Posterior Meniscocapsular Separation | ACL Associated | Hidden Lesion
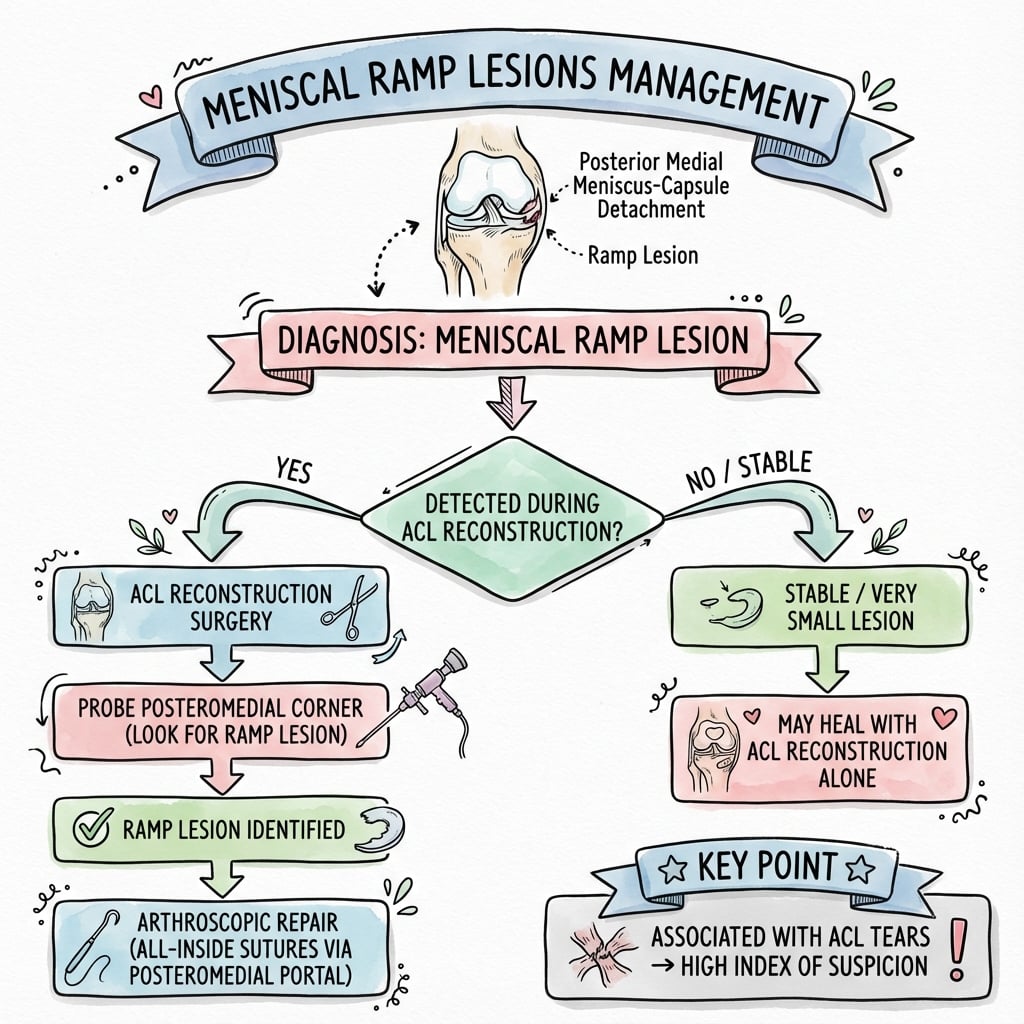
- Ramp lesion = peripheral posterior horn medial meniscus tear at the meniscocapsular/meniscotibial junction
- Roughly 24-40% of ACL tears have an associated ramp lesion
- MRI is unreliable (sensitivity ~27-50%) - a normal scan does NOT exclude a ramp lesion
- Always view posteromedially (trans-notch / posteromedial portal) during ACL reconstruction
- All-inside or suture-hook repair through a posteromedial portal is the workhorse technique
- “Ramp lesions increase anterior tibial translation in the ACL-deficient knee (about 2.6mm, Peltier 2015)
- “Pivot shift is restored only when ACLR is combined with ramp repair (DePhillipo 2018)
- “Located in the peripheral vascular (red-red) zone, giving good healing potential
- “Small stable ramp lesions may not need fixation once the ACL is reconstructed (Deichsel 2024) - controversial
Ramp lesions are easily missed - MRI sensitivity is only about 27-50%, and they are often invisible from standard anterior portals. About 17% are 'hidden' even arthroscopically until a posteromedial portal and minimal debridement are used (Sonnery-Cottet 2014).
