoid over-tightening (limits ROM)
Decision: Based on preoperative symptoms and intraoperative findings. If no preoperative symptoms and nerve healthy: No decompression needed, gentle inspection only. If preoperative symptoms or tight nerve: In situ decompression (release Osborne's ligament, arcade of Struthers). If nerve subluxes or severe symptoms: Anterior subcutaneous transposition (create subcutaneous pocket anterior to medial epicondyle, transpose nerve, secure with fascia sling).
Technical Pearls
Do's (Pearls)
- Identify ulnar nerve first - before any tendon work
- Complete debridement - remove all gray, degenerative tissue
- Decorticate bone - create bleeding bed for healing
- Protect UCL - lies deep, do not violate in non-athletes
- Early ROM - begin gentle motion at 2 weeks (if stable repair)
Don'ts (Pitfalls)
- Don't ignore ulnar nerve - 2-5% injury rate if not careful
- Don't undertake PT failure - must have tried 6 months conservative
- Don't over-tighten repair - causes elbow stiffness
- Don't excise normal tendon - only remove degenerative tissue
- Don't rush rehab - 6-12 months for full recovery
Ulnar Nerve Decision - In Situ vs Transposition
If the ulnar nerve has preoperative symptoms or is tight/subluxes intraoperatively, perform at minimum an in situ decompression (release Osborne's ligament and arcade of Struthers). If nerve subluxes over the medial epicondyle with flexion or severe preoperative neuropathy, perform anterior subcutaneous transposition. Submuscular transposition is reserved for revision cases or severe arthrofibrosis risk.
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Ulnar nerve injury | 2-5% (transient or permanent) | Failure to identify nerve, excessive retraction, thermal injury | If transient: observation, nerve glides. If permanent: nerve exploration, neurolysis, possible transposition |
| Recurrent symptoms | 10-15% | Incomplete debridement, early return to activity, poor rehab compliance | Prolonged PT, activity modification. If persistent: revision surgery with more extensive debridement |
| Elbow stiffness | 5-10% | Prolonged immobilization, aggressive surgery, patient factors (diabetes, smoking) | Prevention: early ROM. Treatment: dynamic splinting, manipulation under anesthesia if severe |
| Wound infection | 1-2% superficial, less than 1% deep | Diabetes, immunosuppression, contamination | Superficial: oral antibiotics, wound care. Deep: surgical debridement, IV antibiotics, possible hardware removal |
| Medial epicondyle fracture | Rare (less than 1%) | Excessive bone removal during decortication, osteoporotic bone | If stable: immobilization, protected ROM. If displaced: ORIF with screws or plate |
| CRPS | Less than 1% | Genetic predisposition, nerve injury, prolonged immobilization | Early recognition critical. Multimodal pain management, PT, sympathetic blocks, mirror therapy |
| Medial antebrachial cutaneous nerve injury | 5-10% (numbness only) | Nerve runs through surgical field, may need to be sacrificed | Counsel preoperatively. Usually resolves. Persistent numbness well-tolerated |
Ulnar Nerve Injury - Most Serious Complication
Ulnar nerve injury (2-5% incidence) is the most serious complication. Causes: failure to identify and protect nerve, excessive retraction, thermal injury from cautery, suture entrapment. Prevention: Identify nerve before tendon work, use vessel loop for gentle retraction, avoid cautery near nerve, assess nerve at end of case (passive elbow flexion/extension - nerve should glide freely). If nerve injury suspected postoperatively (new intrinsic weakness, worsening paresthesias), obtain urgent NCS and consider early exploration.
