Biology and Technique
Injury Types (Seddon/Sunderland)
Critical Must-Knows
- Wallerian Degeneration occurs distal to the injury site.
- Regeneration proceeds at ~1mm/day (or 1 inch/month).
- Tension-free repair is the single most important surgical principle.
- Primary repair is preferred if clean and no gap.
- Grafts (Autograft) are the Gold Standard for gaps.
- Conduits are acceptable for small gaps (less than 2cm) in small diameter nerves.
Clinical Pearls
- "Motor End Plates die after 12-18 months ('Time is Muscle').
- "Sensation can recover years later (though quality diminishes).
- "The most common cause of failure is tension at the repair site.
Clinical Imaging
Imaging Gallery



The Trap: 'Wait and See'
The Problem
Uncertain Diagnosis In closed injuries, it's hard to tell Axonotmesis from Neurotmesis. Waiting 3-6 months is standard.
The Exception
Open Injuries If there is a penetrating wound and a deficit, Assume the nerve is CUT. Do NOT wait. Explore early.
| Feature | Neurapraxia | Axonotmesis | Neurotmesis |
|---|---|---|---|
| Pathology | Myelin Block | Axon cut / Sheath intact | Complete Transection |
| Wallerian Degen | No | Yes | Yes |
| Tinel's | No (or at site) | Yes (Moves distal) | Yes (Stays at site) |
| Recovery | Hours to Weeks | Months (1mm/day) | None without surgery |
| Surgery | No | No | Yes |
My Axon Endo Peri EpiSunderland Classification
| 1 | Myelin Conduction block (Neurapraxia). |
| 2 | Axon Axon cut (Axonotmesis). |
| 3 | Endoneurium Endoneurium cut. |
| 4 | Perineurium Perineurium cut. |
| 5 | Epineurium Complete transection (Neurotmesis). |
| 1 | Myelin Conduction block (Neurapraxia). | 4 | Perineurium Perineurium cut. |
| 2 | Axon Axon cut (Axonotmesis). | 5 | Epineurium Complete transection (Neurotmesis). |
| 3 | Endoneurium Endoneurium cut. |
Hook:Layers breached from inside out.
TIPSSurgical Principles
| T | Tension-free Crucial. |
| I | Ischemia Good vascular bed. |
| P | Preparation Cut back to healthy fascicles. |
| S | Suture Microsurgical technique (9-0 or 10-0). |
| T | Tension-free Crucial. | P | Preparation Cut back to healthy fascicles. |
| I | Ischemia Good vascular bed. | S | Suture Microsurgical technique (9-0 or 10-0). |
Hook:Tips for nerve repair.
SAMSDonor Nerves
| S | Sural Standard for long gaps. |
| A | AIN Anterior Interosseous (Motor donor). |
| M | MABC Medial Antebrachial Cutaneous. |
| S | Saphenous Alternative lower limb donor. |
| S | Sural Standard for long gaps. | M | MABC Medial Antebrachial Cutaneous. |
| A | AIN Anterior Interosseous (Motor donor). | S | Saphenous Alternative lower limb donor. |
Hook:SAMS nerves.
Overview
Terminology
Wallerian Degeneration: The process where the distal axon segment disintegrates and is cleared by macrophages/Schwann cells, creating a tube for the new axon to grow into. Bands of Bungner: The columns of Schwann cells that guide the regenerating axon.
Peripheral nerve injury creates a race between axonal regeneration and end-organ atrophy. Axons regenerate at roughly 1 mm/day, but denervated motor end plates degrade irreversibly by 12-18 months. The whole of nerve surgery is an attempt to win that race: minimise the regeneration distance (transfers), maximise the quality of the conduit (tension-free coaptation, autograft), and preserve the target (timely reconstruction, splinting).
Three questions frame every nerve case:
- Is it cut? Open injury with a deficit is assumed to be neurotmesis until proven otherwise.
- Can it be repaired without tension? If not, it needs a graft, conduit or transfer.
- Is there still a target to reinnervate? Beyond the motor window, the answer shifts from nerve reconstruction toward tendon transfer.
