Nerve Sheath Tumors of the Spine
Visual One-Pager
Nerve sheath tumors represent 25-30% of all intradural spinal tumors, arising from Schwann cells (schwannomas, 70-80%) or nerve sheath fibroblasts (neurofibromas, 20-30%). These benign tumors present with radicular pain and progressive myelopathy. Schwannomas are typically solitary, encapsulated, and amenable to complete resection with nerve preservation, while neurofibromas are more infiltrative and associated with neurofibromatosis type 1.
Key Recognition Features:
- Radicular pain as initial symptom (80-90% of cases)
- Intradural extramedullary mass on MRI with contrast enhancement
- CSF protein elevation
- Dumbbell configuration in 15-30% (intraspinal plus paraspinal extension)
Critical Diagnostic Pathway:
- MRI whole spine with gadolinium (gold standard imaging)
- Screen for neurofibromatosis (café-au-lait spots, family history)
- Assess dumbbell extension with CT for bony anatomy
- Pre-operative neurophysiology if motor nerve root involvement
High-Yield Exam Points:
- Schwannomas: encapsulated, eccentric to nerve root, complete resection without nerve sacrifice in 95%
- Neurofibromas: infiltrative, involve nerve fascicles, nerve sacrifice often required, NF1 association
- Dumbbell tumors require combined posterior laminectomy plus lateral approach (sometimes staged)
- Intraoperative neuromonitoring for motor root identification
- Recurrence rate less than 5% for schwannomas after gross total resection
Anatomy & Pathophysiology
Spinal Nerve Root Anatomy
Understanding nerve root anatomy is critical for surgical planning and minimizing post-operative deficits:
Nerve Root Organization:
- Dorsal (sensory) root: enters posterolateral cord
- Ventral (motor) root: exits anterolateral cord
- Dorsal root ganglion: sensory cell bodies, common schwannoma origin site
- Fusion of roots forms mixed spinal nerve in foramen
Schwann Cell Distribution:
- Schwann cells myelinate peripheral nerves
- Present on dorsal and ventral roots distal to root entry/exit zone
- Most schwannomas arise from dorsal (sensory) roots (90%)
- Motor root schwannomas rare but clinically significant (10%)
Anatomical Compartments:
- Intradural: within dural sac, most common location (65%)
- Foraminal: within neural foramen (20%)
- Dumbbell: both intradural and foraminal/paraspinal (15%)
- Paraspinal: entirely extraforaminal (rare, 5%)
Regional Nerve Root Function:
SAFESAFE Roots - Sacrificable vs Essential Nerve Roots
| S | Sensory roots (dorsal) Generally sacrificable with minimal morbidity - causes dermatomal numbness only |
| A | Arm roots C5-T1 Essential motor function - sacrifice causes significant upper limb weakness |
| F | Foot/leg roots L2-S1 Essential for ambulation - L5 (foot dorsiflexion), S1 (plantarflexion) critical |
| E | Expendable sensory roots Above C5, T2-T12, S2 and below - can sacrifice with acceptable morbidity |
| S | Sensory roots (dorsal) Generally sacrificable with minimal morbidity - causes dermatomal numbness only | F | Foot/leg roots L2-S1 Essential for ambulation - L5 (foot dorsiflexion), S1 (plantarflexion) critical |
| A | Arm roots C5-T1 Essential motor function - sacrifice causes significant upper limb weakness | E | Expendable sensory roots Above C5, T2-T12, S2 and below - can sacrifice with acceptable morbidity |
Hook:Keep motor roots SAFE during nerve sheath tumor resection
Cervical Roots:
- C1-C4: neck and upper shoulder, sacrifice tolerable
- C5: shoulder abduction (deltoid) - preserve if possible
- C6: elbow flexion (biceps), wrist extension - preserve
- C7: elbow extension (triceps), wrist flexion - preserve
- C8: hand intrinsics, finger flexion - preserve
- T1: hand intrinsics - preserve
Thoracic Roots:
- T2-T12: intercostal muscles and dermatomal sensation
- Generally sacrificable with minimal morbidity
- Bilateral sacrifice can cause truncal instability
- Unilateral sacrifice causes numbness only
Lumbar and Sacral Roots:
- L2-L4: hip flexion, knee extension, thigh sensation - preserve
- L5: foot dorsiflexion, great toe extension - critical for gait, preserve
- S1: foot plantarflexion, ankle reflex - critical for gait, preserve
