Meyers-McKeever Classification of Tibial Spine Fractures
Types I and II can be treated non-operatively in a cylinder cast or hinged brace in extension (or near-extension) for 4 to 6 weeks. Types III and IV almost always require operative reduction and internal fixation — arthroscopic suture fixation or screw fixation is the modern standard. If a Type II fracture fails to reduce or maintain reduction on follow-up imaging, it escalates to operative management. Always check for entrapment of the anterior horn of the medial meniscus or the intermeniscal ligament — this blocks reduction and is the commonest reason a Type II or III fails closed management.
Anatomical and biomechanical rationale
- Why children avulse bone rather than tear the ACL. The incompletely ossified tibial eminence is the weakest point in the ligament-bone complex in the skeletally immature knee. The ACL itself has superior tensile strength to its chondroepiphyseal insertion, so the failure mode is bony avulsion rather than mid-substance rupture.
- Peak incidence is 8 to 14 years. The eminence ossifies progressively; before approximately 8 years the cartilaginous eminence rarely fractures in isolation, and after the mid-teens the ossified eminence is strong enough that the ligament itself tears (adult-pattern ACL injury).
- Mechanism of injury is classically a hyperextension or valgus–external rotation force — the same mechanism as an ACL tear. A fall from a bicycle, a sporting twisting injury, or a direct blow to the flexed knee are typical presentations.
- Associated injuries. Meniscal entrapment under the fragment is common in displaced fractures, but a true meniscal tear is uncommon (only ~4% in the Kocher series). Chondral damage and collateral ligament injury also occur. Always image and examine the entire knee, not just the spine.
The weak link is the bone, not the ligamentWhy bone avulses in children
Hook:Same mechanism as an adult ACL tear (hyperextension / valgus–external rotation) — only the failure site differs because of skeletal immaturity.
The Meyers-McKeever classification (with Zaricznyj Type IV)
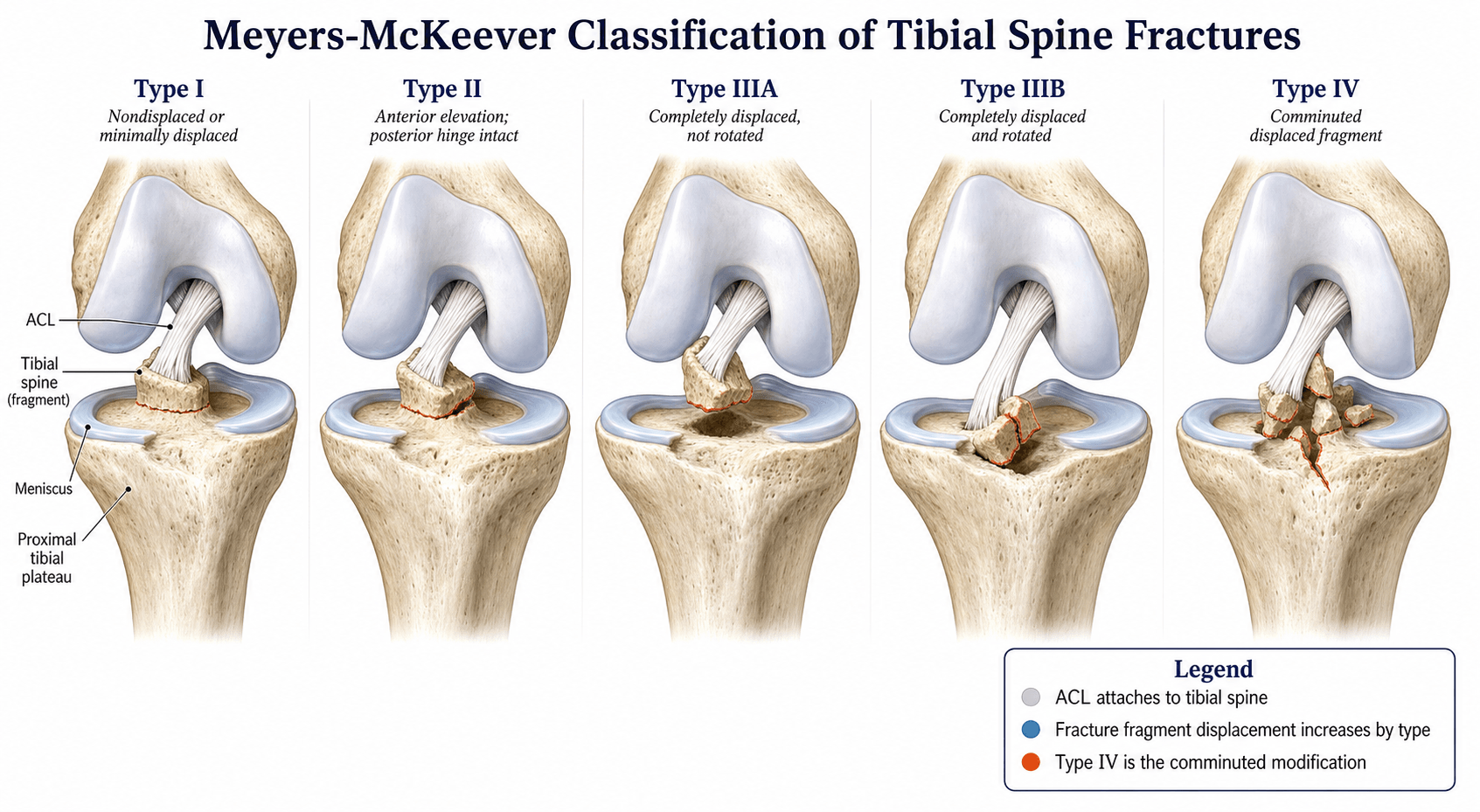

The tibial intercondylar eminence (spine) is an unossified or partially ossified ridge in the child. An acute valgus–external rotation or hyperextension force avulses the ACL from its tibial footprint. The classification is based on the degree of displacement of the fracture fragment.