Pathophysiology
Wallerian Degeneration
Following nerve transection, the distal segment undergoes Wallerian degeneration—a coordinated destruction and clearance process:
Timeline:
- 0-24 hours: Axoplasm granulates, neurofilaments fragment
- 24-48 hours: Calcium influx triggers cytoskeletal breakdown
- Days 3-7: Schwann cells dedifferentiate and proliferate
- Weeks 2-4: Macrophages infiltrate and phagocytose myelin debris
- Weeks 4-8: Complete clearance creates "empty tubes" for regeneration
Molecular Events:
- c-Jun activation in Schwann cells: Master transcription factor for dedifferentiation
- Myelin breakdown: Cholesterol-rich debris must be cleared before regeneration
- Neurotrophic factor release: NGF, BDNF, GDNF guide regenerating axons
Axonal Regeneration
The proximal stump forms a growth cone—a specialized structure that navigates toward target tissues:
Growth Cone Function:
- Filopodia (finger-like projections) sample the environment
- Respond to chemoattractants (neurotrophins) and repellents (semaphorins)
- Require intact endoneurial tubes for successful guidance
Rate of Regeneration:
- Standard rate: 1 mm/day (1 inch/month)
- Faster in children, slower in elderly
- Faster proximally, slower distally
- Calculate expected recovery: Distance to target ÷ 1mm/day + latent period (1 month)
End-Organ Atrophy
Motor End Plate Degeneration:
- Begin to atrophy at 3-6 months
- Irreversible changes by 12-18 months
- Cannot be reinnervated after permanent fibrosis
- This is the "biological clock" that limits proximal repairs
Sensory Receptors:
- More resilient than motor end plates
- Can recover even years after injury
- Quality diminishes over time (never normal 2-point discrimination)
Factors Affecting Regeneration
| Factor | Better Outcome | Worse Outcome |
|---|---|---|
| Age | Children | Adults greater than 60 |
| Level | Distal | Proximal |
| Mechanism | Sharp cut | Crush/avulsion |
| Timing | Early repair | Delayed repair |
| Gap | Direct repair | Long graft |
| Nerve | Pure motor/sensory | Mixed nerve |
Anatomy
Wallerian Degeneration
- Starts: 24-48 hours post-injury.
- Process: Calcium influx leads to Cytoskeleton breakdown leads to Axon and Myelin digestion.
- Clearance: Macrophages clear debris (takes weeks).
The distal stump must be cleared before the new axon can enter.
This latent period is why early repair doesn't mean immediate regeneration.
Classification Systems
Immediate Repair (less than 24-48 hours)
- Indications: Sharp, clean lacerations.
- Pros: Anatomy is clear, no retraction, single procedure.
- Cons: Emergency setting (maybe less optimal team).
Standard of care for clean glass/knife injuries.
Clinical Assessment
History
- Mechanism: Sharp vs Blunt vs Traction.
- Time: Duration since injury.
- Age: Patient age (prognostic).
Examination
- Motor: Test individual muscles (MRC grade).
- Sensory: Light touch, 2PD (Static/Moving).
- Tinel's: Percuss over nerve. Distal advancement sign of regeneration.