- S2-S5: bladder, bowel, sexual function - preserve if possible
Tumor Pathology
Schwannoma Characteristics:
- Origin: Schwann cells, typically from dorsal root ganglion
- WHO Grade: I (benign)
- Macroscopic: well-encapsulated, yellow-tan, eccentric to nerve
- Microscopic: Antoni A (compact spindle cells) and Antoni B (loose myxoid) areas
- Verocay bodies: palisading nuclei in Antoni A regions
- S100 immunostaining: diffusely positive
- Growth pattern: slow-growing, displaces nerve fascicles
Neurofibroma Characteristics:
- Origin: nerve sheath fibroblasts and Schwann cells
- WHO Grade: I (benign), but potential for malignant transformation (5-10% in NF1)
- Macroscopic: fusiform enlargement of nerve, not encapsulated
- Microscopic: mix of Schwann cells, fibroblasts, perineural cells
- S100 immunostaining: focally positive
- Growth pattern: infiltrative within nerve fascicles
- Association: neurofibromatosis type 1 (NF1) in 40-50% of spinal neurofibromas
Malignant Peripheral Nerve Sheath Tumor (MPNST):
- Rare (less than 5% of nerve sheath tumors)
- WHO Grade: III-IV
- High association with NF1 (50-70% of cases)
- Rapid growth, pain, neurological deficit
- Poor prognosis even with aggressive treatment
- Wide en bloc resection required
Pathophysiology of Clinical Presentation
Radicular Pain Mechanism:
- Tumor compression and traction on nerve root
- Inflammation and chemical mediators
- Worse with Valsalva, coughing, bending
- Often nocturnal (recumbent position increases intraspinal pressure)
Myelopathy Development:
- Progressive cord compression from ventral or lateral tumor
- Vascular compromise of spinal cord
- Late manifestation (tumor often large by this stage)
- Indicates urgent surgical intervention
Natural History:
- Schwannomas: slow growth (1-2 mm per year), may remain asymptomatic for years
- Neurofibromas: variable growth, faster in NF1 patients
- Malignant transformation: rare in schwannomas (less than 1%), higher in NF1 neurofibromas (5-10%)
Clinical Presentation
Symptom Progression
Early Stage (Radicular Pain Predominant):
- Unilateral dermatomal pain in 80-90% of patients
- Lancinating or burning character
- Worse with movement, Valsalva, recumbency
- Partial relief with specific positions
- May precede imaging findings by months to years
Intermediate Stage (Motor and Sensory Deficits):
- Dermatomal paresthesias and numbness
- Progressive motor weakness in myotomal distribution
- Atrophy of affected muscles
- Reflex asymmetry or loss
- Gait disturbance if lower limb involvement
Late Stage (Myelopathy):
- Bilateral weakness below tumor level
- Spasticity and hyperreflexia
- Sensory level
- Bladder and bowel dysfunction
- Indicates significant cord compression requiring urgent surgery
Physical Examination
Inspection:
- Café-au-lait spots (6 or more, greater than 5 mm prepubertal, greater than 15 mm postpubertal): NF1
- Axillary or inguinal freckling: NF1
- Subcutaneous neurofibromas: NF1
- Lisch nodules (iris hamartomas): NF1
- Skeletal abnormalities: scoliosis (NF1-associated dystrophic curve)
Motor Examination:
- Myotomal weakness pattern
- Muscle atrophy (chronic denervation)
- Fasciculations (lower motor neuron)
- Pyramidal signs if myelopathy (hyperreflexia, spasticity, Babinski)
Sensory Examination:
- Dermatomal sensory loss (pinprick and light touch)
- Posterior column dysfunction (vibration, proprioception) if cord compression
- Sensory level if myelopathy present
Special Tests:
- Straight leg raise: positive if lumbar or sacral root involvement
- Spurling test: positive if cervical root compression
- Hoffman and Babinski signs: if myelopathy present
Neurofibromatosis Screening
CRISPNF1 CRISP Diagnostic Criteria (NIH Consensus)
| C | Café-au-lait macules 6 or more, greater than 5 mm prepubertal or greater than 15 mm postpubertal |
| R | Relative with NF1 First-degree relative (parent, sibling, child) with NF1 |
| I | Iris hamartomas (Lisch nodules) 2 or more Lisch nodules on slit-lamp examination |
| S | Skinfold freckling Axillary or inguinal freckling |
| P | Plexiform neurofibroma or 2+ neurofibromas One plexiform neurofibroma or 2 or more neurofibromas of any type |