Roughly 24-40% of ACL tears have ramp lesions. Prevalence tends to rise with chronicity and is similar in adolescents and adults. Always suspect with any ACL injury.
Ramp lesions increase anterior tibial translation by disrupting the posterior horn-capsule complex. This may stress ACL grafts and contribute to failure if unaddressed.
Located in the peripheral red-red zone with good vascularity from the perimeniscal capsular plexus, giving a favourable environment for repair healing compared with central avascular tears.
| Finding | Classification | Treatment | Key Pearl |
|---|---|---|---|
| Small separation under 4mm, stable | Type 1-3 stable | May observe if truly stable | Probe to confirm stability |
| Separation greater than 4mm | Type 1-3 unstable | Repair through posteromedial portal | Gap indicates need for repair |
| Complete double lesion | Type 4 | Must repair all-inside technique | High instability without repair |
| Body tear extension | Type 5 | Repair ramp + body lesion | Address both components |
RAMPRAMP - Key Concepts
Hook:RAMP lesions are on the RAMP up to the capsule - in the red zone where ACL tears pull them apart!
PROBEPROBE - Systematic Assessment
Hook:Always PROBE posteromedially during ACL surgery - you'll miss hidden lesions if you don't!
1-2-3-4-5Thaunat Classification
Hook:Types go from simple (1) to complex (5) - higher numbers need more repair!
Overview and Epidemiology
Ramp lesions were historically under-recognized. With improved arthroscopic techniques and awareness, they are now routinely identified during ACL surgery. Failure to address ramp lesions may contribute to ACL graft failure and persistent rotational instability.
- Younger age (under 30)
- Male gender
- High-grade pivot shift
- Chronic ACL injury (delayed presentation)
- Contact sport mechanism
- Posterior horn medial meniscus
- Meniscocapsular junction
- Red-red zone (peripheral 1/3)
- Near posteromedial capsule
Anatomy and Biomechanics
The "ramp" refers to the sloping posterior meniscocapsular junction of the medial meniscus. This junction connects the posterior horn to the posteromedial capsule and is stressed during ACL injury mechanisms (pivot shift). Disruption creates instability.
- Location: Posterior horn of medial meniscus at capsular junction
- Zone: Red-red (peripheral, vascular)
- Blood supply: From posteromedial capsule and meniscocapsular vessels
- Function: Posterior stabilizer, secondary restraint to anterior translation
- Pivot shift mechanism stresses posterior meniscocapsular junction
- Anterior tibial translation pulls on posterior horn
- Rotational component shears capsular attachment
- Higher grades of pivot shift = higher ramp lesion rate
| Parameter | Intact Ramp | Ramp Lesion | After Repair |
|---|---|---|---|
| Anterior translation | Baseline | Increased 2-3mm | Restored |
| Rotational stability | Normal | Decreased | Restored |
| ACL graft stress | Normal | Increased | Normalized |
| Posterior horn function | Normal | Compromised | Restored |
The posterior medial meniscocapsular complex acts as a secondary stabilizer to anterior tibial translation. In the ACL-deficient knee, unrepaired ramp lesions increase laxity and may stress the ACL reconstruction, potentially contributing to graft failure.
Pathophysiology
Mechanism of Injury
Ramp lesions occur through the same mechanism as ACL injuries:
- Pivot shift mechanism: Combined knee flexion, valgus, and internal tibial rotation
- Tibial translation: Anterior tibial translation during ACL rupture shears the posterior meniscocapsular junction
- Contact mechanism: Direct blow to lateral knee with foot planted
Why Posterior Horn?