Investigations
Nerve Conduction Studies
- Timing: Wait 3-4 weeks for Wallerian degeneration to complete (otherwise distal stump conducts).
- Findings: Denervation potentials (Fibs/Positive Sharp Waves) in muscle.
A baseline study at 3-4 weeks is standard for monitoring.
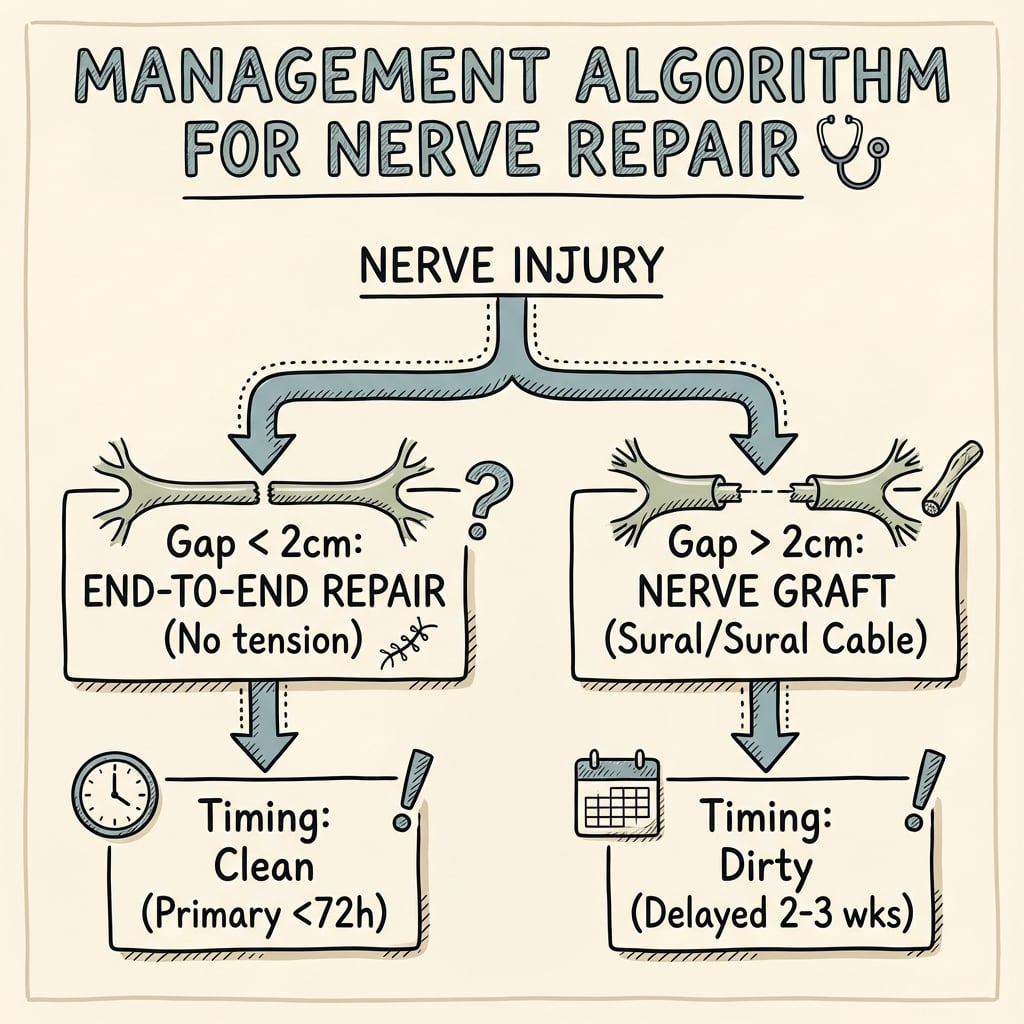
Management Algorithm
Autografts (Gold Standard)
- Indication: Any gap that cannot be closed without tension.
- Donor: Sural (calf), MABC (arm), LABCN (forearm).
- Technique: Cable grafting (multiple strands).
- Pros: Contains Schwann cells + basal lamina.
- Cons: Donor site morbidity (numbness).
Must reverse the graft direction if using Sural nerve (valves).
Surgical Technique
Epineurial Repair
- Standard: For most digital/peripheral nerves.
- Suture: 8-0, 9-0, or 10-0 Nylon.
- Goal: Align surface vessels (vasa nervorum) to ensure rotational alignment.
- Technique: 2-4 sutures in the epineurium. Avoid entering the fascicles.
Faster and less inflammatory than fascicular repair.
The key is to avoid tension which causes ischemia.
Nerve Transfers
Concept: "Rob Peter to Pay Paul". Using a redundant or expendable proximal nerve branch to reinnervate a critical distal target.
- Goal: Bypass the injury site and reduce regeneration distance.
- Example:
- Oberlin Transfer: Ulnar fascicle to Biceps (for Musculocutaneous injury).
- AIN to Ulnar: For high ulnar nerve palsy.
- Spinal Accessory to Suprascapular: For Brachial Plexus injury.
Advantage: Converts a high level injury into a low level injury (faster recovery).
Differential Diagnosis & Decision-Making
The clinical challenge is rarely "is there a nerve problem" but "which lesion, and does it need surgery now". The differential is really a grading and timing problem.
| Scenario | Likely lesion | Distinguishing clue | Action |
|---|---|---|---|
| Closed injury, deficit, recovering Tinel advancing distally | Neurapraxia / axonotmesis | Tinel marches distally over weeks | Observe; serial exam and EMG |
| Closed injury, no recovery by 3 months, Tinel static | Neurotmesis-in-continuity / neuroma | Tinel stays at injury site; EMG no reinnervation | Explore and reconstruct |
| Open laceration, immediate deficit | Transection (neurotmesis) | Penetrating wound over nerve path | Assume cut; early exploration |
| Sudden global limb palsy after dislocation | Traction / plexus lesion | Multiple territories, Horner sign | Image (MRI, CT myelogram); consider transfer |
| Painful percussion lump, no useful function | Stump neuroma | Focal Tinel, no progression | Desensitize, then surgery if refractory |
| Diffuse pain, swelling, allodynia out of proportion | CRPS (mimic) | Vasomotor/trophic change, not a single territory | Pain team; do not re-operate blindly |
The two clinical signs that drive the decision are an advancing versus static Tinel sign and the presence or absence of reinnervation on serial EMG at around 3 months.