Recurrent symptoms management:
- Most common cause: incomplete debridement (gray tissue left behind)
- Second most common: early return to activity (reinjury)
- Third: poor rehabilitation compliance
Revision surgery if conservative fails again:
- MRI to assess extent of recurrent pathology
- More extensive debridement (may need larger exposure)
- Consider ulnar nerve transposition if not done at index surgery
- Counsel realistic expectations (lower success rate, 70-80%)
Postoperative Care and Rehabilitation
Standard Postoperative Rehabilitation
Rehabilitation Timeline After Open Debridement
- Posterior splint at 90 degrees flexion, neutral rotation
- Elevation, ice packs
- Finger ROM encouraged (prevent stiffness, promote circulation)
- Wound care, dressing change at 48 hours
- Pain management (NSAIDs, opioids short-term if needed)
- Remove splint at 7-14 days (based on repair strength)
- Begin gentle active ROM (elbow flexion/extension, forearm rotation)
- Avoid resisted wrist flexion (protect repair)
- No lifting (protect tendon repair)
- Removable splint for comfort/protection between exercises
- Active ROM - full elbow and forearm motion expected by 6 weeks
- Light ADLs - typing, light household tasks
- Gentle stretching - wrist flexors and extensors
- No resisted strengthening yet
- No lifting more than 1kg
- Begin isometric strengthening (wrist flexion, pronation)
- Progress to eccentric exercises (key for tendon remodeling)
- Grip strengthening (putty, stress ball, then Jamar dynamometer)
- Light resistance exercises (1-2kg)
- Sport-specific training begins (golf swing mechanics, throwing program)
- Progressive resistance strengthening
- Return to work: Desk work 6-8 weeks, manual labor 3-6 months
- Return to sport: Golf/tennis 4-6 months, overhead throwing 6-9 months
- Monitor for recurrent symptoms
- Full strength expected by 12 months
- Unrestricted activities
- Ongoing maintenance exercises (eccentric program)
- Return to baseline function in 80-90% of patients
Balance Early Motion with Protection
Postoperative rehabilitation requires balancing early motion to prevent stiffness with protecting the tendon repair to allow healing. Modern approach favors early gentle ROM (starting at 1-2 weeks) to prevent elbow contracture, but delay resisted strengthening until 6 weeks to allow tendon-to-bone healing. Eccentric exercises begin at 6 weeks and are key to tendon remodeling and preventing recurrence.
Outcomes and Prognosis
Outcomes with conservative treatment:
| Timeframe | Success Rate | Key Factors |
|---|---|---|
| 3 months | 50-60% improvement | PT compliance, activity modification |
| 6 months | 75-85% resolution | Eccentric exercises, load management |
| 12 months | 90% resolution | Natural healing, tendon remodeling |
Outcomes with surgical treatment:
| Outcome Measure | Success Rate | Prognostic Factors |
|---|---|---|
| Good/excellent result | 80-90% | Complete debridement, proper rehab, 6+ months conservative trial |
| Return to sport/work | 85-90% | Pre-injury level, 6-12 months timeline, realistic expectations |
| Recurrence | 10-15% | Incomplete debridement, early return to activity, poor compliance |
| Ulnar nerve symptoms | Improve in 80-90% if transposed | Preoperative severity, duration of symptoms, transposition technique |
Predictors of poor outcome:
Poor Prognostic Factors
Poor outcomes (recurrence, persistent pain) associated with: (1) Workers' compensation/litigation (controversial but documented), (2) Concurrent psychiatric comorbidity (depression, anxiety), (3) Short duration conservative trial (less than 6 months), (4) Smoking (impairs tendon healing), (5) Diabetes (healing impairment), (6) Bilateral symptoms (systemic factors). Counsel patients realistically if these present.
Comparison: Conservative vs Surgical:
| Outcome | Conservative (6-12 months) | Surgical (after failed conservative) |
|---|---|---|
| Success rate | 90% | 80-90% |
| Return to activity | 6-12 months | 6-12 months post-surgery |
| Complications | Minimal (injection risks) | 5-10% (nerve, infection, stiffness) |
| Cost | Low | Moderate-high |
| Recurrence | 5-10% | 10-15% |
Controversies and Areas of Uncertainty
Injection Therapy
- Corticosteroid: RCT evidence (Stahl & Kaufman) shows only 6-week benefit with no advantage by 3-12 months - many now question routine use
- PRP: Higher-level evidence exists for lateral, not medial, epicondylitis; medial-specific data are sparse and benefit (if any) is delayed by months
- No injectable is proven to alter long-term natural history
Surgical Technique & Nerve
- Open vs arthroscopic vs percutaneous debridement: no high-quality comparative trials; open remains the reference standard
- Ulnar nerve: when to decompress versus transpose in mild/intermittent neuritis is not standardised
- Eccentric loading: cornerstone of rehab but optimal dose, frequency and pain-monitoring threshold remain debated
The Honest Examiner Answer
If asked about controversy, state plainly that medial epicondylitis is under-studied compared with lateral disease: the surgical evidence base is largely Level 4 case series, the single best injection trial (Stahl & Kaufman) is negative beyond 6 weeks, and PRP recommendations are extrapolated from lateral epicondylitis. This justifies a conservative-first, exercise-led, shared-decision approach.