- Description
- Undisplaced or minimally displaced
- Displacement
- Fragment in anatomic position
- Management
- Non-operative: cylinder cast or brace in extension for 4–6 weeks
- Description
- Hinged — posterior cortex intact
- Displacement
- Anterior third to half elevated; posterior hinge intact
- Management
- Trial of extension casting; if residual gap on lateral X-ray, consider operative fixation
- Description
- Fully displaced
- Displacement
- Complete separation from the tibial bed; may be rotated
- Management
- Arthroscopic (or open) reduction and fixation — suture or screw
- Description
- Comminuted (Zaricznyj addition)
- Displacement
- Multiple fragments
- Management
- Arthroscopic reduction and fixation; often suture-based as screw purchase is poor in comminuted bone
Undisplaced · Hinged · Displaced · ComminutedThe four types
Hook:Non-operative for I and II; operative for III and IV. The dividing line is whether the fragment will sit reduced — a Type II that won't stay down behaves like a Type III.
The anterior horn of the medial meniscus and the intermeniscal ligament can become interposed between the fragment and the tibial bed — this is the commonest cause of a failure to reduce a Type II or III fracture. If the lateral radiograph shows a persistent gap despite extension casting or intra-operative extension, suspect soft-tissue interposition and explore arthroscopically.
Clinical presentation and imaging
- Presentation. A child or adolescent with an acute traumatic haemarthrosis of the knee, pain, inability to weight-bear, and a positive Lachman test or anterior drawer. The haemarthrosis may be tense.
- Plain radiographs. Lateral view is the key film — it demonstrates the elevation of the fragment and the degree of displacement. The AP view may show the eminence fragment superimposed on the intercondylar notch. A tunnel (notch) view can also be helpful.
- CT is useful for surgical planning in Types III and IV to assess fragment size, comminution, and displacement direction. It is not mandatory for Types I and II.
- MRI identifies associated soft-tissue injuries (meniscal tears, chondral damage, partial ACL tears of the remnant) and confirms the integrity of the posterior cortex hinge in Type II. It is increasingly recommended for Types II–IV.

The lateral radiograph shows elevation of the tibial spine fragment from the tibial plateau. Measure the gap between the fragment and its bed — a gap of more than 2 mm is considered displaced (Type II or III).
An ossifying tibial eminence in a younger child can appear irregular on X-ray and mimic a fracture. Correlate with clinical examination (haemarthrosis, instability) and compare with the contralateral knee if in doubt.
A tibial spine avulsion is only one cause of a tense post-traumatic knee effusion in a child — the examiner will ask for the rest, because they change the management:
- Tibial spine (eminence) avulsion fracture — the classic skeletally-immature "ACL-equivalent".
- Intrasubstance ACL tear — increasingly recognised even in children (especially adolescents nearing maturity); the ligament can tear mid-substance rather than avulse bone, and importantly a partial ACL/interstitial plastic-deformation injury can COEXIST with the bony avulsion, which is part of why laxity can persist after an anatomically reduced fragment.
- Patellar dislocation (often self-reduced) — an MPFL/medial-retinacular tear, frequently with an osteochondral fragment off the patella or lateral femoral condyle.
- Osteochondral fracture, a peripheral meniscal tear, and a physeal or tibial-plateau fracture complete the list (PCL injury is less common).
