Technique, normal anatomy and pathological patterns for the orthopaedic exam
Seddon Classification
Neurapraxia: Conduction block, nerve intact
Axonotmesis: Axon disrupted, endoneurium intact
Neurotmesis: Complete nerve disruption
Key: MRI can show continuity but not differentiate axonotmesis from neurotmesis reliably
Critical Must-Knows
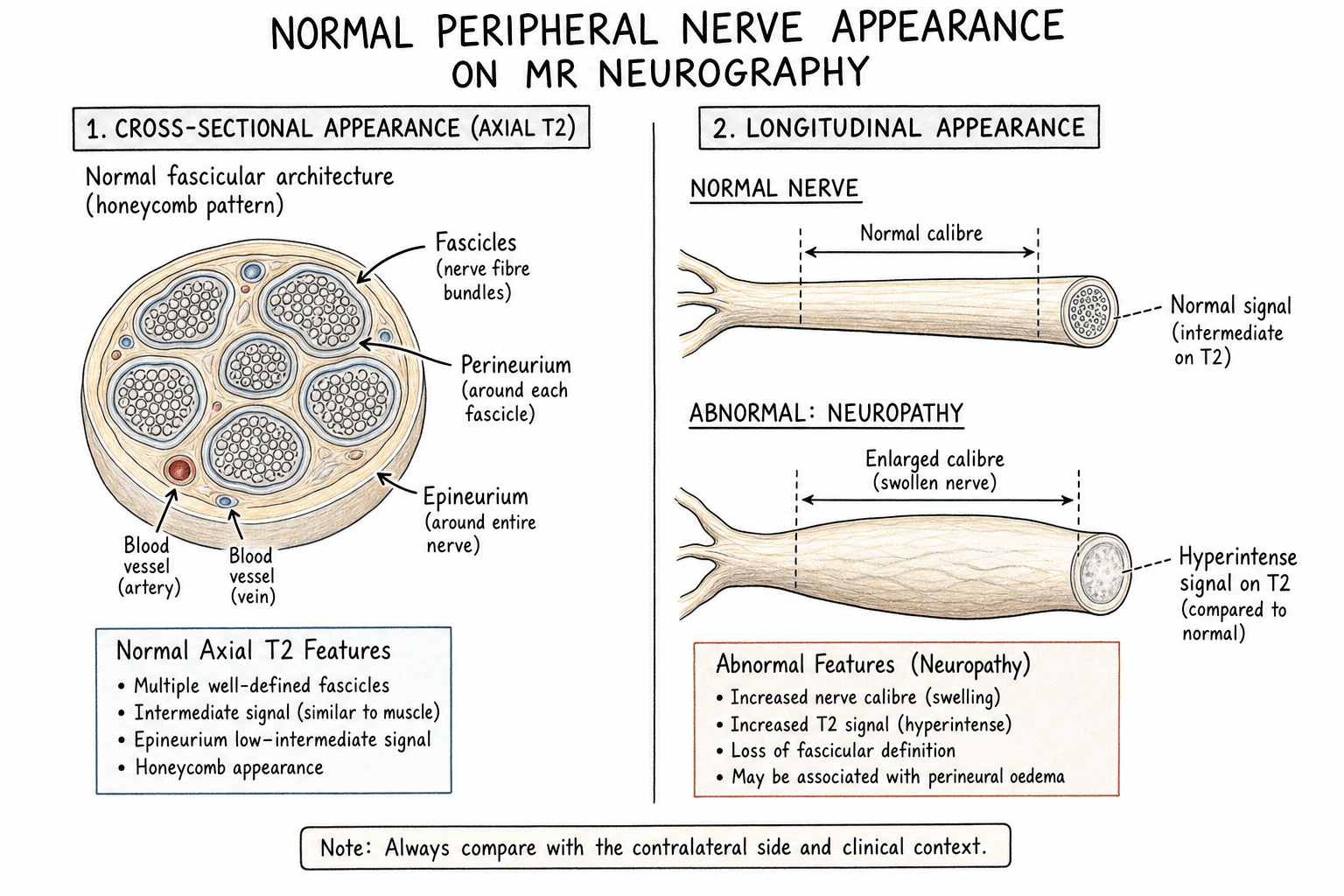
- Normal nerve: intermediate T1, slightly high T2, fascicular pattern
- Pathology: nerve enlargement, T2 hyperintensity, loss of fascicular pattern
- 3T MRI preferred for nerve imaging (higher SNR)
- PD or T2 fat-sat sequences best for nerve visualisation
- Denervation oedema in muscle indicates upstream nerve injury