Evidence Base and Key Trials
Operative Treatment of Medial Epicondylitis - Influence of Concomitant Ulnar Neuropathy
- Retrospective review of 30 elbows (26 patients) treated by flexor-pronator debridement with ulnar nerve decompression/transposition when indicated, mean follow-up 7 years
- Overall 87% good or excellent results; resisted forearm pronation was the most sensitive provocative test (positive in 28 of 30 elbows)
- Outcome was strongly modulated by ulnar neuropathy severity: 24/25 elbows with no or mild neuropathy (type IA/IB) did well, versus only 2/5 elbows with moderate/severe neuropathy (type II) (p = 0.009)
- Grading the associated ulnar neuropathy is essential for prognosis and operative planning
Surgical Treatment of Medial Epicondylitis - Results in 35 Elbows
- Reviewed 35 of 38 consecutive elbows treated operatively after failed conservative care, mean follow-up 85 months
- Residual tears with incomplete healing were consistently found in the flexor origin; histology showed reactive fibrous connective tissue with variable inflammation
- Mean subjective elbow function improved from 38% to 98% of normal; 25 excellent, 9 good, 1 fair (86% with no limitation)
- Isokinetic and grip strength returned to the level of the unoperated elbow
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Classic Presentation - Initial Assessment (2-3 min)
"A 42-year-old male recreational golfer presents with 4 months of medial elbow pain. Pain is worse after playing golf and with gripping activities. No history of trauma. Examination shows point tenderness at the medial epicondyle and pain with resisted wrist flexion. How would you assess and manage this patient?"
Scenario 2: Surgical Technique - Operative Management (3-4 min)
"A 38-year-old manual laborer has failed 9 months of conservative treatment for medial epicondylitis. He has severe pain affecting his ability to work. MRI shows degenerative changes at the flexor-pronator origin. He also has intermittent paresthesias in the small and ring fingers with positive Tinel's at the cubital tunnel. You plan surgical debridement. Walk me through your operative approach."
Scenario 3: Complication Management - Ulnar Nerve Injury (2-3 min)
"You performed open debridement and repair for medial epicondylitis without ulnar nerve transposition (nerve appeared healthy intraoperatively). The patient returns 2 weeks postoperatively with new onset numbness in the small and ring fingers, and weakness of finger abduction (first dorsal interosseous). What is your assessment and management?"
MCQ Practice Points
Anatomy Question
Q: Which muscles form the common flexor-pronator origin at the medial epicondyle, and which two are most commonly affected in medial epicondylitis? A: The superficial layer includes pronator teres, flexor carpi radialis, palmaris longus, and flexor carpi ulnaris. The pronator teres (medial head) and flexor carpi radialis are most commonly affected in medial epicondylitis.
Differential Diagnosis Question
Q: How do you distinguish medial epicondylitis from UCL injury in an overhead throwing athlete? A: UCL injury presents with valgus instability (positive valgus stress test at 30 degrees flexion, positive milking maneuver), pain during throwing (late cocking/acceleration phase), and MRI shows UCL thickening or tear. Medial epicondylitis presents with pain from resisted wrist flexion/pronation (golfer's elbow test), point tenderness at flexor-pronator origin (more anterior than UCL), and no valgus instability.
