Central Third | Watershed Area | High Nonunion Risk
- High-risk stress fracture of the central sagittal navicular — classically attributed to a relatively avascular central third, though cadaver work shows a true central avascular zone in only ~12% (McKeon 2012), so biomechanical loading is increasingly emphasised
- MRI is the most sensitive test — plain radiographs are frequently normal early; the Saxena classification is graded on coronal/frontal-plane CT (Type I dorsal cortical break, II into body, III both cortices)
- Strict non-weight-bearing immobilisation is the standard of care — Torg's meta-analysis: NWB 96% union vs weight-bearing rest only 44%; activity restriction with weight-bearing is inadequate
- Surgery (single/double cannulated screw, medial to lateral) offers no proven advantage over NWB for outcome or return-to-sport time, but is used for complete/displaced fractures, nonunion, or elite athletes
- Nonunion is the feared complication — driven mainly by inadequate immobilisation and delayed diagnosis; established nonunion or sclerosis may need ORIF with bone grafting (vascularised graft for revision/AVN)
- “Standard of care = strict NWB immobilisation (NWB 96% vs WB 44% union, Torg 2010)
- “MRI most sensitive; Saxena classification graded on CT
- “Surgery shows no outcome advantage over NWB in meta-analysis
- “'N spot' tenderness over the navicular is the key clinical sign
| Type | CT Finding | Typical Treatment | Note |
|---|---|---|---|
| Type I | Dorsal cortical break only | NWB cast/boot 6-8 weeks | Best prognosis; nonop usually sufficient |
| Type II | Fracture into navicular body | NWB; ORIF if athlete/incomplete healing | Saxena recommended ORIF for II/III |
| Type III | Both cortices breached (complete) | ORIF / cannulated screw +/- graft | Higher nonunion risk if WB or sclerotic |
In Torg's meta-analysis, fracture type did not correlate with treatment outcome once non-weight-bearing immobilisation was used — the dominant determinant of union is strict NWB, not the Saxena grade. Saxena's own series advocated ORIF for Type II/III to speed return to sport, but later evidence found no return-to-sport advantage over NWB.
WATERSHEDNavicular Stress Fracture Features
Hook:WATERSHED: Watershed area (central 1/3), Arterial supply poor, Tensile stress high, Edema on MRI, Risk of nonunion high, Sagittal orientation, Healing slow, Elite athletes affected, Diagnosis by MRI!
NWBTreatment Decision
Hook:NWB: Non-weight bearing strict 6-8 weeks, Weight bearing delayed, Bearing only after healing confirmed!
MRIDiagnosis
Hook:MRI: MRI most sensitive, Radiographs often normal early, Imaging by CT classifies (Saxena) and confirms union!
Overview and Epidemiology
Navicular stress fractures are high-risk stress fractures of the tarsal navicular, typically oriented in the sagittal plane through the central body. They are classified high-risk because the central body is under high tensile load and is the slowest-healing segment, giving a meaningful risk of delayed union and nonunion if not properly immobilised. First described in 1970, they are now well recognised in jumping and sprinting athletes.
Definition and key features
- Location: Central body of the navicular, sagittally oriented (vertical)
- Mechanism: Fatigue failure under repetitive high tensile/compressive load (sprinting, jumping)
- Classification: Saxena CT classification (Type I dorsal cortical break, II into body, III both cortices)
- Why high-risk: Slow healing in the central body; traditionally attributed to a relatively avascular central third, though this is now disputed (see Controversies)
Epidemiology
- Frequency: Uncommon (a small percentage of all stress fractures) but disproportionately important because of nonunion risk
- Demographic: Young athletes, peak in the 2nd-3rd decades; in adolescents (Mehta 2023) there was a female predominance (~65%) in leanness/endurance sports
- Sports: Track and field/running, sprinting, jumping, gymnastics/dance, basketball, football/soccer
- Risk factors: Training error (rapid load increase), biomechanics (cavus foot, restricted ankle dorsiflexion, short first metatarsal/metatarsus adductus), and bone-health factors (RED-S / relative energy deficiency in sport, low BMD, the female athlete triad)
The label "high-risk" reflects the consequence of treatment failure (delayed union/nonunion), not a high incidence. The single most important determinant of union is strict non-weight-bearing immobilisation — the meta-analysis showed 96% union with NWB vs 44% with weight-bearing rest.