Controversies & Areas of Uncertainty
Epineurial vs Fascicular Repair
Group-fascicular repair is theoretically more precise for mixed nerves, but randomized and comparative data have not consistently shown superiority over epineurial repair, while adding scar burden and operative time.
Allograft vs Autograft for Long Gaps
Registry and meta-analysis data suggest comparable meaningful recovery for short-to-moderate gaps, but high-quality head-to-head evidence for long motor gaps (over 50-70 mm) is limited, and autograft remains the reference for critical motor defects.
Conduit Gap Limit
The commonly quoted ceiling is 2-3 cm in small sensory nerves, but the exact threshold is expert-opinion based, not defined by a single trial; outcomes deteriorate as gap and nerve diameter increase.
Timing of Closed-Injury Surgery
The "wait 3 months" rule balances spontaneous recovery against the motor end-plate clock. There is genuine uncertainty about the optimal cut-off, and earlier nerve transfer is increasingly favoured for proximal injuries to beat the clock.
Complications
- Neuroma: Painful lump at repair site (failed regeneration).
- CRPS: Pain syndrome.
- Failure of Motor Recovery: Atrophy and irreversible motor end-plate fibrosis (the biological clock).
- Cold Intolerance: Permanent symptom in almost all nerve injuries.
- Mismatch: Sensory axon growing into motor tube (wasted).
- Cross-talk: Synkinesis (rare in peripheral, common in facial nerve).
Postoperative Care
- Splint: Protective position (relieve tension).
- Motion: Protected gliding (controlled active motion) to prevent adhesion.
- Wean Splint: Gradual extension.
- Desensitization: Texture exposure.
- Sensory: Discriminative training (Dellon).
- Motor: Biofeedback / Mirror therapy.
Neural plasticity plays a huge role in outcome.
Prognosis
- Factors:
- Age: The most important factor. Children regenerate excellently. Adults greater than 60 poorly.
- Level: Distal is better than Proximal.
- Type: Sharp cut better than Crush/Avulsion.
- Gap: Tension kills repair.
- Delay: Repair within 3 months is best.
- Outcome: Normal 2PD is rarely achieved in adults (~6-10mm is good).
Evidence Base
Interfascicular Grafting (Tension Principle)
- Series of median and ulnar nerve injuries reconstructed with interfascicular nerve grafts
- Established that a tension-free graft outperforms a primary repair held together under tension
- Articulated the principle that tension at the coaptation causes ischaemia and intraneural fibrosis
Oberlin Transfer (Original Description)
- Four patients with C5-C6 root avulsion treated by transfer of ~10% of the ulnar nerve to the biceps motor branch
- Restored elbow flexion without significant impairment of hand function
- Introduced distal nerve transfer as a paradigm for brachial plexus reconstruction
Conduit vs Microsurgical Repair (RCT)
- Randomized prospective trial of 30 median or ulnar nerve injuries in the distal forearm, 5-year follow-up
- Silicone tube repair was at least as good as conventional microsurgical suture for sensory and motor recovery
- Cold intolerance was significantly less severe in the tubular repair group
Sensory Re-education
- Reviewed published sensory re-education programmes after nerve suture
- More patients reached the highest level of recovery (S4) with structured re-education
- Time to peak recovery shortened (≈2 years versus ≈5 years without re-education)
Autograft vs Allograft vs Conduit (Meta-analysis)
- 35 studies, 1559 nerve gap repairs (5-70 mm), PRISMA meta-analysis
- Meaningful recovery comparable for autograft and allograft regardless of gap or nerve type
- Conduits inferior for short sensory gaps (62% MR versus autograft 82% and allograft 87%)
Processed Nerve Allograft Registry (RANGER)
- Largest peripheral nerve registry: 385 subjects, 624 processed nerve allograft repairs
- 82% meaningful recovery across sensory, mixed and motor repairs for gaps up to 70 mm
- Recovery fell with longer gaps (91% for under 15 mm versus 69% for 50-70 mm)
Digital Nerve Repair (Updated Meta-analysis)
- 15 studies, 625 digital nerve repairs analysed for sensory outcome
- Autograft was statistically superior on static two-point discrimination
- Both autograft and allograft outperformed conduit repair when a gap was present
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Gap
"You are exploring a cut median nerve at the wrist. The ends are retracted. You cannot approximate them without flexing the wrist 45 degrees. What do you do?"