Conservative Treatment Question
Q: What is the most effective conservative treatment for medial epicondylitis and what is the expected success rate? A: Eccentric strengthening exercises are the most effective conservative intervention. The patient performs wrist flexion with the affected hand, then uses the unaffected hand to extend the wrist (eccentric lowering against resistance). Combined with activity modification, NSAIDs, and bracing, 90% of patients improve within 6-12 months of conservative treatment.
Ulnar Nerve Question
Q: What percentage of medial epicondylitis patients have concurrent ulnar nerve symptoms, and how should this be assessed? A: 50% of patients with medial epicondylitis have concurrent ulnar neuritis. Assess with Tinel's sign at the cubital tunnel, elbow flexion test (hold elbow flexed for 60 seconds), and intrinsic hand muscle strength. If positive, order nerve conduction studies. At surgery, perform at minimum in situ decompression (release Osborne's ligament); if nerve subluxes or severe symptoms, consider anterior transposition.
Surgical Indication Question
Q: What are the indications for surgical treatment of medial epicondylitis? A: Indications: (1) Failed conservative treatment for minimum 6 months (including PT, activity modification, NSAIDs, bracing, and possibly injection), (2) Persistent pain affecting work or quality of life, (3) Structural damage on MRI (large partial tear, complete disruption), (4) Patient preference after informed discussion with realistic expectations. Surgery should NOT be offered before 6 months of conservative trial.
Complications Question
Q: What is the most serious complication of medial epicondylitis surgery and how can it be prevented? A: Ulnar nerve injury (2-5% incidence) is the most serious complication. Prevention strategies: (1) Identify the ulnar nerve BEFORE any tendon work (palpate in cubital tunnel, protect with vessel loop), (2) Avoid excessive retraction, (3) Avoid cautery near nerve (thermal injury), (4) Assess nerve at end of case (should glide freely with elbow flexion/extension), (5) If preoperative ulnar symptoms, perform in situ decompression or transposition.
Guidelines, Registries & Global Practice
Global epidemiology:
Population Burden
- Point prevalence ~0.4% of working-age adults (Finnish population study), versus ~1.3% for lateral epicondylitis - medial disease is roughly 3x less common
- Peak incidence age 45-54, no consistent sex difference
- Accounts for an estimated 10-20% of all elbow epicondylar tendinopathies
- Independent risk factors: repetitive plus forceful work, smoking, obesity, diabetes
At-Risk Activities Worldwide
- Throwing/overhead sports: baseball pitching, javelin, cricket fast bowling (valgus overload)
- Golf and racquet sports: wrist-flexion- and pronation-dominant strokes
- Manual occupations: construction, plumbing, carpentry, assembly-line work
- Strength sports: heavy deadlifts, rows, repetitive gripping
Society guidance, side by side:
How Major Bodies Frame Epicondylar Tendinopathy
| Body / Region | Core Position | Injection Stance | Surgical Threshold |
|---|---|---|---|
| AAOS / AOSSM (US) | Load management plus eccentric/progressive flexor-pronator rehabilitation as first line; emphasise tendinosis biology | Corticosteroid for short-term relief only; PRP optional in recalcitrant cases (evidence evolving) | Open debridement after 6+ months of failed structured conservative care |
| NICE / BOA (UK) | Reassurance and self-management; most epicondylar tendinopathy is self-limiting over 6-24 months | Limit corticosteroid injections; caution re: worse long-term outcomes; PRP not routinely recommended | Surgery only for genuinely refractory, well-localised disease |
| EFORT / European consensus | Exercise-based therapy central; address ergonomic and lifestyle risk factors (smoking, load) | Injectables adjunctive, not curative; shared decision-making | Reserve for failed multimodal conservative programme |
| Resource-variable settings | Activity modification, simple analgesia and home eccentric programmes form the mainstay | Steroid injection where available; PRP often inaccessible (cost/equipment) | Open debridement (no arthroscopy/anchors required) where surgery is indicated |
Why Guidelines Converge
Across AAOS, NICE/BOA and EFORT the message is consistent: medial epicondylitis is a load-related tendinosis that is largely self-limiting, exercise (eccentric/progressive loading) is the highest-value intervention, and corticosteroid offers only short-term relief (Stahl & Kaufman RCT). Surgery is uniformly a last resort after a minimum 6-month structured conservative trial.