Anatomy and Pathophysiology
Navicular Anatomy
Tarsal navicular:
- Location: Midfoot, between talus and cuneiforms
- Function: Keystone of medial longitudinal arch
- Articulations: Talus (proximal), three cuneiforms (distal), cuboid (lateral)
- Blood supply: Dorsalis pedis (dorsal), medial plantar artery (plantar)
Blood supply (and the modern caveat):
- Dorsal surface: Medial tarsal branches of the dorsalis pedis (consistent, ~96% of specimens)
- Plantar surface: Branches of the medial plantar artery (from posterior tibial)
- Classic teaching: A relatively avascular "watershed" central third between these systems, predisposing the central body to fracture and nonunion
- Modern evidence (McKeon 2012, cadaver): Most naviculars (30 of 54) have diffuse intraosseous flow; a true central avascular zone was found in only ~12%. This implies vascular anatomy alone does not explain most fractures and that biomechanical overload is the dominant factor
Pathophysiology
Stress fracture mechanism:
- Repetitive high load: The navicular is the keystone of the medial arch; sprinting/jumping transmit large compressive and shear forces across the central body
- Sagittal fracture plane: Tensile/shear concentration produces a vertical (sagittal) fracture line through the central body
- Fatigue failure: Repetitive loading outpaces remodelling, especially with training error or impaired bone health (RED-S)
Why it heals slowly / risks nonunion:
- Mechanical: Ongoing weight-bearing maintains shear across the fracture and prevents union — the key modifiable factor
- Biological: Slow remodelling in dense central cancellous bone; a minority have genuinely reduced central perfusion
- Diagnostic delay: Frequently missed because early radiographs are often normal, allowing the fracture to progress before treatment
Classification Systems
Saxena CT Classification (graded on coronal/frontal-plane CT)
Type I: Dorsal cortical break only (incomplete)
- Best prognosis; non-weight-bearing immobilisation usually sufficient
Type II: Fracture extends into the navicular body
- NWB; Saxena advocated ORIF to expedite return in athletes
Type III: Both cortices breached (complete fracture)
- Highest risk if weight-bearing or sclerotic; ORIF +/- bone graft often used
Saxena recommended ORIF for Type II/III, but Torg's meta-analysis later found type did not predict outcome once strict NWB was used.
Clinical Assessment
History
Symptoms:
- Midfoot / medial arch pain: Often vague and poorly localised, especially with activity
- "N spot" tenderness: Focal tenderness over the dorsal navicular — the classic sign
- Activity-related: Pain with running, sprinting, jumping, cutting; eased by rest
- Gradual onset: Insidious, no discrete traumatic event
Risk factors:
- Training errors (sudden increase in intensity/duration)
- Biomechanical issues (overpronation, cavus foot)
- Bone health (low bone density, female athlete triad)
- Footwear (inadequate support)
Physical Examination
Inspection:
- Swelling (may be minimal)
- Deformity (rare)
Palpation:
- "N spot" tenderness: Focal tenderness over the dorsal navicular (key sign)
- Midfoot tenderness
- No acute traumatic mechanism
Range of Motion:
- Midfoot ROM may be limited
- Pain with midfoot stress
Special tests:
- "N spot" palpation: Tenderness over navicular
- Single-leg hop: Pain with loading
- Midfoot stress: Pain with inversion/eversion
The "N spot" — focal tenderness over the dorsal navicular — is the classic localising sign and should raise suspicion in any athlete with poorly localised midfoot/medial arch pain. Because plain radiographs are frequently normal early, a positive N spot with activity-related pain warrants advanced imaging (MRI most sensitive; CT to classify and assess union).
Investigations
Standard X-ray Protocol (weight-bearing foot series)
AP / lateral / oblique views:
- Frequently normal early — the diagnosis requires a high index of suspicion (Pavlov/Torg 1983)
- Late changes: a sclerotic fracture line, fragmentation, or cyst formation in chronic cases
Key point: A normal radiograph does NOT exclude the diagnosis — proceed to MRI/CT if clinical suspicion is high.