The practical rule: a tense haemarthrosis in a child is a significant intra-articular injury until proven otherwise — examine for instability, scrutinise the lateral film, and use MRI to separate these diagnoses and to detect entrapment.
Management by type
- 1Classify on the lateral filmLateral radiograph defines displacement and the posterior hinge. Gap over 2 mm = displaced (II/III). CT for III/IV surgical planning; MRI for soft-tissue assessment in II–IV.
- 2Type I–II: trial of closed reductionExtend (or hyperextend) the knee to reduce the fragment; cylinder cast/hinged brace in extension. Repeat the lateral film in the cast — persistent gap means escalation.
- 3Type III–IV (or irreducible II): theatreArthroscopic reduction; FIRST release any entrapped anterior horn/intermeniscal ligament and clear the bed, then reduce anatomically.
- 4Fix + early motionSuture fixation through transosseous tunnels (physeal-sparing; preferred for comminuted IV) or screw for a large single fragment. Hinged brace, ROM from ~2 weeks to limit arthrofibrosis.
- Initial Management
- Cylinder cast or hinged brace in extension or near-extension for 4–6 weeks
- If Reduction Fails / Persistent Gap
- Not applicable (already reduced)
- Rehabilitation
- Range-of-motion at 4–6 weeks; progressive weight-bearing; physiotherapy for quadriceps and proprioception
- Initial Management
- Trial of extension casting or hyperextension manoeuvre; repeat lateral X-ray to confirm reduction
- If Reduction Fails / Persistent Gap
- If gap persists or fragment does not reduce: arthroscopic reduction and fixation
- Rehabilitation
- Same timeline as Type I if non-operative; post-operative protocol if fixed
- Initial Management
- Arthroscopic reduction and fixation (suture or screw); check for meniscal or intermeniscal ligament interposition
- If Reduction Fails / Persistent Gap
- If fragment is rotated or soft tissue is interposed: remove the block, reduce, and fix
- Rehabilitation
- Hinged brace; range-of-motion from 2 weeks; weight-bearing as tolerated in brace by 4–6 weeks
- Initial Management
- Arthroscopic reduction and suture fixation (screw fixation often unsuitable due to comminution)
- If Reduction Fails / Persistent Gap
- If fragments are too comminuted for fixation: debride small loose pieces and reattach the ACL remnant to the tibial bed with sutures through transosseous tunnels
- Rehabilitation
- Same as Type III post-operative protocol; may need slower progression if fixation tenuous
Never accept persistent displacement in Type III/IV fractures. Unreduced tibial spine fractures heal in a raised position, producing a bony block to full extension and residual ACL laxity. Late reconstruction is more complex and yields inferior results compared with early anatomical reduction.
Complications and outcomes
- Residual ACL laxity. Reported in a significant minority of patients even after anatomical reduction and fixation. Mechanisms include plastic deformation of the ACL before avulsion, interposed tissue healing in a lengthened position, and insufficient fixation. Patients and families should be counselled about this possibility up front.
- Loss of extension (arthrofibrosis). The most common complication after surgical fixation, particularly if immobilisation is prolonged or rehabilitation is delayed. Early range-of-motion in a hinged brace reduces the risk.
- Meniscal injury. The anterior horn of the medial meniscus or the intermeniscal ligament can be trapped beneath the fragment, blocking reduction. This must be identified and released at the time of surgery.
- Growth disturbance. Rare, because the fracture is through the chondroepiphyseal region rather than the physis itself. However, in very young children or with transphyseal fixation techniques, the risk must be considered. Avoid transphyseal hardware when possible in the skeletally immature.
- Non-union or malunion. Uncommon with operative management of displaced fractures; non-operative management of Type II with a persistent gap carries a higher risk of malunion in a displaced position.
LAME — Laxity · Arthrofibrosis · Meniscal entrapment · Extension lossThe four key complications
Hook:Counsel families about Laxity and Arthrofibrosis pre-operatively — both can occur even after a technically perfect reduction.
Loss of motion is the most frequent problem after tibial spine fixation, so know more than "it can happen":
- Risk factors — prolonged immobilisation, delayed surgery, rigid fixation, and younger patients; a malreduced or proud fragment is itself a mechanical block to full extension, so an accurate, flush reduction is part of preventing stiffness.
- Prevention — fixation secure enough to allow early range of motion in a hinged brace (immediate to about 2 weeks) is the single best protection; over-tensioning or leaving the fragment elevated defeats it.
- Recognition — a loss of terminal extension (and sometimes flexion) at follow-up; an extension block may be a proud/malreduced fragment or a fibrous "cyclops"-type nodule in the intercondylar notch.