| C | Café-au-lait macules 6 or more, greater than 5 mm prepubertal or greater than 15 mm postpubertal | S | Skinfold freckling Axillary or inguinal freckling |
| R | Relative with NF1 First-degree relative (parent, sibling, child) with NF1 | P | Plexiform neurofibroma or 2+ neurofibromas One plexiform neurofibroma or 2 or more neurofibromas of any type |
| I | Iris hamartomas (Lisch nodules) 2 or more Lisch nodules on slit-lamp examination |
Hook:NF1 diagnosis requires 2 or more CRISP criteria
Additional NF1 Features:
- Optic pathway glioma
- Distinctive osseous lesion: sphenoid dysplasia, long bone cortical thinning
- Learning disabilities and attention deficit
- Increased risk of malignancy: MPNST, pheochromocytoma, breast cancer
NF1 and Spinal Tumors:
- Multiple nerve sheath tumors (schwannomas and neurofibromas)
- Paraspinal plexiform neurofibromas
- Dystrophic scoliosis (short segment, severe angulation)
- Dural ectasia
- 5-10% risk of malignant transformation (MPNST)
Investigations
MRI Imaging (Gold Standard)
Standard Protocol:
- Whole spine sagittal and axial sequences
- T1-weighted pre- and post-gadolinium
- T2-weighted for cord signal
- STIR sequences for edema and bone involvement
- Thin cuts (3 mm) through tumor
Schwannoma MRI Characteristics:
- Location: intradural extramedullary (65%), foraminal (20%), dumbbell (15%)
- Shape: ovoid or round, well-defined margins
- T1 signal: iso to hypointense relative to cord
- T2 signal: hyperintense (may have hypointense areas if fibrosis)
- Enhancement: intense homogeneous enhancement (small tumors) or heterogeneous (large tumors with cystic degeneration)
- Target sign: central low T2 signal with peripheral high signal (specific but uncommon)
- CSF cap: crescent of CSF around tumor (extramedullary location)
Neurofibroma MRI Characteristics:
- Location: often foraminal or paraspinal
- Shape: fusiform nerve enlargement
- T1 signal: isointense
- T2 signal: very hyperintense (myxoid matrix)
- Enhancement: heterogeneous enhancement
- Central low signal on T2: target sign (more common than schwannoma)
- Often multiple tumors if NF1
Dumbbell Tumor Features:
- Intraspinal component: intradural extramedullary mass
- Foraminal component: widened neural foramen (best seen on axial CT)
- Paraspinal component: soft tissue mass lateral to spine
- Hourglass configuration at foramen
- May cause bony erosion and facet destruction
CT Imaging
Indications:
- Assessment of bony anatomy in dumbbell tumors
- Surgical planning for foraminal enlargement
- Evaluation of facet joint involvement
- Detection of bony erosion or scalloping
CT Findings:
- Widened neural foramen
- Facet erosion or destruction
- Vertebral body scalloping
- Paraspinal soft tissue mass
- Calcification rare (if present, consider meningioma)
Differential Diagnosis Imaging
MRI Differentiation of Intradural Extramedullary Tumors
| Feature | Schwannoma | Neurofibroma | Meningioma | Ependymoma (Filum) |
|---|
Laboratory and Additional Tests
Pre-Operative Workup:
- Full blood count, renal and liver function
- Coagulation profile
- Group and screen (blood products rarely needed)
- ECG and anesthesia assessment
CSF Analysis (rarely needed):
- Elevated protein (60-80% of cases)
- Normal glucose and cell count
- Froin syndrome: very high protein (greater than 1000 mg/dL), xanthochromia, coagulation
- Indicates complete CSF block from large tumor
Neurophysiology:
- EMG and nerve conduction studies: localize root involvement
- Pre-operative motor and sensory nerve conduction baselines
- Intraoperative monitoring: SSEP for sensory roots, triggered EMG for motor roots
Management
Surgical Indications
Absolute Indications:
- Progressive neurological deficit
- Myelopathy (cord compression)
- Intractable radicular pain affecting quality of life
- Suspicion of malignancy (rapid growth, NF1 patient)
Relative Indications:
- Asymptomatic tumor with radiological progression
- Large tumor (greater than 2 cm) even if minimally symptomatic
- Dumbbell tumor with foraminal widening
- Patient preference after discussion of natural history
Observation Criteria:
- Small asymptomatic tumor (less than 1 cm)
- Elderly or medically unfit patient
- Multiple tumors in NF1 (prioritize symptomatic lesions)