The posteromedial corner is vulnerable because:
- The posterior horn medial meniscus is fixed to the tibia via coronary ligament
- During anterior tibial translation, the femoral condyle impinges on the posterior horn
- This creates a "grinding" effect between femoral condyle and tibial plateau
- Combined with rotational force, the meniscocapsular junction tears
Relationship to ACL Deficiency
In the ACL-deficient knee:
- Posterior medial meniscocapsular complex acts as secondary stabilizer
- Restrains anterior tibial translation
- Unrepaired ramp lesion increases rotatory laxity
- May overload ACL reconstruction leading to graft failure
- This is why concurrent repair during ACLR is critical
Natural History
Without repair:
- Progressive meniscocapsular separation
- Increased knee laxity despite ACL reconstruction
- Potential accelerated cartilage degeneration
- Higher risk of re-rupture or graft failure
Classification Systems
Thaunat Classification (2016)
| Type | Description | Stability | Treatment |
|---|---|---|---|
| Type 1 | Meniscocapsular separation (peripheral only) | Variable | Repair if gap greater than 4mm or unstable |
| Type 2 | Partial superior leaf lesion | Often stable | Repair if unstable on probing |
| Type 3 | Partial inferior leaf lesion | Often stable | Repair if unstable on probing |
| Type 4 | Double lesion (complete separation) | Unstable | Must repair - complete instability |
| Type 5 | Lesion extending into meniscal body | Unstable | Repair both ramp and body components |
The majority of ramp lesions are peripheral meniscocapsular/meniscotibial separations located in the vascular red-red zone, giving them favourable healing potential. The exam point is the principle: classify by tear pattern (partial vs full thickness) and meniscotibial integrity, and decide repair by stability on probing rather than by type number alone.
Clinical Assessment
- Mechanism: Pivot shift injury (usually with ACL)
- Presentation: Often masked by ACL symptoms
- Pain: Posteromedial joint line (may be subtle)
- Instability: Giving way, especially rotational
- Chronicity: Duration since ACL injury
- Joint line: Posterior medial tenderness (subtle)
- ACL tests: Positive Lachman, pivot shift
- Pivot shift grade: Higher grade = higher ramp risk
- McMurray: Often negative for ramp alone
- Deep squat: May reproduce posterior pain
Ramp lesions rarely have distinctive clinical findings separate from the associated ACL tear. The diagnosis is primarily made on MRI and confirmed at arthroscopy. Always maintain high clinical suspicion in any ACL tear, especially with:
- High-grade pivot shift
- Delayed presentation (over 6 months)
- Young male athletes
Investigations
Imaging Protocol
3T preferred. Dedicated sequences for posterior horn. Look for: meniscocapsular separation, increased signal at junction, irregularity of posterior horn periphery, posteromedial tibial bone bruise. Low sensitivity (around 27-50%) - a negative MRI does not exclude a ramp lesion.
Sagittal: Assess posterior horn integrity, look for separation sign. Coronal: Look for peripheral irregularity and increased signal at meniscocapsular junction.
Gold standard for diagnosis. Systematic probing of posteromedial compartment mandatory during all ACL reconstructions. 70° scope improves visualization.
| Sign | View | Description | Reliability |
|---|---|---|---|
| Meniscocapsular separation | Sagittal | Gap between posterior horn and capsule | High if present |
| Increased peripheral signal | Coronal/Sagittal | T2 hyperintensity at junction | Moderate |
| Irregular posterior horn contour | Sagittal | Abnormal peripheral margin | Moderate |
| Perimeniscal fluid | All planes | Fluid tracking along capsule | Low specificity |
MRI has poor sensitivity for ramp lesions (about 27-50% in dedicated series, lowest for true meniscocapsular-junction tears). This is why arthroscopic assessment is mandatory during ACL reconstruction. Do not rely solely on MRI to rule out a ramp lesion - always view trans-notch and probe posteromedially. A posteromedial tibial bone bruise on MRI is a useful indirect clue.
Management Algorithm
When to Repair
Absolute Indications:
- Type 4 (double) lesion
- Type 5 (body extension)
- Gap greater than 4mm on probing
- Frank instability on probing
Relative Indications:
- Smaller stable lesions in young athletes
- High-demand patients
- Concomitant ACL reconstruction
May Observe:
- Truly stable Type 1-3 lesions (probe test stable)
- Low-demand elderly patients
- Contraindication to prolonged rehabilitation
Given the excellent healing potential (red-red zone) and minimal morbidity of repair, most surgeons advocate for repair of any visualized ramp lesion during ACL reconstruction, especially in young athletes.
Surgical Technique
All-Inside Repair Technique
Gold standard for ramp lesion repair during ACL reconstruction.
Surgical Steps
Use 70° arthroscope through anterolateral portal to view posteromedial compartment. Alternatively, create posteromedial viewing portal. Must see entire posterior horn-capsule junction.
Debride tear edges with shaver (minimal). Rasp meniscal and capsular surfaces to stimulate bleeding and healing response. Do not over-debride.
Create posteromedial working portal. Use spinal needle to confirm trajectory. Avoid saphenous nerve (stay anterior to sartorius). Entry typically 1cm above joint line, posterior to MCL.