- Managing established arthrofibrosis — start with intensive physiotherapy; if motion does not recover, proceed to examination under anaesthesia and gentle manipulation (protecting the physis and the fixation), and arthroscopic lysis of adhesions with notch debridement / cyclops-lesion excision and removal of any prominent hardware.
Guidelines, registries and global practice
- No single universal guideline. Management of paediatric tibial spine fractures is guided by the Meyers-McKeever classification and institutional protocols rather than a single society-level guideline. The AO Foundation and POSNA (Pediatric Orthopaedic Society of North America) teaching broadly follow the classification-based algorithm described above.
- Fixation technique varies by region. Arthroscopic suture fixation is increasingly the global standard, particularly for Types III and IV, because it avoids hardware-related complications and respects the physis. Screw fixation remains common in centres with established expertise, particularly for large single fragments (Type III). Open reduction is reserved for irreducible or complex comminuted fractures.
- Non-operative vs operative threshold. There is broad international consensus that Types I and II are managed non-operatively (with the caveat that a Type II that does not reduce or maintain reduction is elevated to operative management). Types III and IV are almost universally treated operatively. This consensus spans North American (POSNA), European (EPOS), and Australasian practice.
- Rehabilitation protocols. Centres vary in the timing of range-of-motion initiation (immediate vs 2 weeks post-operative) and weight-bearing progression (4 vs 6 weeks). Early motion is increasingly favoured to reduce arthrofibrosis risk.
Viva practice
- I undisplaced; II hinged (posterior cortex intact); III displaced/rotated; IV comminuted (Zaricznyj).
- Non-operative I–II; operative III–IV — a Type II that won't stay reduced becomes operative.
- Paediatric ACL-equivalent — bony avulsion because the unossified eminence is the weak link.
- Meniscal/intermeniscal-ligament entrapment (~26% type II, ~65% type III) is the commonest block to reduction — release it before reducing.
- Suture fixation is physeal-sparing and preferred for comminuted IV (biomechanically no clear advantage between methods — surgeon's judgment).
- Counsel about residual ACL laxity and arthrofibrosis even after anatomical reduction.
Exam viva
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy fell from his bicycle and landed on his right knee. The knee is swollen and tense. Lachman test demonstrates anterior laxity with a soft endpoint. The lateral radiograph shows the tibial spine fragment elevated approximately 5 mm from its bed with a posterior hinge intact. How would you classify and manage this injury?”
“You are asked to see a 10-year-old girl with a fully displaced, rotated tibial spine fracture (Meyers-McKeever Type III). At arthroscopy, the anterior horn of the medial meniscus is interposed between the fragment and the tibial bed and cannot be reduced. How would you proceed?”
Exam cheat sheet
The four types
- Type I: undisplaced — cast or brace in extension for 4 to 6 weeks
- Type II: hinged (posterior cortex intact), anterior third to half elevated — trial extension casting; fix if persistent gap
- Type III: fully displaced, may be rotated — arthroscopic reduction and fixation (suture or screw)
- Type IV: comminuted (Zaricznyj addition) — arthroscopic reduction and suture fixation
Key decision points
- Types I and II: non-operative (with the caveat that a Type II that does not reduce needs surgery)
- Types III and IV: operative — arthroscopic reduction and internal fixation
- Always check for meniscal or intermeniscal ligament interposition — the commonest cause of irreducible fracture
- Counsel families about residual ACL laxity even after anatomical reduction
Complications and pitfalls
- Residual ACL laxity: common even with good reduction (plastic deformation of the ACL before avulsion)
- Arthrofibrosis: most common post-operative complication; early range-of-motion reduces risk
- Meniscal entrapment: blocks reduction; must be identified and released at surgery
- Growth disturbance: rare but consider with transphyseal fixation in the skeletally immature
Evidence
Fracture of the intercondylar eminence of the tibia
- Original classification of tibial intercondylar eminence fractures into three types based on displacement
- Recommended non-operative treatment for undisplaced fractures and operative reduction for displaced fractures
- Established the clinical and radiographic criteria still used today
Avulsion fracture of the tibial eminence: treatment by open reduction and pinning
- Proposed the Type IV (comminuted) addition to the Meyers-McKeever classification
- Recognised that comminuted fragments require a different fixation strategy to the original three types
- Described outcomes with open reduction and pinning techniques
According to PubMed, the classification is from Meyers & McKeever 1959 (PMID 13630956) with the comminuted Type IV added by Zaricznyj 1977 (PMID 591548). The meniscal-entrapment prevalence (26% type 2, 65% type 3) is from Kocher et al. 2003 (DOI 10.1177/03635465030310031301), and the biomechanical fixation comparison (no significant difference between methods) from Mahar et al. 2008 (DOI 10.1097/BPO.0b013e318164ee43).