Most Common Bone Malignancy
- BPLTK Primaries: Breast (female), Prostate (male), Lung (poor prognosis), Thyroid, Kidney.
- Mirels Score: 4 parameters (Site, Pain, Lesion, Size) - above 8 needs prophylactic fixation.
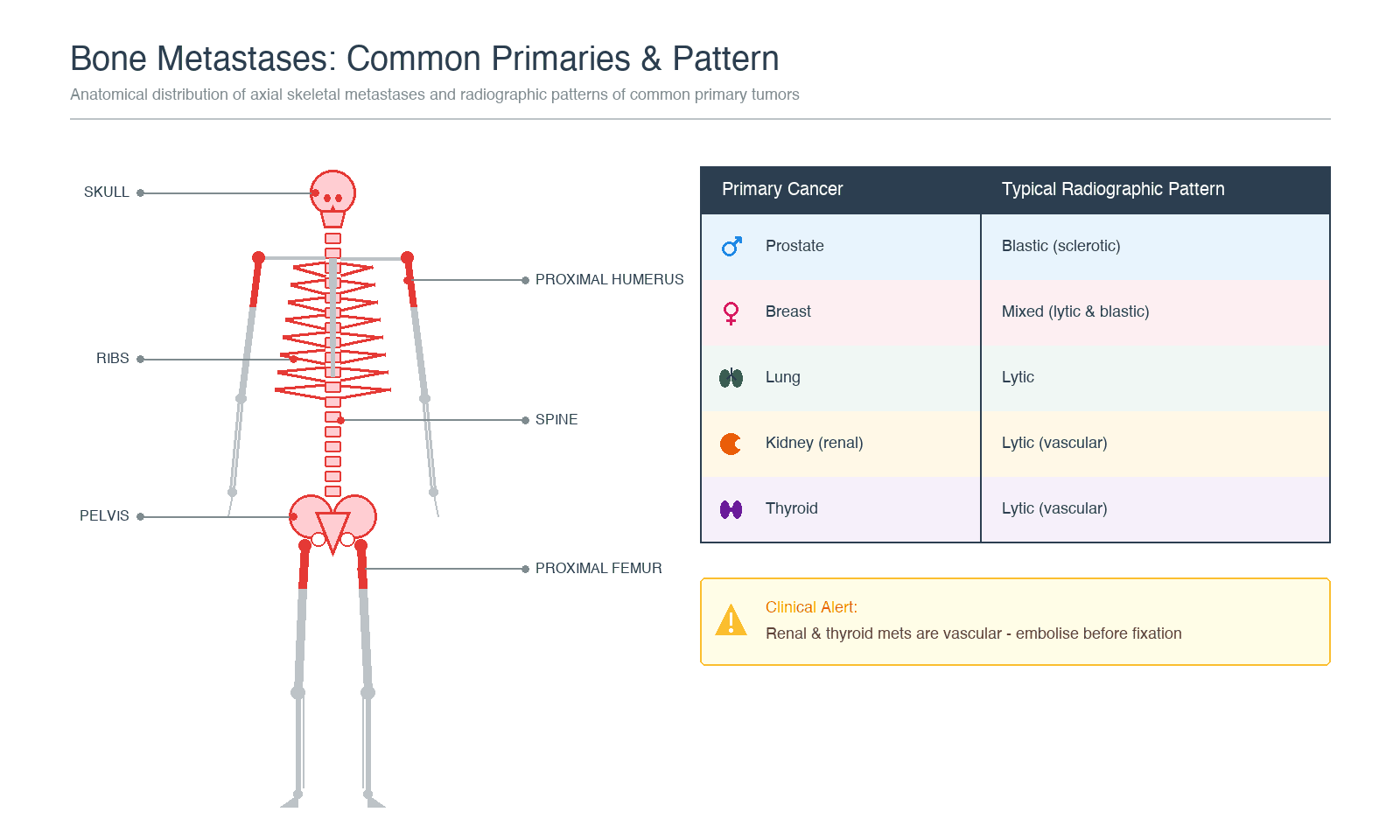
- Blastic Metastases: Prostate (most), breast (treated), small cell lung.
- Lytic Metastases: Kidney, thyroid, lung - structurally weaker.