Use all-inside meniscal repair device (FasT-Fix, ULTRA FasT-Fix, etc.). Pass sutures through meniscus then into capsule. Typically 1-3 sutures depending on lesion length.
Tension sutures to reduce meniscus to capsule. Confirm reduction with probe. Verify no gap remains and meniscus is stable.
- 70° scope essential for visualization
- Posteromedial portal allows direct access
- Rasp both surfaces for healing
- All-inside devices simplify repair
- Usually 1-3 sutures sufficient
- Missing the lesion (probe systematically)
- Saphenous nerve injury (portal placement)
- Over-debridement (lose tissue)
- Inadequate reduction (check after suturing)
- Not addressing associated body tear
Complications
| Complication | Incidence | Risk Factors | Prevention/Management |
|---|---|---|---|
| Failure to heal | Under 10% | Poor technique, inadequate fixation | Adequate sutures, good reduction |
| Saphenous nerve injury | Rare | Portal placement | Careful PM portal creation |
| Stiffness | 5-10% | Prolonged immobilization | Early ROM protocol |
| Re-tear | Under 5% | Trauma, early return to sport | Protected rehabilitation |
| Missed lesion | Variable | Poor visualization technique | Systematic probing every case |
Failure to identify and repair a ramp lesion during ACL reconstruction may contribute to:
- Persistent rotational instability
- Increased stress on ACL graft
- Potential ACL graft failure
- Residual symptoms
Always probe posteromedially during ACL surgery!
Postoperative Care and Rehabilitation
Rehabilitation with ACL Reconstruction
Protocol follows ACL rehab with minor modifications:
Combined ACL + Ramp Repair Protocol
Brace locked or 0-90°. Partial weight-bearing with crutches. Quad sets, straight leg raises. Avoid forced flexion beyond 90°.
Progressive ROM to full. Advance weight-bearing. Closed chain strengthening. Avoid deep squats.
Full weight-bearing. Progressive resistance training. Stationary cycling, swimming. Avoid pivoting.
Jogging progression. Agility drills begin. Sport-specific training. Functional testing.
Return to non-contact sport if criteria met. Full return 9-12 months. Follows ACL return-to-sport criteria.
Because ramp lesions are in the red-red zone with excellent healing, the rehabilitation protocol for combined ACL + ramp repair is essentially the same as ACL alone. No significant restriction is needed for the ramp repair component.
Outcomes and Prognosis
| Outcome | Repaired | Unrepaired | Significance |
|---|---|---|---|
| Healing rate | Generally high | Variable | Favoured by red-red zone vascularity |
| Rotational stability | Restored | Increased laxity | Better biomechanics |
| ACL graft failure | Lower risk | Potentially higher | May protect graft |
| Return to sport | Similar to ACL alone | May have instability | Repair recommended |
The combination of peripheral red-red zone location (good vascularity) and secure fixation gives generally high healing rates. Repair adds little time and morbidity to ACL reconstruction and biomechanically helps restore rotational stability (the pivot shift), though firm prospective evidence that it reduces graft re-rupture is still incomplete.
Evidence Base and Key Trials
The 'Hidden Lesion' - Prevalence with Systematic Exploration
- 302 consecutive ACL reconstructions with a 3-stage systematic posteromedial exploration
- Overall ramp lesion prevalence 40% of the cohort (50 of 125 medial meniscal tears)
- 16.8% were 'hidden lesions' seen only after debridement through a posteromedial portal
- Standard anterior arthroscopy alone misses a substantial proportion of ramp tears
Thaunat Classification of Ramp Lesions
- Defines ramp tears by tear pattern (partial vs full thickness) and meniscotibial ligament disruption
- Describes a single posteromedial portal suture-hook repair technique
- Provides a common language to grade lesion severity and guide repair
- Higher-grade / unstable lesions are those warranting fixation
Posterior Medial Meniscus as a Secondary Restraint (Biomechanics)
- Cadaveric study (10 knees) of sequential ACL, ramp and meniscotibial ligament sectioning
- Ramp lesion increased anterior tibial translation by 2.6mm over the isolated ACL-deficient state
- Meniscotibial ligament detachment increased internal and external rotatory laxity
- Posterior horn of medial meniscus acts as a secondary restraint to anterior translation
Repair Needed to Restore the Pivot Shift (Robotic Biomechanics)