Management Algorithm
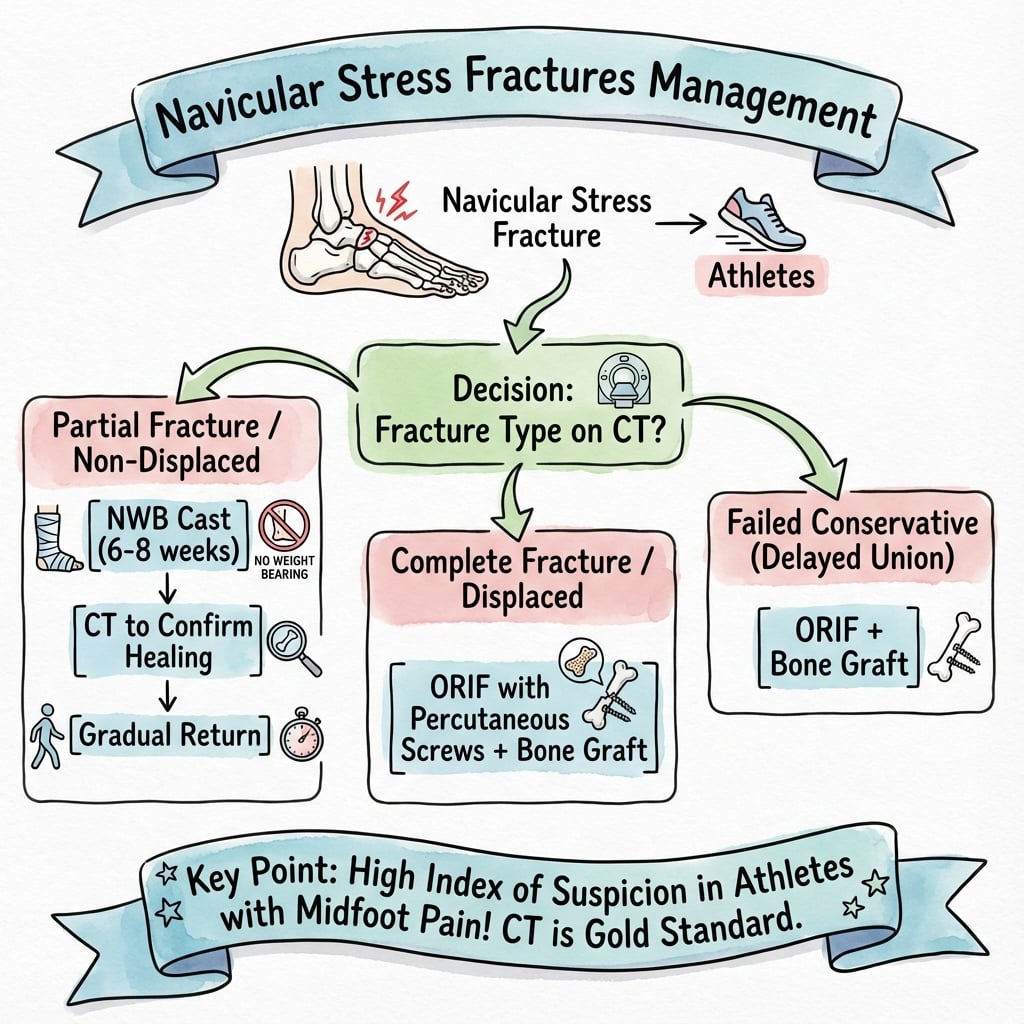
Management Pathway
Navicular Stress Fracture Management
Athlete with activity-related midfoot pain and a positive "N spot". Radiographs are often normal early — obtain MRI (most sensitive) to confirm and CT to classify (Saxena type) and assess sclerosis/union.
Non-weight-bearing cast or boot for ~6-8 weeks is the standard of care (NWB 96% union vs weight-bearing rest 44%, Torg 2010). Weight-bearing activity restriction alone is inadequate. Address training load, biomechanics and bone-health/RED-S.