- Vascular Tumors: Kidney and thyroid - MUST embolize before surgery.
- “BPLTK for common primaries
- “Mirels above 8 = prophylactic fixation
- “Kidney and thyroid are VASCULAR - embolize
- “Blastic = prostate; Lytic = kidney
- “Surgical goal is PALLIATION, not cure
Mirels Score predicts pathological fracture risk (Mirels, Clin Orthop Relat Res 1989).
- 4 Parameters: Site (upper/lower/peritrochanteric), Pain (mild/moderate/functional), Lesion (blastic/mixed/lytic), Size (under 1/3, 1/3-2/3, over 2/3 cortex).
- Score 1-3 for each (total range 4-12).
- Score 7 or lower: low risk → may irradiate safely without fixation.
- Score 8: grey zone (the original threshold for fixation); roughly 15% fracture risk - weigh patient factors.
- Score 9 or higher: greater than 33% fracture risk → PROPHYLACTIC FIXATION indicated.
- The original 1989 paper recommended fixation at a score of 8 or higher; in modern practice many fix at 9 or higher because the score over-predicts fracture (specificity only 35%, Damron 2003).
- Peritrochanteric location and lytic lesions score highest risk.
- Score 1
- Upper limb
- Score 2
- Lower limb
- Score 3
- Peritrochanteric
- Score 1
- Mild (not affected by activity)
- Score 2
- Moderate (some relief with rest)
- Score 3
- Functional (pain with weight-bearing)
- Score 1
- Blastic (sclerotic)
- Score 2
- Mixed
- Score 3
- Lytic (destructive)
- Score 1
- Under 1/3 diameter
- Score 2
- 1/3 to 2/3 diameter
- Score 3
- Over 2/3 diameter
Overview and Epidemiology
Metastatic bone disease is the most common malignancy affecting bone, far exceeding primary bone tumors in frequency.
Epidemiology
- Incidence: 25-30x more common than primary bone tumors
- Prevalence: Found at autopsy in 70-85% of patients with breast/prostate cancer
- Age: Typically middle-aged to elderly (reflecting primary cancer demographics)
- Impact: 350,000-400,000 people living with bone metastases in USA
Common Primary Tumors (BPLTK)
- Breast: Most common source overall and in women
- Prostate: Most common source in men
- Lung: Third most common; poor prognosis
- Thyroid: Differentiated carcinoma has better prognosis
- Kidney: Renal cell carcinoma; very vascular
Less Common Primaries
- Gastrointestinal (colon, stomach)
- Bladder
- Melanoma
- Unknown primary (10-15% of cases)
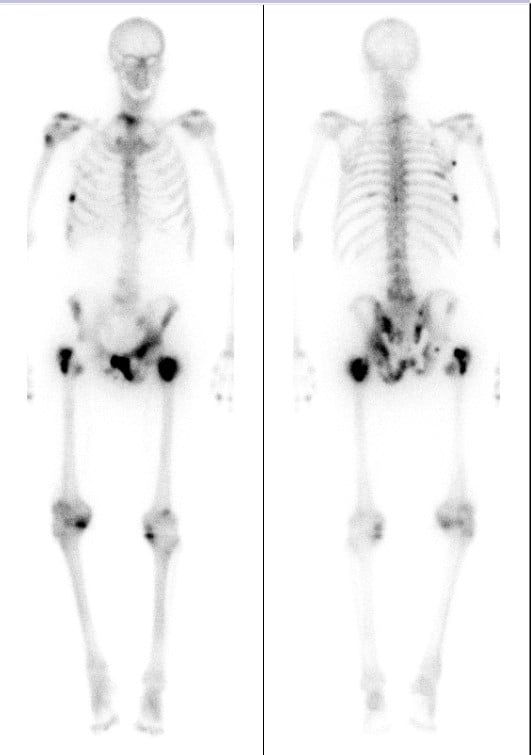
Distribution (Red Marrow Distribution)
- Spine: 70% - most common site (thoracic greater than lumbar greater than cervical)
- Pelvis: 40%
- Proximal Femur: 25%
- Ribs: 25%
- Skull: 15%
- Proximal Humerus: 15%
Pathophysiology
Mechanisms of Bone Metastasis
Metastatic Cascade:
- Primary Tumor Growth: Cancer cells proliferate in organ of origin
- Local Invasion: Tumor penetrates basement membrane
- Intravasation: Entry into bloodstream or lymphatics
- Circulation: Survival in circulation (most cells die)
- Extravasation: Exit from vessels at distant site
- Colonization: Establish growth in bone microenvironment
Why Bone?