Clinical Pearls
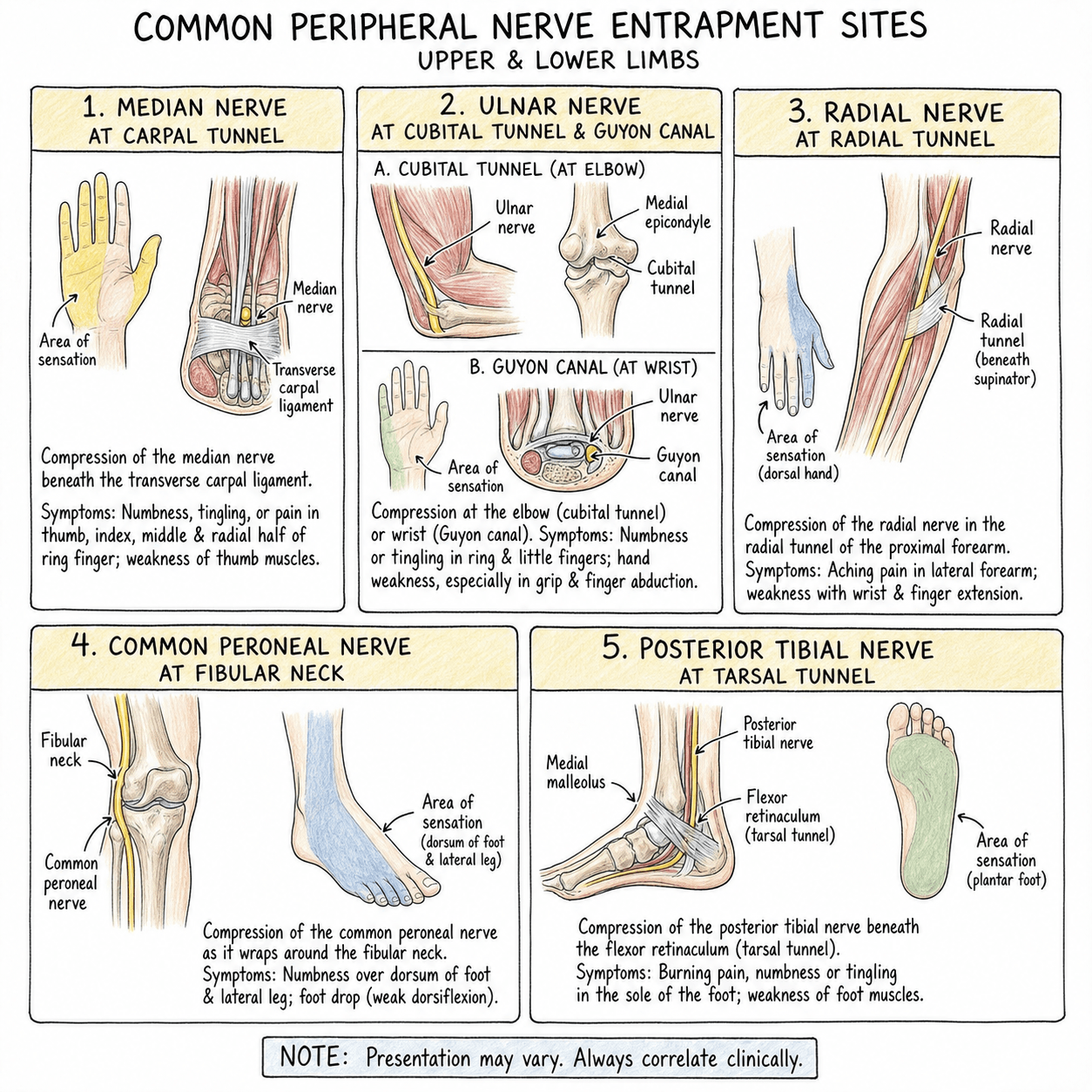
- "Carpal tunnel: median nerve greater than 10mm² at pisiform level
- "Cubital tunnel: ulnar nerve enlargement proximal to tunnel
- "Brachial plexus: roots, trunks, divisions, cords, branches
- "Nerve tumour: fusiform swelling, target or fascicular sign
- "Muscle denervation: T2 high acutely, fatty replacement chronically
Clinical Warning
MRI neurography is a specialised technique. Know the normal nerve signal characteristics, signs of compression (enlargement, T2 hyperintensity), and the muscle denervation pattern that indicates nerve pathology. Carpal tunnel and cubital tunnel are common clinical applications.