- 12 matched cadaveric pairs tested in a 6-DOF robotic system
- Combined meniscocapsular + meniscotibial lesions increased translation, rotation and the pivot shift
- ACLR alone restored anterior translation but did NOT restore the pivot shift
- Pivot shift was eliminated only when ACLR was combined with ramp repair
Do Small Ramp Lesions Need Repair? (Defect-Size Biomechanics)
- 8 cadaveric knees, robotic 6-DOF testing of 1cm, 2cm and 3cm ramp lesions
- Only a 3cm lesion significantly increased anterior translation in the ACL-deficient knee
- After simulated ACL reconstruction, ramp lesions had NO significant kinematic effect
- Small, stable ramp lesions may be left untreated when the ACL is reconstructed
MRI Has Low Sensitivity for Ramp Lesions
- 81 ACL-injured knees with methodical 3-step arthroscopic exploration as reference
- MRI sensitivity for ramp lesions only 27 to 46%; specificity 84 to 96%
- Sensitivity was lowest (0 to 20%) for true meniscocapsular-junction lesions
- Inter-observer reliability of MRI was only fair to moderate
Ramp Lesions in Children and Adolescents
- Systematic review, 387 paediatric/adolescent ACL injuries, 90 ramp lesions (23.3%)
- Prevalence in children similar to adult populations
- Pooled MRI sensitivity 50%, specificity 75%, accuracy 70%
- Posteromedial tibial bone bruise or thin fluid at the meniscocapsular junction should raise suspicion
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old male footballer presents for ACL reconstruction 3 months after injury. MRI shows complete ACL tear. There is a subtle increased signal at the posterior medial meniscus-capsule junction. How would you approach this case?”
“During ACL reconstruction on a 25-year-old female athlete, you probe the posteromedial compartment and find a 6mm gap between the posterior horn of the medial meniscus and the capsule with easy separation on probing. Walk me through your management.”
“A 28-year-old male presents 18 months after ACL reconstruction with persistent rotational instability. He has positive pivot shift. MRI shows intact ACL graft but a posterior medial meniscocapsular separation. How do you assess and manage this?”
MCQ Practice Points
Q: What is the prevalence of ramp lesions in patients with ACL tears? A: Approximately 24-40% - With systematic posteromedial arthroscopic exploration, prevalence reaches about 40% (Sonnery-Cottet 2014). Prevalence tends to be higher in chronic injuries and is similar in adolescents and adults.
Q: How reliable is MRI for detecting ramp lesions? A: Poor - sensitivity only ~27-50% - MRI frequently misses ramp lesions, especially true meniscocapsular-junction tears. This is why systematic arthroscopic exploration of the posteromedial compartment is mandatory during ACL reconstruction.
Q: In the Thaunat classification, which type represents a complete double lesion? A: Type 4 - Type 4 is a double lesion with complete separation of both superior and inferior surfaces. Type 1 is meniscocapsular only, Types 2-3 are partial, and Type 5 extends into the meniscal body.
Q: What gap size at the meniscocapsular junction indicates need for repair? A: Greater than 4mm - A gap of greater than 4mm on arthroscopic probing, or any lesion that is unstable on probing, indicates the need for repair regardless of classification type.
Q: In which meniscal zone are ramp lesions located, and what is the healing implication? A: Red-red zone - Ramp lesions are located at the peripheral meniscocapsular junction in the red-red zone, which has good blood supply. This vascularity supports the generally high healing rates seen with repair.
Q: What is the gold standard repair technique for ramp lesions? A: All-inside repair through posteromedial portal - All-inside repair using a posteromedial working portal is the gold standard. It avoids a posterior incision, reduces saphenous nerve risk, and provides secure fixation.
Guidelines, Registries & Global Practice
Ramp lesions complicate roughly 24-40% of ACL tears worldwide (up to 40% when a systematic posteromedial exploration is performed). Prevalence is comparable across adult and adolescent populations and tends to rise with chronicity and high-grade pivot shift. There is no formal national-society registry dedicated to ramp lesions; evidence is drawn from cadaveric, cohort and systematic-review data across centres in Europe, North America and Asia.