Scenario 2: The Old Injury
"A patient presents 18 months after a laceration to the Ulnar nerve at the forearm. They have no sensation and no intrinsics (Claw hand). They want surgery."
Scenario 3: The Neuroma
"A patient has a painful stump neuroma after a digital nerve injury. It's Tinel positive."
MCQ Practice Points
Biology
Q: At what rate does a nerve regenerate? A: Approximately 1mm per day (or 1 inch per month).
Technique
Q: What is the maximum gap suitable for a nerve conduit in a digital nerve? A: Generally accepted as less than 2cm (some say 3cm maximum).
Prognosis
Q: What is the most significant predictor of poor outcome in adults? A: Increasing Age (especially greater than 60).
Anatomy
Q: Which structure guides the regenerating axon? A: The Basal Lamina of the Schwann Cell (Bands of Bungner).
Timing
Q: What is the critical time limit for motor recovery after nerve injury? A: 12-18 months - after this time, motor end plates undergo irreversible fibrosis and atrophy, so muscle recovery is not possible.
Guidelines, Registries & Global Practice
Global Epidemiology
- Peripheral nerve injury complicates an estimated 2-3% of trauma admissions and a higher proportion of upper-limb lacerations.
- The upper limb dominates: digital, median and ulnar nerves account for the majority of repaired civilian injuries, most commonly from glass, knife and power-tool lacerations in young working-age men.
- Lower-limb and high-energy plexus injuries are less common but carry a far worse prognosis and a heavier disability and economic burden.
- In conflict and high-energy settings, blast and gunshot mechanisms shift the pattern toward longer gaps, contamination and delayed reconstruction.
Side-by-Side Guidance
There is no single randomized "level 1" guideline mandating one repair method; practice is driven by surgical principle plus society/consensus statements. Where bodies differ, it is mainly in emphasis.
| Theme | BOA / BSSH (UK) | AAOS / ASSH (US) | AO / consensus (Europe) |
|---|---|---|---|
| Open injury + deficit | Early exploration and repair | Early exploration and repair | Early exploration and repair |
| Closed injury | Observe 3 months, then re-image/EMG | Observe with serial exam/EMG | Observe; baseline EMG at 3-4 weeks |
| Gap management | Tension-free graft preferred for true gaps | Autograft gold standard; allograft accepted | Tension-free coaptation; graft if any tension |
| Conduits | Short (under 2-3 cm) small sensory gaps only | Short sensory gaps only | Short sensory gaps only |
| Nerve transfers | Strongly endorsed for proximal/plexus injury | Strongly endorsed; expanding indications | Endorsed for proximal injury |
The shared, exam-critical message across all bodies: tension-free coaptation, the biological clock for motor end plates, and early exploration of open injuries with a deficit.
Registries & Evidence Sources
- RANGER registry (processed nerve allograft): the largest peripheral nerve outcome dataset, reporting ~82% meaningful recovery for gaps up to 70 mm.
- Unlike arthroplasty, there is no global implant survivorship registry for nerve repair; evidence comes from trials, meta-analyses and the allograft registry rather than national joint-style registries.
High-Resource vs Limited-Resource Practice
| Resource setting | Typical reality |
|---|---|
| High-resource | Microscope, dedicated hand units, processed allograft and conduits available, early hand therapy, nerve transfers offered |
| Limited-resource | Loupe magnification, autograft preferred (low cost, no supply chain), delayed presentation common, therapy access limited |
In limited-resource settings, autograft remains the workhorse because it needs no commercial supply chain; conduits and processed allografts are cost- and availability-limited. Delayed presentation makes the 12-18 month motor window a frequent reason for primary tendon transfer rather than nerve reconstruction.
Clinical summary
Principles
- •Tension-Free Repair
- •Clean Preparation
- •Microsurgical alignment
- •Early protected motion
Timing
- •Primary: Less than 48 hours - best outcomes, clean wounds
- •Delayed: 2-3 weeks - contaminated/crushed injuries
- •Secondary: Greater than 3 months - if recovery plateau
- •Nerve regeneration rate: 1mm/day (1 inch/month)
- •Advanced Tinel sign indicates regeneration progress
Options
- •1. Primary Repair
- •2. Nerve Conduit (Gap less than 2cm)
- •3. Nerve Autograft (Gap greater than 2cm)
- •4. Nerve Transfer