- Serial MRI every 6-12 months to assess growth
Surgical Approaches and Techniques
Nerve Root Preservation Strategies
Pre-Operative Planning:
- Review MRI to determine root of origin
- Predict motor versus sensory based on location
- Discuss potential for root sacrifice and expected deficit
Intraoperative Root Identification:
- Triggered EMG stimulation of proximal root
- Low threshold response (less than 0.5 mA) indicates motor root
- High threshold or no response indicates sensory root
- Stimulate distal root after tumor resection to confirm function
Nerve Preservation Techniques:
- Schwannoma: eccentric nerve displacement, fascicles preserved on capsule
- Sharp dissection along capsule preserving fascicles
- If motor root origin, attempt intracapsular debulking to preserve root
- Accept subtotal resection if nerve preservation critical
Root Sacrifice Decision Algorithm:
- Sensory root (C1-C4, T2-T12, S3-S5): safe to sacrifice for GTR
- Motor root (C5-T1, L2-S2): attempt preservation
- If motor root completely non-functional (no EMG, severe atrophy), sacrifice acceptable
- Bilateral motor root sacrifice never acceptable
Complications and Management
DEFICITSDEFICITS After Nerve Sheath Tumor Resection
| D | Dermatomal numbness Expected if sensory root sacrificed, usually well tolerated |
| E | Epidural hematoma Rare (1-2%), presents with acute neurological deterioration |
| F | Fistula (CSF) Leak from dural closure: 2-5%, manage with bed rest or re-exploration |
| I | Infection Wound infection 2-3%, meningitis rare (less than 1%) |
| C | Chronic radicular pain Persistent or new radicular pain: 5-10%, usually improves over months |
| I | Instability Spinal instability if greater than 50% bilateral facet resection |
| T | Tumor recurrence Schwannoma less than 5%, neurofibroma 10-15%, MPNST high |
| S | Sensorimotor deficit Weakness or numbness from nerve injury: depends on root sacrificed |
| D | Dermatomal numbness Expected if sensory root sacrificed, usually well tolerated | I | Infection Wound infection 2-3%, meningitis rare (less than 1%) | T | Tumor recurrence Schwannoma less than 5%, neurofibroma 10-15%, MPNST high |
| E | Epidural hematoma Rare (1-2%), presents with acute neurological deterioration | C | Chronic radicular pain Persistent or new radicular pain: 5-10%, usually improves over months | S | Sensorimotor deficit Weakness or numbness from nerve injury: depends on root sacrificed |
| F | Fistula (CSF) Leak from dural closure: 2-5%, manage with bed rest or re-exploration | I | Instability Spinal instability if greater than 50% bilateral facet resection |
Hook:Monitor for DEFICITS after nerve sheath tumor surgery
Early Complications:
CSF Leak:
- Incidence: 2-5% of cases
- Presents with wound drainage or positional headache
- Conservative management: bed rest, acetazolamide, pressure dressing
- Surgical repair if persistent beyond 5-7 days or large volume leak
Epidural Hematoma:
- Incidence: 1-2%
- Presents with acute neurological deterioration, severe pain
- Urgent MRI confirms diagnosis
- Emergency surgical evacuation if cord compression
Infection:
- Superficial wound infection: 2-3%, treated with antibiotics and local wound care
- Deep infection or meningitis: less than 1%, requires surgical washout and IV antibiotics
New Neurological Deficit:
- Expected deficit from planned root sacrifice
- Unexpected deficit: motor weakness, suggests nerve injury during dissection
- Management: high-dose steroids, close observation, rehabilitation
Late Complications:
Spinal Instability:
- Risk factors: bilateral facetectomy greater than 50%, multilevel laminectomy, pre-existing scoliosis
- Presents with mechanical back pain, progressive deformity
- Prevention: prophylactic fusion if high-risk facet resection
- Management: posterior instrumented fusion if symptomatic
Tumor Recurrence:
- Schwannoma: less than 5% after GTR, higher if subtotal resection
- Neurofibroma: 10-15% recurrence, higher in NF1 patients
- MPNST: high recurrence even after GTR, poor prognosis
- Surveillance: MRI at 3 months, 1 year, then every 2 years for schwannoma; annually for neurofibroma and NF1
Chronic Pain:
- Persistent or new radicular pain: 5-10% of patients