| Body / Source | Detection | Treatment stance |
|---|---|---|
| ESSKA / European meniscus consensus | Recommend posteromedial / trans-notch arthroscopic assessment in ACLR | Repair unstable lesions; stability-based decision-making |
| ISAKOS / sports-medicine expert opinion | High index of suspicion; MRI alone insufficient | Repair displaced/unstable tears at time of ACLR |
| AAOS (US) ACL guidance | No ramp-specific recommendation; broad ACL guidance only | Defers to surgeon judgement / lesion stability |
| AO / general arthroscopy teaching | Emphasise routine posteromedial inspection | Repair when displaceable; preserve meniscal tissue |
- Routine trans-notch viewing and dedicated posteromedial portal
- All-inside devices and suture-hook repair readily available
- 3T MRI and intra-operative image capture standard
- Strong sports-medicine fellowship exposure to the technique
- Reliance on lower-field MRI (or none) increases dependence on arthroscopic skill
- All-inside implants may be costly or unavailable - inside-out / suture-hook alternatives used
- Awareness and training are the main determinants of detection
- Emphasis on simple, low-cost suture repair to preserve the meniscus
- Record that the posteromedial compartment was systematically inspected (trans-notch and/or posteromedial portal)
- Record presence or absence of a ramp lesion
- If present: document tear pattern, stability on probing, and treatment
- Capture arthroscopic images of the lesion and repair where possible
- If not repaired, document the rationale (small, stable, patient factors)
- Counsel the patient about the possibility of an undetected lesion and the small chance of further surgery if symptomatic
Differential Diagnosis
| Condition | Distinguishing features | Key investigation / finding |
|---|---|---|
| Ramp lesion | Peripheral posterior horn MM tear at meniscocapsular junction; often asymptomatic in isolation | Trans-notch / posteromedial arthroscopy; MRI often normal |
| Posterior root tear of medial meniscus | Loss of hoop tension, meniscal extrusion, may have insidious onset | Coronal MRI 'ghost sign', radial extrusion on MRI |
| Bucket-handle medial meniscus tear | Mechanical locking, true block to extension | Displaced fragment / 'double PCL' sign on MRI |
| Meniscotibial (coronary) ligament injury | Posteromedial laxity, overlaps with ramp spectrum | Arthroscopic probing of meniscotibial attachment |
| Posteromedial corner / sMCL injury | Valgus and rotatory laxity, medial tenderness | Valgus stress test, MRI of POL/sMCL |
| Posterior horn degenerative / horizontal tear | Older patient, no acute pivot injury | MRI signal not reaching surface, no capsular separation |
Controversies and Areas of Uncertainty
Whether every visualised ramp lesion should be repaired is debated. Robotic data (Deichsel 2024) show small ramp lesions have little kinematic effect once the ACL is reconstructed, supporting selective, stability-based repair rather than reflex fixation of every lesion.
The classic 'gap greater than 4mm on probing' threshold is a pragmatic guide, not a validated cut-off. Probing technique, lesion length and meniscotibial-ligament integrity all influence the decision, and definitions vary between surgeons.
All-inside, inside-out and single-portal suture-hook techniques all have advocates. High-quality comparative outcome data are limited, so choice is driven by training, access and lesion morphology rather than proven superiority.
Biomechanically, repair best restores the pivot shift (DePhillipo 2018), and missed lesions are implicated in residual rotatory laxity. However, robust prospective clinical evidence that ramp repair reduces ACL graft re-rupture remains incomplete.
Definition
- Ramp = posterior meniscocapsular separation
- Location: posterior horn medial meniscus at capsule junction
- Zone: Red-red (peripheral, excellent vascularity)
- Function: secondary stabilizer to anterior translation
Epidemiology
- About 24-40% prevalence with ACL tears (40% with systematic exploration)
- Higher prevalence with chronic ACL injury
- Similar prevalence in adolescents and adults (about 23%)
- MRI sensitivity only ~27-50% - arthroscopy is the diagnostic gold standard
Thaunat Classification
- Type 1 = Meniscocapsular separation (most common)
- Type 2 = Partial superior lesion
- Type 3 = Partial inferior lesion
- Type 4 = Double lesion (must repair)
- Type 5 = Body extension (repair both)
Repair Indications
- Gap greater than 4mm on probing
- Instability on probing (any size)
- Type 4 or 5 lesions
- Young/high-demand patients
- When in doubt, repair (excellent healing)
Surgical Technique
- 70° scope for visualization
- Posteromedial working portal
- Rasp both surfaces
- All-inside repair (1-3 sutures)
- Confirm reduction after tensioning
Key Numbers
- Healing rate generally high (red-red zone)
- MRI sensitivity only ~27-50%
- Gap threshold ~4mm (a guide, not absolute)
- Repair typically adds under 15-30 min to ACL surgery (DePhillipo 2019 survey)
- Return to sport: follows ACL protocol (9-12 months)