- Hematogenous Spread: Most common route to bone
- Batson's Venous Plexus: Valveless vertebral venous system allows retrograde flow
- Explains predilection for spine and axial skeleton
- Low-pressure system facilitates tumor cell lodging
- Red Marrow Distribution: Sites with active hematopoiesis
- Rich blood supply
- Growth factors present
- Supportive microenvironment
The Vicious Cycle
Seed and Soil Hypothesis (Paget 1889): Cancer cells (seed) preferentially grow in bone microenvironment (soil)
The Cycle:
- Tumor cells arrive in bone marrow
- Tumor cells secrete factors (PTHrP, IL-6, TNF) → stimulate osteoclasts
- Osteoclasts resorb bone → release growth factors (TGF-β, IGF, BMPs)
- Growth factors stimulate tumor → more factor secretion
- Cycle perpetuates → progressive bone destruction
Lytic vs Blastic Metastases
Lytic Lesions (Bone Destruction):
- Kidney, thyroid, lung
- Osteoclast activation dominant
- Structurally weak bone
- High fracture risk
- Mechanisms: PTHrP, IL-1, IL-6, TNF-α
Blastic Lesions (Bone Formation):
- Prostate (most), treated breast, small cell lung
- Osteoblast activation dominant
- Dense but disorganized bone (structurally weak)
- Lower fracture risk
- Mechanisms: Endothelin-1, BMPs, Wnt signaling
Mixed Lesions:
- Breast (untreated), GI cancers
- Both processes active
Role of RANK/RANKL Pathway
- RANK: Receptor on osteoclast precursors
- RANKL: Ligand secreted by osteoblasts and tumor cells
- RANKL binding to RANK: Osteoclast activation and differentiation
- OPG (osteoprotegerin): Decoy receptor, inhibits RANKL
- Therapeutic target: Denosumab (RANKL inhibitor)
Clinical Features
History
- Known Cancer: 85% have known primary at presentation
- Unknown Primary: 15% bone metastasis is first presentation of cancer
- Pain: Most common symptom
- Night pain (classic)
- Activity-related (mechanical instability)
- Rest pain (tumor growth)
- Pathological Fracture: May be presenting feature
- Neurological: Spinal cord compression (weakness, sensory changes, bladder/bowel)
- Constitutional: Weight loss, fatigue, anorexia
Physical Examination
Examination Approach
-
Local Assessment
- Point tenderness over lesion
- Palpable mass (large lesions)
- Surrounding soft tissue swelling
-
Fracture Assessment
- Deformity, shortening
- Inability to weight-bear
- Crepitus (do not elicit if suspected)
-
Neurological Assessment (Spine)
- Motor: Power in myotomes
- Sensory: Dermatomal distribution
- Reflexes: Hyperreflexia (UMN) or hyporeflexia
- Bladder/bowel function
- Rectal tone, perianal sensation
-
Systemic Assessment
- Breast examination
- Prostate examination (DRE)
- Thyroid palpation
- Lymphadenopathy
- Abdominal masses
- General condition, performance status
Red Flags for Cord Compression
- New back pain in cancer patient
- Bilateral leg symptoms
- Bladder/bowel dysfunction
- Progressive weakness
- Sensory level
Metastatic spinal cord compression is an EMERGENCY. Early recognition critical as neurological recovery correlates with pre-treatment function. MRI whole spine urgently. High-dose dexamethasone, urgent oncology/spinal referral for decompression/radiation.