Registry and outcome notes:
- Medial epicondylitis involves no implant, so it is not tracked by arthroplasty registries (NJR, AJRR, AOANJRR). Outcome evidence therefore rests on case series (Gabel & Morrey; Vangsness & Jobe) and a small number of RCTs (Stahl & Kaufman; epicondylar PRP trials).
- Reported good/excellent surgical outcomes cluster around 85-90%, consistent across decades and health systems.
- The most robust prognostic signal across series is concomitant ulnar neuropathy severity, not geography.
High- versus limited-resource practice variation:
Practice Variation by Resource Setting
| Element | Well-Resourced Settings | Limited-Resource Settings | Reason for Difference |
|---|---|---|---|
| Diagnosis | Clinical, with MRI/ultrasound available for uncertainty or surgical planning | Clinical diagnosis alone; imaging often unavailable | Medial epicondylitis is fundamentally a clinical diagnosis - advanced imaging is confirmatory, not essential |
| Rehabilitation | Supervised physiotherapy with progressive loading and dynamometry | Home-based eccentric programme with printed/verbal instruction | The active ingredient (eccentric loading) is achievable without equipment |
| Injections | Image-guided corticosteroid; PRP available (often self-funded) | Landmark-guided steroid where available; PRP usually inaccessible | PRP requires centrifugation, cost and remains evidence-limited |
| Surgery | Open or arthroscopic debridement, suture anchors, formal nerve transposition | Open debridement with bone tunnels; in situ ulnar decompression | Open technique with bone tunnels delivers comparable results without implants |
Documentation - Universally Important
Regardless of health system, two records protect both patient and surgeon: (1) a documented preoperative ulnar nerve examination (Tinel's, elbow flexion test, intrinsic strength) - essential if postoperative neuropathy arises, and (2) evidence of a minimum 6-month structured conservative trial before surgery. Consent should specifically cover ulnar nerve injury (2-5%), recurrence (10-15%) and prolonged recovery (6-12 months).
MEDIAL EPICONDYLITIS (GOLFER'S ELBOW)
Clinical summary
Key Anatomy
- •Flexor-pronator origin: PT (most medial), FCR (most affected), PL, FCU
- •Ulnar nerve: 50% concurrent neuritis - assess Tinel's, elbow flexion test
- •UCL: Deep to flexor mass, assess valgus stress (exclude injury in athletes)
- •Pathology: Angiofibroblastic tendinosis (degenerative), not inflammatory
Clinical Assessment
- •Golfer's elbow test: Resisted wrist flexion reproduces medial pain (POSITIVE)
- •Point tenderness: 5-10mm distal and anterior to medial epicondyle
- •Differential: UCL injury (valgus stress), cubital tunnel syndrome, cervical radiculopathy
- •Always assess ulnar nerve: Tinel's, elbow flexion test, intrinsic strength
Treatment Algorithm
- •Conservative first line (90% success): PT (eccentric exercises), NSAIDs, activity modification, brace
- •Duration: 6-12 months for resolution with conservative care
- •Injection: Consider at 3-6 months if persistent (corticosteroid or PRP)
- •Surgery: Only after 6 months failed conservative - open debridement and repair
Surgical Pearls
- •Identify ulnar nerve FIRST (before tendon work) - protect with vessel loop
- •Debride all degenerative tissue (gray, friable) back to healthy tendon
- •Decorticate medial epicondyle (create bleeding bone bed for healing)
- •If preoperative ulnar symptoms: in situ decompression or transposition
- •Early ROM at 2 weeks, eccentric strengthening at 6 weeks, return to sport 6-12 months
Complications
- •Ulnar nerve injury: 2-5% (most serious - prevention is key)
- •Recurrence: 10-15% (incomplete debridement, early return to activity)
- •Stiffness: 5-10% (early ROM prevents)
- •Infection: 1-2% superficial, less than 1% deep