SCALE-TReading the Abnormal Nerve
| S | S = Size (cross-sectional area enlargement) | L | L = Localisation to a known fibro-osseous tunnel |
| C | C = Calibre change at an entrapment point | E | E = Enhancement (suggests tumour or active inflammation) |
| A | A = Architecture (loss of fascicular / honeycomb pattern) | T | T = T2 signal hyperintensity (oedema) plus muscle denervation |
| S | S = Size (cross-sectional area enlargement) | A | A = Architecture (loss of fascicular / honeycomb pattern) | E | E = Enhancement (suggests tumour or active inflammation) |
| C | C = Calibre change at an entrapment point | L | L = Localisation to a known fibro-osseous tunnel | T | T = T2 signal hyperintensity (oedema) plus muscle denervation |
Hook:Signal change alone is non-specific; combine size, calibre, architecture and muscle denervation before calling pathology.
Overview & Imaging Principles
What MR neurography adds
Where Nerve Imaging Fits
| Question | Best initial test | Role of MR neurography |
|---|---|---|
| Typical carpal/cubital tunnel | Clinical + nerve conduction studies | Reserved for atypical or secondary causes |
| Superficial focal neuropathy | High-resolution ultrasound | Problem-solving, deep extension |
| Plexus / proximal / deep nerve | MR neurography | First-line imaging |
| Suspected nerve tumour | MRI with contrast | Characterisation and surgical planning |
| Functional deficit, localising level | MRI muscle denervation map | Identifies level and chronicity |
Clinical Imaging Technique
Optimal MRI Neurography Protocol
| Parameter | Recommendation | Rationale |
|---|---|---|
| Field strength | 3T preferred over 1.5T | Higher SNR for small structures |
| Coil | Dedicated surface coil | Maximises signal-to-noise |
| Slice thickness | Less than 3mm | Resolves fascicular detail |
| In-plane resolution | Less than 1mm | Visualises nerve architecture |
| Sequences | PD fat-sat, T2 fat-sat, T1 | Nerve-fluid contrast |
| Planes | Axial perpendicular to nerve + along nerve | Cross-section and longitudinal |
Nerve Visualisation Principles
Systematic Approach: Normal Nerve Appearance
Normal Peripheral Nerve MRI Characteristics
| Feature | Appearance | Significance |
|---|---|---|
| T1 signal | Intermediate (isointense to muscle) | Anatomic localisation |
| T2/PD signal | Mildly hyperintense to muscle | Not as bright as fluid |
| Fascicular pattern | Honeycomb appearance on axial | Intact nerve architecture |
| Size | Consistent along course | Enlargement indicates pathology |
| Enhancement | Minimal or none with Gd | Enhancement suggests pathology |
| Course | Smooth, no deviation | Mass effect causes displacement |
Fascicular Pattern
Key Findings: Pathological Nerve Patterns
MRI Signs of Nerve Compression
| Finding | Description | Significance |
|---|---|---|
| Nerve enlargement | Increased cross-sectional area | Proximal to compression site |
| T2 hyperintensity | Increased signal (brighter than normal) | Oedema, inflammation |
| Calibre change | Abrupt narrowing at compression point | Indicates entrapment location |
| Notching | Flattening at compression site | External compression |
| Loss of fascicular pattern | Homogeneous signal | Fibrosis, chronic compression |
Carpal Tunnel Syndrome
Cubital Tunnel Syndrome
Muscle Denervation
MRI Appearance of Muscle Denervation
| Stage | Timeframe | T1 Signal | T2/STIR Signal | Reversibility |
|---|---|---|---|---|
| Acute | Less than 1 month | Normal | High (oedema) | Fully reversible |
| Subacute | 1-6 months | Normal to slightly high | High | Largely reversible |
| Chronic | Greater than 6 months | High (fatty) | Variable | Irreversible fatty infiltration |
OEDEMA Then FATDenervation Pattern
| O | O = Oedema-like signal (high T2) in acute phase |
| E | E = Early changes potentially reversible |
| F | F = Fatty replacement in chronic phase |
| A | A = Atrophy accompanies fatty change |
| T | T = Time determines reversibility |
| O | O = Oedema-like signal (high T2) in acute phase | A | A = Atrophy accompanies fatty change |
| E | E = Early changes potentially reversible | T | T = Time determines reversibility |
| F | F = Fatty replacement in chronic phase |
Hook:If you see muscle oedema in a specific nerve distribution, look for the nerve pathology upstream. Chronic denervation (fatty infiltration) indicates poor recovery potential.