Investigations
Imaging
- First-line investigation
- Lytic (dark, destructive) vs Blastic (white, sclerotic) vs Mixed
- Need 30-50% cortical destruction to be visible
- Assess fracture risk, deformity
- Better cortical assessment than X-ray
- Quantify bone destruction
- CT chest/abdomen/pelvis for staging
- CT-guided biopsy planning
- Most sensitive for marrow involvement
- Essential for spinal metastases
- Assesses soft tissue extension
- Whole spine MRI if cord compression suspected
- Whole-body screening
- Highly sensitive but low specificity
- May miss pure lytic lesions (kidney, myeloma)
- Superscan = widespread metastases
- Increasingly used for staging
- Assesses metabolic activity
- Helps identify unknown primary
- Monitors treatment response
Laboratory Investigations
- Full Blood Count: Anaemia, pancytopenia (marrow infiltration)
- Biochemistry: Calcium (hypercalcemia), ALP (elevated), LDH
- Tumor Markers: PSA (prostate), CEA (GI, breast), AFP (germ cell), thyroglobulin
- Serum/Urine Protein Electrophoresis: Exclude myeloma
- Iron Studies: Chronic disease pattern
Biopsy
- Unknown primary tumor
- Solitary lesion (could be primary bone tumor)
- Atypical presentation
- Clinical doubt about diagnosis
- Image-guided core needle biopsy (preferred)
- Align biopsy tract with potential surgical approach
- Tissue for histology, immunohistochemistry, molecular studies
A solitary bone lesion in a patient with known cancer is NOT always metastatic. 10% of solitary lesions in cancer patients are primary bone tumors or benign. Biopsy if any doubt.
Differential Diagnosis of a Destructive Bone Lesion
- Clues that favour it
- Age over 40, known primary, multiple lesions, axial distribution
- Action point
- Confirms staging plus Mirels-based fixation decision
- Clues that favour it
- Pure punched-out lytic lesions, cold on bone scan, anaemia, raised ESR, paraprotein
- Action point
- Serum/urine electrophoresis, marrow biopsy - non-surgical primary treatment
- Clues that favour it
- Permeative lesion, large soft-tissue mass, relatively well patient
- Action point
- Biopsy - chemo/radiotherapy responsive, usually not resected
- Clues that favour it
- Solitary, aggressive periosteal reaction, soft-tissue mass, no known primary
- Action point
- DO NOT fix - refer to tumour unit for staging and planned biopsy
- Clues that favour it
- Fever, raised inflammatory markers, sinus, marrow oedema, may mimic tumour
- Action point
- Cultures plus biopsy before any implant
- Clues that favour it
- Raised calcium and PTH, subperiosteal resorption, generalised osteopenia
- Action point
- Treat hyperparathyroidism - lesion regresses
- Clues that favour it
- Younger patient, typical benign radiographic pattern, incidental
- Action point
- Observe or address per benign-lesion pathway
An aggressive solitary destructive lesion with no known primary must be staged and biopsied at the unit that will perform definitive surgery. Intramedullary nailing of an unsuspected primary sarcoma contaminates the entire bone, converts a limb-salvageable tumour into an amputation, and worsens survival.
Management
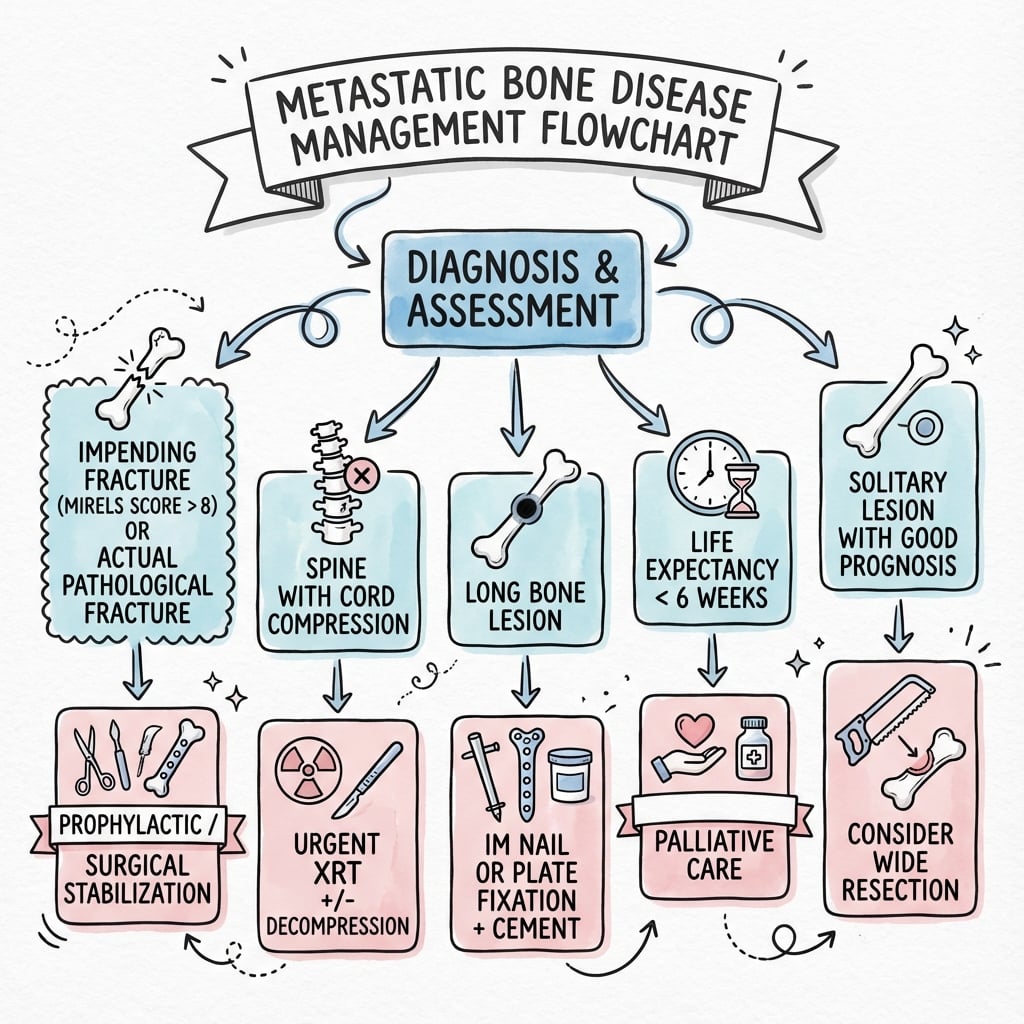
Management Principles