At ~6-8 weeks, confirm union on CT and check that the N spot is non-tender before progressive weight-bearing and a graded return to running. If not healed, continue immobilisation or consider fixation.
For complete (Type III)/displaced fractures, established nonunion, sclerosis, or failed conservative care: cannulated screw fixation (single or double, medial to lateral). Established nonunion/AVN may need ORIF with bone grafting (vascularised graft achieved 100% union in Nunley's series).
Surgical Technique
Percutaneous Screw Fixation (Preferred)
Indications:
- Failed conservative treatment
- Displaced fracture
- Complete fracture with sclerosis
Approach:
- Medial stab incision
- Guidewire placement under fluoroscopy
- Screw fixation
Technique:
- Exposure: Medial stab incision near the navicular tuberosity
- Guidewire: Place from medial to lateral, perpendicular to the fracture, under fluoroscopy
- Verification: Confirm position on AP, lateral and oblique views
- Screw: Cannulated lag screw (commonly 4.0-4.5mm); single or double screws (double increasingly used for rotational control)
- Compression: Lag technique / partially threaded screw across the fracture
- Verification: Confirm reduction and hardware position fluoroscopically; avoid joint penetration
Advantages:
- Minimally invasive, provides interfragmentary compression
- Suited to acute complete fractures without sclerosis
Note: For complete fractures without nonunion, percutaneous fixation is reasonable; established nonunion or sclerosis usually requires open debridement and grafting.
Complications
| Complication | Driver | Risk Factors | Prevention/Management |
|---|---|---|---|
| Delayed union / nonunion | Main concern | Weight-bearing during treatment, delayed diagnosis, sclerosis | Strict NWB immobilisation; ORIF + bone graft if established |
| Missed / delayed diagnosis | Common | Normal early radiographs, vague pain | High index of suspicion, early MRI |
| Refracture / recurrence | Possible | Premature return, uncorrected biomechanics/RED-S | Confirm union on CT, graded return, address risk factors |
| AVN / fragmentation | Uncommon | Established nonunion, central sclerosis | Vascularised bone graft for revision (100% union, Nunley 2021) |
Nonunion (the key complication)
- Cause: Most often inadequate immobilisation (weight-bearing during treatment) and delayed diagnosis; biology contributes in a minority
- Prevention: Strict NWB immobilisation and CT-confirmed union before loading — the single biggest modifiable factor
- Management: ORIF with debridement of sclerotic bone and autograft; vascularised bone graft for difficult revisions or AVN (Nunley reported 100% union with vascularised grafting vs 75-80% for ORIF +/- non-vascularised graft)
Delayed union
- Cause: Inadequate or premature loading, uncorrected risk factors
- Management: Extend immobilisation, re-image with CT, and reassess training load and bone health before considering fixation
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- CT to confirm healing
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes (verified figures)
- Union rate
- ~96%
- Source
- Torg meta-analysis 2010
- Union rate
- ~44%
- Source
- Torg meta-analysis 2010
- Union rate
- ~82%
- Source
- Torg meta-analysis 2010
- Union rate
- ~80%
- Source
- Nunley 2021
- Union rate
- ~75%
- Source
- Nunley 2021
- Union rate
- 100%
- Source
- Nunley 2021
- Union rate
- ~85% successful
- Source
- Mehta 2023
- Return to sport: Typically ~3-4 months in athletes (Saxena 2006 reported ~4 months for both operative and non-operative); the meta-analysis found no difference in return-to-activity time between NWB and surgery. In adolescents, operative cases returned in a median of ~5 months and took longer than non-operative cases (Mehta 2023).