Specific Nerve Imaging
Brachial Plexus MRI Assessment
| Structure | Location | Key Pathologies |
|---|---|---|
| Roots (C5-T1) | Exit neural foramina | Avulsion (pseudomeningocele), stretch |
| Trunks | Supraclavicular | Trauma, tumour, TOS |
| Divisions | Behind clavicle | Less commonly seen |
| Cords | Infraclavicular | Tumour, aneurysm compression |
| Branches | Axilla, arm | Specific nerve injuries |
Root Avulsion Signs
Differential Diagnosis on Nerve MRI
Distinguishing Causes of an Abnormal Nerve on MRI
| Entity | Key MRI Pattern | Discriminating Feature | Pitfall |
|---|---|---|---|
| Entrapment neuropathy | Proximal enlargement, T2 hyperintensity, calibre change at tunnel | Abnormality localises to a known fibro-osseous tunnel | Mild T2 signal can be normal at tunnels (magic-angle, partial volume) |
| Traumatic neuropathy | Discontinuity, neuroma-in-continuity, stump neuroma | History of trauma plus focal fusiform mass at injury level | Perineurial fibrosis may mimic enlargement |
| Schwannoma | Fusiform, eccentric to nerve, split-fat and target signs | Separable from parent fascicles; nerve passes at edge | Cystic/ancient change can look aggressive |
| Neurofibroma | Fusiform, central within nerve, target sign | Nerve enters and exits centrally; cannot be separated | Plexiform type in NF1 may harbour MPNST |
| MPNST | Over 5cm, ill-defined, heterogeneous, perilesional oedema, loss of split-fat | Absent split-fat sign, low ADC on DWI, rapid growth, NF1 | Target sign does NOT exclude malignancy |
| Intraneural ganglion | Cystic T2-bright tubular lesion tracking along nerve | Connection to adjacent joint (e.g. superior tibiofibular) | Mistaken for solid tumour |
| Lipomatosis of nerve (fibrolipomatous hamartoma) | Coaxial-cable / spaghetti appearance, fat between thickened fascicles | Macroscopic fat following fat signal on all sequences | May coexist with macrodactyly |
| Inflammatory / hereditary neuropathy | Diffuse symmetric multi-nerve thickening and T2 signal | Bilateral, non-focal, no tunnel localisation | Misread as multifocal entrapment |
Split-Fat Sign
Controversies & Areas of Uncertainty
MRI vs ultrasound vs nerve conduction studies
Is routine MRI needed in carpal tunnel syndrome?
Quantitative neurography (DTI, T2 mapping)
Significance of nerve T2 hyperintensity
Guidelines, Registries & Global Practice
Imaging Guidance for Peripheral Nerve Disorders (Society Positions)
| Body | Position on MRI / Neurography | Practical Implication |
|---|---|---|
| AAOS (US, CTS CPG) | Routine imaging not required to diagnose idiopathic CTS; electrodiagnostics support diagnosis | Reserve MRI for atypical or secondary causes |
| ACR Appropriateness Criteria (US) | MR neurography / high-resolution US usually appropriate for focal neuropathy and plexopathy | Modality choice guided by site and local expertise |
| NICE / BOA (UK) | Clinical and electrodiagnostic diagnosis first; imaging for atypical features or masses | MRI targeted, not screening |
| EFORT / European MSK radiology consensus | MR neurography and US complementary; 3T and dedicated coils recommended where available | Protocol and expertise dependent |
| ESSR (European Soc MSK Radiology) | Endorses high-resolution US and MR neurography with standardised nerve protocols | Drives reporting consistency |
Global epidemiology context
High- vs limited-resource practice
Registry / quality note
Evidence
Median nerve cross-sectional area at the pisiform is enlarged in carpal tunnel syndrome
- Retrospective comparison of 164 wrists: 67 with clinically and electrodiagnostically confirmed CTS versus 97 controls.