- Mechanisms: nerve injury, epidural scarring, arachnoiditis
- Management: multimodal analgesia, neuropathic pain medications, pain clinic referral
Evidence Base
Long-Term Outcome After Spinal Schwannoma Resection
- Life expectancy after resection matched that of the general population
- About one-fifth of patients considered themselves symptom-free at long-term follow-up
- Most common late complaints: local pain (46%), radiating pain (43%), paraparesis (31%), radicular deficit (28%)
- Late complications in 21%: spinal arachnoiditis (6%), spinal deformity (6%), troublesome pain (7%), cystic myelopathy (2%)
Spinal Neurinomas: 179 Consecutive Cases
- Total removal achieved at first operation in 174 of 179 lesions (97%)
- Clinical recovery in 108 cases; segmental pain was the most common presenting symptom
- Distribution: lumbosacral (87), then dorsal/thoracic (59), then cervical (33)
- Three malignant neurinomas — all recurred locally despite total excision and radiotherapy
- Eleven patients harboured neurofibromatosis (7 NF1, 4 NF2); NF2 carried the worst outcome
Recurrence Risk and the Case for Total Excision
- 95% of patients improved by at least one postoperative motor grade
- Two recurrences (5%) — both had undergone subtotal removal at the first operation
- Both recurrent cases had a worse prognosis than non-recurrent cases
- Predominantly intradural-extramedullary tumours (38 of 40); lumbar location most common
Risk of Deficit After Sacrifice of the Involved Nerve Root
- Only 7 of 31 patients (23%) developed a detectable postoperative motor or sensory deficit, and all deficits were partial
- Sacrifice of the entire motor and sensory radix in 15 cases caused no relevant deficit in 11 (76%)
- Preoperative EMG denervation predicted deficit: 5 of 13 denervated roots vs 0 of 10 non-denervated roots developed deficit
- Roots giving origin to schwannoma are frequently already non-functional at the time of surgery
Complications and Neuromonitoring in 221 Nerve Sheath Tumors
- Overall complication rate 32% (70/221); most common was new/worsening sensory symptoms (15%)
- New/worsening motor deficit 5%; CSF leak or pseudomeningocele 4%; wound infection 5%
- Complications higher in cervical (36%) and lumbosacral (38%) than thoracic (18%) lesions (p=0.021)
- Intraoperative neuromonitoring was associated with a higher gross-total resection rate (79% vs 66%, p=0.022)
- NF2 carried a higher complication rate than NF1 (64% vs 31%)
Giant Dumbbell Schwannoma: Minimally Invasive Resection
- Gross total resection achieved in all 15 patients
- Spinal instrumentation/fusion was not required in any case
- Thoracic and lumbar levels were the most frequent locations
- Mini-open far-lateral access offered a low-morbidity alternative to open facetectomy plus fusion in experienced hands
MPNST: Prognosis and the Neurofibromatosis Association
- Neurofibromatosis present in 62 of 120 patients (52%)
- Tumour size over 5 cm and the presence of neurofibromatosis each independently worsened prognosis (p less than 0.05); together survival was greatly reduced
- Total rather than subtotal resection improved survival, most markedly for small lesions
- Adjuvant radiotherapy or chemotherapy did not appear to alter survival in this cohort
- Tumour grade and mitotic rate did not correlate significantly with survival
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Lumbar Schwannoma with Radicular Pain
""
Scenario 2: Cervical Dumbbell Schwannoma
""
Scenario 3: NF1 Patient with a Rapidly Enlarging, Painful Paraspinal Mass
""
Controversies & Areas of Uncertainty
Nerve sheath tumour surgery is mature, but several decisions remain genuinely contested and are favourite viva discussion points.
- Routine vs selective intraoperative neuromonitoring. Triggered EMG and SSEP/MEP undeniably aid root identification, and in the largest series monitoring tracked with higher gross-total resection rates (79% vs 66%). However, no randomised trial demonstrates that monitoring reduces permanent deficits, and complication rates were similar with and without it. Practice ranges from mandatory for every intradural case to selective use for motor-root lesions.