Long-Term Prognosis
- With strict NWB immobilisation the great majority unite and return to sport
- The dominant determinants of a poor outcome are weight-bearing during treatment and delayed diagnosis — not fracture type
- Recurrence risk is reduced by confirming union on CT, a graded return, and correcting training load, biomechanics and bone-health/RED-S factors
Differential Diagnosis
Activity-related midfoot/medial arch pain in an athlete has a broad differential. The navicular stress fracture is the diagnosis not to miss.
| Condition | Key features | Distinguishing point |
|---|---|---|
| Navicular stress fracture | Insidious midfoot pain, positive 'N spot', often normal early X-ray | Sagittal central-body line on MRI/CT; high-risk for nonunion |
| Posterior tibial tendinopathy | Medial pain/swelling along tendon, weak single-heel-rise, progressive flatfoot | Tenderness along the tendon, not focal over the navicular |
| Accessory navicular / os tibiale externum | Medial prominence, pain at tuberosity, often bilateral | Ossicle at medial tuberosity on imaging; chronic, not a sagittal body line |
| Midfoot (Lisfranc/TMT) osteoarthritis | Dorsal midfoot pain, stiffness, older or post-injury | Joint-space narrowing/osteophytes on weight-bearing X-ray |
| Kohler disease (paediatric) | Child with limp and medial midfoot pain | Sclerotic, flattened navicular in a child; self-limiting osteochondrosis |
| Other tarsal/metatarsal stress fracture | Activity-related forefoot/midfoot pain | Localising tenderness and MRI/CT site differ |
Controversies and Areas of Uncertainty
The historical "watershed/avascular central third" explanation is challenged by McKeon's cadaver study, where most naviculars had diffuse intraosseous flow and only ~12% had a true central avascular zone. Many authors now emphasise mechanical overload over vascular anatomy as the dominant cause.
Surgery is often offered to athletes for a "faster, more predictable" recovery, yet Torg's meta-analysis showed no outcome or return-to-sport advantage over NWB (and a trend favouring NWB). The genuine surgical indications (complete/displaced fracture, nonunion, sclerosis, failed NWB) are clearer than the "elite athlete shortcut".
Saxena's CT classification drives an operative algorithm for Type II/III, but the meta-analysis found type did not correlate with outcome once NWB was used. Whether higher Saxena/BSI grade should change first-line treatment remains debated.
Optimal fixation is not standardised — single vs double cannulated screws, and when to add bone graft. Evidence supports vascularised grafting for sclerotic/avascular nonunion (100% union, Nunley), but routine graft choice in primary fixation is unsettled.
If asked "why does it occur in the central third?", give the classic tensile-load + relative-avascularity answer but show awareness that the avascular-zone theory is overstated (only ~12% in cadaver work) and that biomechanical overload and bone-health factors (RED-S) are increasingly emphasised. This nuance separates a pass from a strong pass.
Evidence Base
Conservative vs surgical treatment — landmark meta-analysis
- NWB 96% vs weight-bearing rest 44% successful (P=.0001)
- Surgery 82%; no significant advantage over NWB (P=.64)
- Fracture type did not predict outcome
- NWB immobilisation is the standard of care for partial AND complete fractures
Original case series defining the injury
- Defined the injury in athletes with vague midfoot pain
- Sagittal fracture through the central navicular body
- Radiographs frequently unhelpful — high suspicion needed
- Established immobilisation as treatment
Saxena CT classification — prospective athlete cohort
- Defines the Saxena CT classification (I/II/III)
- Return to activity ~4 months regardless of type/treatment
- Advocated ORIF for Type II/III to standardise care
- CT scan guides severity assessment
Arterial anatomy — challenges the avascular dogma
- Diffuse intraosseous flow in most naviculars
- True central avascular zone in only ~12%
- Dorsalis pedis supplies dorsal bone in ~96%
- Mechanical loading likely dominates over vascularity
High-risk stress fractures — narrative review
- Navicular is a recognised high-risk stress fracture
- High-risk sites share high tension + low blood flow
- Require early imaging and aggressive offloading
- Greater risk of progression and nonunion than low-risk sites
Operative algorithm including vascularised grafting
- Algorithmic surgery by chronicity/sclerosis
- ORIF alone 80%, +graft 75%, +vascularised graft 100% union
- Vascularised grafting beneficial for the most difficult cases
- Return to sport similar across operative groups
Adolescent multicentre series
- Non-operative success 85% in adolescents
- Female predominance in leanness/endurance sports
- Visible fracture line predicts need for surgery
- Operative cases returned to sport later (~5 months)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old elite runner presents with 6 weeks of midfoot pain, worse with running. Clinical examination shows 'N spot' tenderness over navicular. X-rays are negative. MRI shows bone marrow edema and fracture line in central 1/3 of navicular (sagittal orientation).”