- Palliation - NOT cure
- Pain relief
- Restore/maintain function
- Prevent pathological fracture
- Improve quality of life
- Durable solution (patient may outlive implant)
- Medical oncology
- Radiation oncology
- Orthopaedic surgery
- Palliative care
- Pain management
- Physiotherapy
- Primary tumor type and responsiveness
- Expected survival
- Performance status
- Extent of metastatic disease
- Fracture risk (Mirels score)
- Patient wishes
Complications
Skeletal-Related Events (SREs)
Definition: Major complications from bone metastases requiring intervention
Types of SREs:
- Pathological Fracture: Most common SRE
- Spinal Cord Compression: Neurological emergency
- Bone Pain Requiring Radiation: Severe uncontrolled pain
- Hypercalcemia of Malignancy: Metabolic emergency
- Surgery to Bone: Stabilization or reconstruction
Pathological Fracture
Incidence: 10-30% of patients with bone metastases
- Lytic lesions (higher risk than blastic)
- Large lesion size (greater than 2/3 cortex)
- Peritrochanteric location
- Weight-bearing bones
- Mirels score above 8
- Urgent surgical stabilization
- Durable construct allowing immediate weight-bearing
- Post-operative radiation
- Worse outcomes than prophylactic fixation
Spinal Cord Compression
Oncological Emergency - Time-sensitive intervention
Incidence: 5-10% of cancer patients
- Back pain (95% - often first symptom)
- Motor weakness (75%)
- Sensory changes (50%)
- Bladder/bowel dysfunction (50%)
- Ambulatory status predicts outcome
- High-dose dexamethasone (10mg IV, then 16mg daily)
- Urgent MRI whole spine
- Neurosurgical/spinal consult
- Decompression + stabilization vs radiation
- HOURS matter - neurological recovery correlates with pre-treatment function
- Pre-treatment ambulatory status (most important)
- Time to develop motor deficit
- Extent of cord compression
- Primary tumor type
Hypercalcemia of Malignancy
Metabolic Emergency
- Osteoclastic bone resorption (lytic metastases)
- PTHrP secretion by tumor (humoral)
- Vitamin D production (lymphoma)
- Confusion, lethargy
- Nausea, vomiting, constipation
- Polyuria, polydipsia
- Dehydration
- Cardiac arrhythmias
- IV hydration (4-6L normal saline)
- Bisphosphonates (zoledronic acid)
- Calcitonin (rapid but short-lived effect)
- Denosumab if bisphosphonates fail
- Treat underlying cancer
Bone Pain
- Occurs in 75% of patients with bone metastases
- Severe impact on quality of life
- Limits mobility and function
- Periosteal stretching
- Microfractures
- Tumor growth
- Inflammatory mediators
- Nerve compression
- WHO pain ladder (simple analgesics → opioids)
- Radiation therapy (80% response rate)
- Bisphosphonates/denosumab
- Interventional pain management
- Neurolytic procedures for refractory pain
Surgical Complications
- Massive hemorrhage (especially kidney/thyroid)
- Cement extravasation
- Neurovascular injury
- Fat embolism
- Wound complications (15-20%)
- Infection (5-10% - higher than non-cancer surgery)
- Implant failure
- Local tumor progression
- DVT/PE (high risk population)
- Preoperative embolization (vascular tumors)
- Meticulous surgical technique
- Adequate bone cement use
- Post-operative radiation
- DVT prophylaxis