- Mean median nerve cross-sectional area at the pisiform level was 18.8 mm² in CTS versus 12.1 mm² in controls (p less than 0.05).
- Cross-sectional area at the hook of hamate did not differ significantly between groups.
3T MRI nerve cross-sectional area correlates with electrodiagnostic severity in CTS
- 70 wrists of 35 patients with unilateral idiopathic CTS imaged at 3T with nerve conduction studies.
- Median nerve cross-sectional area was greatest at the scaphoid body level and positively correlated with distal motor latency.
- Cross-sectional area at the distal radioulnar joint and hamate hook did not correlate with severity.
Absent split-fat sign and ADC best discriminate malignant from benign nerve sheath tumours
- 87 peripheral nerve sheath tumours; 55 indeterminate lesions analysed (18 malignant, 37 benign) with conventional and diffusion-weighted MRI.
- Size, margin, perilesional oedema and split-fat, fascicular and target signs differed between benign and malignant tumours.
- Combining mean ADC value with absence of the split-fat sign gave a C-index greater than 0.9 for identifying MPNST.
MRI features of neurogenic tumours and tumour-like lesions
- Review of neurogenic tumours and pseudotumours: traumatic and Morton neuroma, lipomatosis of nerve, nerve sheath ganglion, perineurioma and benign/malignant PNST.
- Defining MRI clues include nerve entering or exiting the mass, fusiform shape, split-fat sign, target sign, fascicular appearance and denervation of the supplied muscle.
- No single finding reliably separates benign from malignant lesions; pattern recognition guides diagnosis.
3D MR neurography enables multiplanar peripheral nerve assessment
- Review of high-resolution isotropic 3D MR neurography acquisition and clinical applications.
- 3D techniques allow multiplanar reconstruction along tortuous nerves plus anatomical and functional tissue characterisation.
- Applications span entrapment, trauma, inflammatory/infectious neuropathies and neoplasms.
MR neurography is feasible around orthopaedic hardware with metal-artifact reduction
- Technical review of MR neurography for peripheral nerve injury in the presence of metallic hardware.
- Conventional 2D proton-density and T2 fat-suppressed sequences plus 3D reversed steady-state and multispectral techniques reduce susceptibility artifact.
- Real-time radiologist monitoring and protocol optimisation improve diagnostic yield near metal.
MR neurography and high-resolution ultrasound are complementary for nerve imaging
- Review correlating MR neurography with high-resolution ultrasound for peripheral nerve assessment.
- Both modalities provide detailed nerve anatomy and pathology with optimised technique.
- Reported diagnostic accuracy largely reflects local expertise and access to current technology.
Foundational description of MR neurography of peripheral nerves
- Early review establishing direct MR visualisation of normal-sized major peripheral nerves using phased-array surface coils.
- Described the imaging appearance of normal nerve plus traumatic, compressive and neoplastic pathology.
- Illustrated brachial and lumbosacral plexus, carpal tunnel and cubital tunnel imaging.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 45-year-old presents with hand numbness and thenar weakness. Nerve conduction studies confirm carpal tunnel syndrome. The hand surgeon requests MRI."
"A patient presents after a motorbike accident with a flail arm. Clinical examination suggests brachial plexus injury. What would you expect on MRI?"
"A 30-year-old presents with a slowly enlarging painless mass in the forearm. Ultrasound shows a fusiform mass along the course of a nerve."
MRI Neurography Quick Reference
Clinical summary
Normal Nerve Appearance
- •T1: Intermediate (like muscle)
- •T2: Mildly hyperintense to muscle
- •Fascicular pattern (honeycomb)
- •Size consistent along course
Compression Signs
- •Nerve enlargement proximal to compression
- •T2 hyperintensity (oedema)
- •Calibre change at compression point
- •Loss of fascicular pattern
Carpal Tunnel Criteria
- •Median nerve greater than 10mm² at pisiform
- •Palmar bowing of retinaculum
- •Nerve flattening within tunnel
- •Thenar denervation (late)
Denervation Pattern
- •Acute: High T2, normal T1 (oedema)
- •Chronic: High T1 (fatty infiltration)
- •Distribution follows nerve supply
- •Identifies level of injury