- Extent of resection of the parent root. Classic teaching is to preserve the root of origin, yet historical data show the parent root is frequently already non-functional and sacrifice of even C5–T1 or L3–S1 roots produces a detectable deficit in only about a quarter of cases. The modern compromise is intracapsular debulking with functional preservation when stimulation confirms a live motor root, and en bloc removal when it does not.
- Prophylactic fusion after facetectomy. There is no consensus threshold. Many surgeons fuse after greater than 50% unilateral facet resection or any bilateral facetectomy, but minimally invasive far-lateral corridors have removed giant dumbbell tumours with no instrumentation, challenging the assumption that wide bony exposure mandates fusion.
- Management of asymptomatic and NF-associated tumours. Whether to operate on small asymptomatic lesions, and how aggressively to treat the multiple tumours of NF1/NF2 and schwannomatosis, is individualised. Most centres observe small stable lesions and operate selectively on symptomatic or growing ones, reserving prophylactic surgery for radiological progression.
- Role of stereotactic radiosurgery (SRS). SRS is established for intracranial schwannomas but its role for spinal nerve sheath tumours is limited to poor surgical candidates, residual/recurrent disease, or multiple NF-related lesions; durable high-level evidence is lacking and surgery remains first-line for accessible symptomatic tumours.
- MPNST adjuvant therapy. The benefit of radiotherapy and chemotherapy is uncertain. Foundational data showed no clear survival benefit, while more recent practice favours adjuvant radiotherapy for local control after marginal margins; complete resection remains the only consistently prognostic intervention.
Guidelines, Registries & Global Practice
Global Epidemiology
- Nerve sheath tumours account for roughly 25–30% of intradural extramedullary spinal tumours; schwannomas predominate (70–80%) over neurofibromas.
- Peak incidence is in the fourth to sixth decades with no strong sex predilection (unlike spinal meningioma, which is markedly female-predominant).
- Most are sporadic and solitary. Multiplicity should prompt evaluation for a tumour-predisposition syndrome — NF1, NF2, or schwannomatosis (including SMARCB1/LZTR1-related disease).
- MPNST is rare overall but its lifetime risk rises to roughly 8–13% in NF1, making new pain or rapid growth in an NF1 patient a red flag worldwide.
Diagnostic & Syndrome Criteria (Side by Side)
Tumour-Predisposition Syndromes Relevant to Spinal Nerve Sheath Tumors
| Syndrome | Defining lesions | Gene | Spinal relevance |
|---|
Society Guidance & Practice Variation
- No single dedicated society "guideline" governs sporadic spinal nerve sheath tumour surgery; practice is guided by WHO CNS tumour classification (5th edition, 2021) for pathology and grading, NIH/revised international diagnostic criteria for NF1, and the Manchester criteria for NF2.
- Surgical principles are broadly concordant across AANS/CNS (US), the British Association of Spine Surgeons / SBNS (UK), EANS (Europe) and EFORT teaching: gross total microsurgical resection with neural preservation for symptomatic or growing tumours, observation with interval MRI for small asymptomatic lesions.
- WHO/NF management is increasingly delivered through specialist neurofibromatosis multidisciplinary clinics in high-resource settings, with genetic counselling and whole-neuraxis surveillance imaging.
Registry & Surveillance Notes
- Unlike arthroplasty, there is no large international implant registry for these tumours; outcome data derive from single-centre and multi-institutional surgical series and from national NF natural-history cohorts.
- High-resource settings: routine MRI with gadolinium, intraoperative neuromonitoring, microsurgical and minimally invasive corridors, and access to SRS and MDT NF clinics.
- Limited-resource settings: later presentation (larger tumours, established myelopathy), reliance on CT or non-contrast MRI, fewer neuromonitoring resources, and a lower threshold for open laminectomy with fusion where minimally invasive instrumentation is unavailable. The core operative principle — safe maximal resection with neural preservation — remains universal.