- Multidisciplinary approach
Long-term Complications
- Impaired fracture healing
- Radiation-induced fractures (rare)
- Soft tissue fibrosis
- Osteonecrosis of jaw (ONJ): 1-2% risk
- Atypical femur fractures (rare)
- Renal impairment (bisphosphonates)
- Local recurrence despite treatment
- New skeletal lesions
- Visceral metastases
- Declining performance status
Guidelines, Registries & Global Practice
Bone is the third most common site of metastasis after lung and liver. Breast, prostate, lung, thyroid and kidney account for the great majority of skeletal metastases, and bone metastases drive a heavy burden of skeletal-related events (SREs) regardless of health system.
Global Epidemiology
- Figure
- approx. 3.6% develop bone metastases; of those approx. 46% develop an SRE
- Source
- Jensen, BMC Cancer 2011 (Danish population cohort)
- Figure
- approx. 14% have at least one SRE on contemporary therapy
- Source
- Kwon, Urol Oncol 2022 (SEER-Medicare)
- Figure
- axial skeleton (spine, pelvis, proximal femur, ribs) following red marrow
- Source
- Multiple
- Figure
- pathological fracture; metastatic spinal cord compression in approx. 5-10% of cancer patients
- Source
- Multiple
Major Guidance, Side by Side
- Core recommendation
- Suspect MSCC and image whole-spine MRI within 24 h; early specialist referral; treat impending long-bone fracture before it breaks
- Evidence basis
- Patchell RCT + consensus
- Core recommendation
- A solitary destructive lesion in a patient with no known primary must be biopsied/staged before fixation - avoid "fix and forget"
- Evidence basis
- Expert consensus
- Core recommendation
- Mirels-based fracture-risk assessment; durable load-bearing construct allowing immediate weight-bearing; post-operative radiotherapy to whole operated bone
- Evidence basis
- Mirels, Damron
- Core recommendation
- Single 8 Gy fraction equals multi-fraction for pain in uncomplicated lesions
- Evidence basis
- Chow/Rich meta-analysis
- Core recommendation
- Bone-modifying agents (denosumab or zoledronic acid) for all patients with bone metastases from breast/prostate cancer and myeloma; monitor for ONJ and hypocalcaemia
- Evidence basis
- Stopeck RCT, Lipton pooled analysis
Registry and Practice Variation
- No dedicated international "bone-metastasis implant" registry exists; outcomes are drawn from oncology trial datasets and institutional series rather than arthroplasty-style joint registries.
- Practice variation: single-fraction radiotherapy uptake varies widely between countries despite equivalent efficacy, reflecting reimbursement and capacity rather than evidence. Preoperative embolization for renal/thyroid metastases is standard in tertiary centres but its measured benefit is greatest for large lesions and open reconstructions, and is less consistent for intramedullary nailing and non-renal primaries (Pazionis 2014, Robial 2012).
- Resource-limited settings: where interventional radiology, endoprostheses or radiotherapy are scarce, management shifts toward cemented internal fixation and single-fraction radiotherapy; late presentation with established fracture or cord compression is more common, worsening functional outcome.