“A 25-year-old athlete has a navicular stress fracture treated conservatively with 8 weeks non-weight-bearing. CT at 8 weeks shows persistent fracture line with sclerotic margins (nonunion). Patient has persistent pain and wants to return to sport.”
“A 15-year-old female cross-country runner has 2 months of vague medial midfoot pain. She has a positive 'N spot'. She has a low BMI, irregular periods, and has recently increased her mileage. Radiographs are normal.”
MCQ Practice Points
Q: Why do navicular stress fractures occur in the central body? A: High tensile/compressive load across the keystone of the medial arch produces a sagittal fracture in the central body. Classically attributed to a relatively avascular central third, but cadaver work (McKeon 2012) found a true central avascular zone in only ~12%, so mechanical overload is now emphasised.
Q: How are navicular stress fractures diagnosed and classified? A: Suspect on a positive 'N spot' with activity-related midfoot pain. Radiographs are frequently normal early. MRI is the most sensitive test; CT defines the Saxena classification (I dorsal cortical break, II into body, III both cortices) and confirms union.
Q: What is the standard of care? A: Strict non-weight-bearing immobilisation (cast/boot) for ~6-8 weeks. Torg's meta-analysis: NWB 96% union vs weight-bearing rest 44% — weight-bearing activity restriction is inadequate. Confirm union on CT before progressive loading.
Q: Does surgery beat non-operative treatment? A: No proven advantage. In the meta-analysis surgery achieved ~82% union with no significant outcome or return-to-sport benefit over NWB. Reserve cannulated-screw fixation for complete/displaced fractures, nonunion, sclerosis, or failed NWB.
Q: What drives nonunion and how is it managed? A: Mainly weight-bearing during treatment and delayed diagnosis. Established sclerotic nonunion needs ORIF with debridement and grafting; vascularised bone grafting achieved 100% union in the most difficult cases (Nunley 2021).
Guidelines, Registries & Global Practice
Global epidemiology
- Uncommon overall but a disproportionately important high-risk stress fracture in running, sprinting, jumping, gymnastics and military/endurance populations worldwide
- Bone stress injuries cluster where energy availability is low — RED-S/female athlete triad is a globally recognised driver, particularly in adolescent and female endurance athletes (Mehta 2023)
Society guidance and consensus (side by side)
- Position on navicular stress fracture
- Frame as a bone stress injury; screen and treat low energy availability; grade and risk-stratify before return-to-sport
- Position on navicular stress fracture
- High-risk stress fracture; early advanced imaging, non-weight-bearing immobilisation, cautious staged return
- Position on navicular stress fracture
- General stress/insufficiency-fracture principles: investigate persistent activity-related bone pain, address bone health, multidisciplinary care
- Position on navicular stress fracture
- For operative cases: anatomic reduction, interfragmentary compression (lag screw), bone grafting of established nonunion
There is broad international agreement that strict non-weight-bearing immobilisation is first-line and that surgery is reserved for complete/displaced fractures, nonunion or failed conservative care.
Registry note
There is no dedicated navicular-stress-fracture implant registry (these are not arthroplasty). Evidence comes from athlete case series and the Torg meta-analysis rather than national joint registries.
High- vs limited-resource practice variation
- Well-resourced settings: Ready MRI/CT access enables early diagnosis, BSI grading and CT-confirmed union; multidisciplinary RED-S management; vascularised grafting available for revision
- Limited-resource settings: Diagnosis may rely on clinical suspicion plus radiographs (often normal) with consequent delay; treatment defaults to prolonged strict non-weight-bearing immobilisation — fortunately the highest-yield, low-cost intervention and the proven standard of care
A common foot-and-ankle viva. Anchor your answer on the verified evidence: strict NWB immobilisation is the standard of care (96% vs 44% union vs weight-bearing rest, Torg 2010); surgery has no proven advantage; suspect on the N spot, image with MRI (most sensitive) and classify on CT (Saxena); and show awareness that the "avascular central third" theory is overstated. Be ready to discuss nonunion management (debride + graft, vascularised graft for the hardest cases) and RED-S.