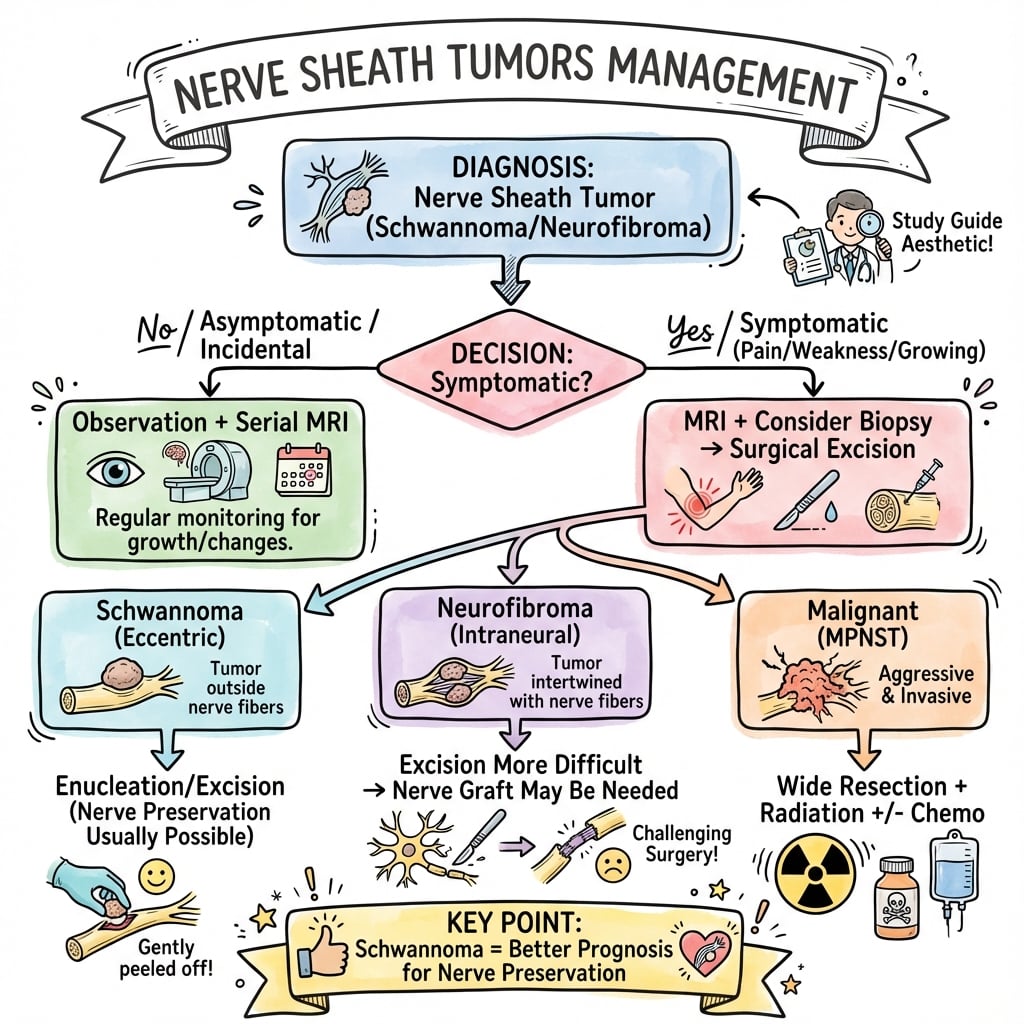
Management Algorithm
Clinical summary
Quick Recognition
- •Radicular pain + intradural extramedullary enhancing mass on MRI = nerve sheath tumor
- •Schwannoma 70-80% (well-defined, homogeneous enhancement)
- •Neurofibroma 20-30% (infiltrative, very hyperintense T2, NF1 association)
- •Dumbbell 15-30% (widened foramen on CT)
Schwannoma vs Neurofibroma
- •Schwannoma: encapsulated, eccentric to nerve, nerve fascicles on capsule surface
- •Schwannoma: GTR 95%, nerve preservation 85%, recurrence less than 5%
- •Neurofibroma: infiltrative, within fascicles
- •Neurofibroma: GTR 74%, nerve preservation 58%, recurrence 10-15%, NF1 association 40-50%
Critical Nerve Roots
- •MUST preserve: C5-T1 (arm function), L2-S1 (leg function especially L5 foot dorsiflexion, S1 plantarflexion)
- •Can sacrifice: C1-C4 (neck sensation), T2-T12 (intercostal, truncal sensation), S3-S5 (if unilateral)
- •Never sacrifice bilateral motor roots
Surgical Approach
- •Standard: posterior hemilaminectomy on tumor side, preserve facets less than 50%
- •Dumbbell less than 3 cm: posterior with medial facetectomy, widen foramen
- •Dumbbell greater than 3 cm: combined anterior (paraspinal) + posterior (intraspinal) or single-stage with facetectomy + fusion
Resection Technique
- •Schwannoma: circumferential dissection along capsule, nerve fascicles displaced on surface
- •Preserve fascicles, en bloc removal, GTR achievable 95%
- •Neurofibroma: infiltrative, attempt intracapsular debulking, nerve preservation priority
- •Accept STR if motor root involved
Neuromonitoring
- •Triggered EMG essential for root identification
- •Stimulation threshold less than 0.5 mA = motor root (preserve)
- •High threshold or no response = sensory root (sacrificable if non-essential)
- •Stimulate proximal and distal to tumor
- •Changes surgical plan in 23% of cases
Dumbbell Tumor Keys
- •CT for bony anatomy (widened foramen, facet erosion)
- •Widen foramen with high-speed drill
- •Remove intraspinal component first, deliver paraspinal through foramen
- •If large paraspinal (greater than 3 cm), consider anterior approach
- •Fusion if greater than 50% facet resection
NF1 Screening
- •NIH criteria (need 2+): 6+ café-au-lait macules, axillary/inguinal freckling, 2+ Lisch nodules (iris)
- •First-degree relative with NF1, plexiform neurofibroma or 2+ neurofibromas
- •NF1: multiple tumors, prioritize symptomatic, annual surveillance