Special Considerations
Unknown Primary
- 10-15% of bone metastases have no known primary
- Workup: CT CAP, PET, tumor markers, serum/urine electrophoresis
- Biopsy essential for diagnosis and treatment planning
- Immunohistochemistry directs investigation
Solitary Metastasis
- May represent oligometastatic disease
- Consider aggressive local treatment
- Wide resection + adjuvant therapy in selected cases
- Better prognosis than polymetastatic disease
Renal Cell Carcinoma (Special Case)
- Very vascular - MUST embolize
- May be radiosensitive (modern targeted therapy)
- Solitary metastasis: Consider nephrectomy + metastasectomy
- Targeted therapy (TKIs, immunotherapy) have improved outcomes
Pathological Fracture vs Impending Fracture
- Actual fracture: Fix urgently, control pain
- Impending fracture: Elective prophylactic fixation
- Better outcomes with prophylactic surgery than fracture fixation
MCQ Practice Points
Q: Which primary cancers most commonly metastasize to bone? A: Breast, prostate, lung, thyroid, and kidney (mnemonic: "BLT with a Kosher Pickle"). These five primaries account for over 80% of skeletal metastases. Breast and prostate are the most common sources overall.
Q: What Mirels score indicates prophylactic fixation is recommended? A: The original Mirels paper (1989) recommended prophylactic fixation for a score of 8 or higher (out of 12), reserving radiotherapy alone for scores of 7 or lower. A score of 8 carries roughly 15% fracture risk and 9 or higher greater than 33%; because the score over-predicts fracture (specificity only 35%, Damron 2003), many surgeons fix at 9 or higher and treat 8 as a grey zone weighed against patient factors.
Q: Which primary tumors typically produce osteoblastic (sclerotic) metastases? A: Prostate and breast cancer. Prostate is classically blastic (98% blastic), while breast can be lytic, blastic, or mixed. Lung, thyroid, and renal metastases are typically lytic. Multiple myeloma is also purely lytic.
Q: What is the mechanism of action of denosumab in treating bone metastases? A: RANKL inhibitor (monoclonal antibody). By blocking RANKL, denosumab prevents osteoclast activation and bone resorption. Unlike bisphosphonates, it is not renally excreted so is safer in renal impairment.
Self-Assessment Quiz
At a Glance
Metastatic bone disease is the most common malignancy affecting bone, far exceeding primary bone tumors. The BPLTK primaries (Breast, Prostate, Lung, Thyroid, Kidney) account for most cases, with metastases preferentially affecting the axial skeleton following red marrow distribution. The Mirels scoring system predicts pathological fracture risk using 4 parameters (Site, Pain, Lesion type, Size)—scores greater than 8 indicate prophylactic fixation due to greater than 33% fracture risk. Blastic lesions suggest prostate (most common), while lytic lesions (kidney, thyroid, lung) are structurally weaker. Kidney and thyroid metastases are highly vascular and require preoperative embolization. Management is palliative with durable constructs allowing immediate weight-bearing.
BPLTKCommon Primaries - BPLTK
Hook:BPLTK (Bad Places Leak To Kidneys) - the 5 common primaries that metastasize to bone.
SPLSMirels Score - SPLS
Hook:SPLS - Site, Pain, Lesion, Size. Above 8 = Fix, above 9 = Definitely fix.
PBSBlastic vs Lytic - PBS
Hook:PBS (Prostate, Breast, Small cell) make bone STRONGER (blastic). Everything else is LYTIC and weak.
TKVascular Metastases - TK
Hook:TK (Total Knockout) - Thyroid and Kidney will knock you out with blood loss. Embolize 24-48h before surgery.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with breast cancer presents with painful right thigh. X-ray shows a large lytic lesion in the proximal femur involving 60% of the cortex. She has functional pain on weight-bearing. Mirels score is 9.”
“A 72-year-old man with known renal cell carcinoma has a painful proximal humerus lesion. X-ray shows a large lytic lesion. You're planning surgery. What additional steps are needed?”
“A 65-year-old man presents with back pain and pathological fracture of L3. No cancer history. X-ray shows lytic destruction. How would you investigate and manage?”
COMMON PRIMARIES - BPLTK
- Breast - most common female, responsive, years survival
- Prostate - most common male, BLASTIC, indolent
- Lung - poor prognosis, months survival
- Thyroid - VASCULAR, embolize, good if differentiated
- Kidney - VASCULAR, embolize, targeted therapy
MIRELS SCORE
- Site: Upper (1), Lower (2), Peritroch (3)
- Pain: Mild (1), Moderate (2), Functional (3)
- Lesion: Blastic (1), Mixed (2), Lytic (3)
- Size: Under 1/3 (1), 1/3-2/3 (2), Over 2/3 (3)
- SCORE ABOVE 8 = PROPHYLACTIC FIXATION
BLASTIC vs LYTIC
- BLASTIC: Prostate (most), breast (treated), small cell
- Blastic = dense but disorganized bone (still weak)
- LYTIC: Kidney, thyroid, lung, most others
- Lytic = structurally weaker = higher fracture risk
VASCULAR - EMBOLIZE
- Kidney and Thyroid = VASCULAR
- MUST embolize 24-48 hours before surgery
- Reduces blood loss 50-80%
- Cell saver contraindicated in malignancy
SURGICAL PRINCIPLES
- Goal = PALLIATION (not cure)
- Immediate weight-bearing
- Durable construct
- Protect entire bone (long nail)
- Post-op radiation for local control
PROXIMAL FEMUR OPTIONS
- Head/neck spared: Cephalomedullary nail (long)
- Head/neck involved: Endoprosthetic replacement
- Long-stem cemented prosthesis
- Cement augmentation for defects
MEDICAL MANAGEMENT
- Bisphosphonates or Denosumab reduce skeletal events
- Radiation for pain (80% response)
- Systemic therapy based on primary
- MDT approach essential
Evidence Base
- Derived a weighted 4-parameter score (Site, Pain, Lesion, Size) from 78 irradiated long-bone metastases
- Mean score 7 in lesions that did not fracture; mean score 10 in lesions that fractured within 6 months
- Lesions scoring 7 or lower could be irradiated safely; lesions scoring 8 or higher warranted prophylactic fixation
- Risk of fracture rose progressively as the score increased above 7
- 53 observers across 5 experience levels scored 12 femoral metastatic lesions
- Overall sensitivity 91%, specificity 35% for predicting fracture
- Mirels score outperformed unstructured clinical judgement at every experience level
- Reproducible and valid but over-predicts fracture (low specificity)
- Mirels score negative predictive value 86-100% (excellent at excluding impending fracture)
- Positive predictive value only 23-70%, confirming over-treatment
- CT-based finite-element / engineering methods correlate strongly with ex-vivo strength (r 0.68-0.96)
- No clinically validated quantitative method has yet replaced Mirels
- 101 patients randomised to surgery plus radiotherapy versus radiotherapy alone
- Ambulation after treatment: 84% (surgery) versus 57% (radiotherapy alone), odds ratio 6.2
- Patients retained the ability to walk far longer (median 122 vs 13 days)
- More non-ambulant patients regained walking with surgery (62% vs 19%); less steroid and opioid use
- 27 renal cell and 12 thyroid carcinoma cases matched to 41 non-embolised controls
- Embolisation reduced mean estimated blood loss (0.90 vs 1.77 L) and transfusion (2.15 vs 3.56 units)
- Operative time shorter with embolisation (3.13 vs 3.91 hours)
- Benefit greatest for large tumours and open femoral procedures; renal function preserved
- 2,046 patients with breast cancer and bone metastases randomised to denosumab or zoledronic acid
- Denosumab superior in delaying time to first skeletal-related event (hazard ratio 0.82, P = .01)
- Reduced first and subsequent SREs (rate ratio 0.77)
- Osteonecrosis of the jaw similar (2.0% vs 1.4%); hypocalcaemia more frequent with denosumab
- 29 randomised trials of palliative radiotherapy for uncomplicated bone metastases
- Overall pain response 61% (single fraction) versus 62% (multiple fraction) - equivalent
- Complete response 23% vs 24%; no difference in pathological fracture or cord compression risk
- Re-treatment more common after single fraction (20% vs 8%)