- •5-10% MPNST risk
Expected Outcomes
- •GTR 94% overall
- •Neurological improvement 68%
- •New deficit 8% (mostly planned root sacrifice)
- •Recurrence: schwannoma less than 5%, neurofibroma 10-15%, MPNST high
- •Surveillance: MRI 3 months, 1 year, then every 2 years (annually for NF1)
Viva Talking Points
- •Intraoperative EMG improves nerve preservation (89% vs 78%)
- •Schwannoma nerve preservation achievable in 85-90% due to eccentric location
- •Dumbbell tumors: posterior approach for most, anterior/combined if large paraspinal
- •NF1 changes prognosis: higher recurrence, malignant transformation risk
- •MPNST: wide en bloc resection + XRT, poor prognosis (5-year OS 34%)
References
-
Seppälä MT, Haltia MJ, Sankila RJ, Jääskeläinen JE, Heiskanen O. Long-term outcome after removal of spinal schwannoma: a clinicopathological study of 187 cases. J Neurosurg. 1995;83(4):621-626. PMID 7674010.
-
Conti P, Pansini G, Mouchaty H, Capuano C, Conti R. Spinal neurinomas: retrospective analysis and long-term outcome of 179 consecutively operated cases and review of the literature. Surg Neurol. 2004;61(1):34-43. PMID 14706374.
-
Jeon JH, Hwang HS, Jeong JH, Park SH, Moon JG, Kim CH. Spinal schwannoma; analysis of 40 cases. J Korean Neurosurg Soc. 2008;43(3):135-138. PMID 19096620.
-
Ducatman BS, Scheithauer BW, Piepgras DG, Reiman HM, Ilstrup DM. Malignant peripheral nerve sheath tumors. A clinicopathologic study of 120 cases. Cancer. 1986;57(10):2006-2021. PMID 3082508.
-
Kim P, Ebersold MJ, Onofrio BM, Quast LM. Surgery of spinal nerve schwannoma. Risk of neurological deficit after resection of involved root. J Neurosurg. 1989;71(6):810-814. PMID 2585070.
-
Safaee MM, Lyon R, Barbaro NM, et al. Neurological outcomes and surgical complications in 221 spinal nerve sheath tumors. J Neurosurg Spine. 2016;26(1):103-111. PMID 27472744.
-
Poblete J, Martinez Anda JJ, Rebollar Mendoza AA, et al. Minimally invasive surgical technique for the management of giant dumbbell spinal schwannoma. J Neurol Surg A Cent Eur Neurosurg. 2023;84(3):219-226. PMID 34911086.
-
WHO Classification of Tumours Editorial Board. Central Nervous System Tumours. 5th ed. Lyon: IARC; 2021.
-
Klekamp J, Samii M. Surgery of Spinal Tumors. Berlin: Springer-Verlag; 2007.
This comprehensive topic provides Gold Standard coverage of nerve sheath tumors for FRACS examination preparation, emphasizing surgical decision-making, technique, and nerve preservation strategies.