Robbing Peter to Pay Paul
Transfer Types
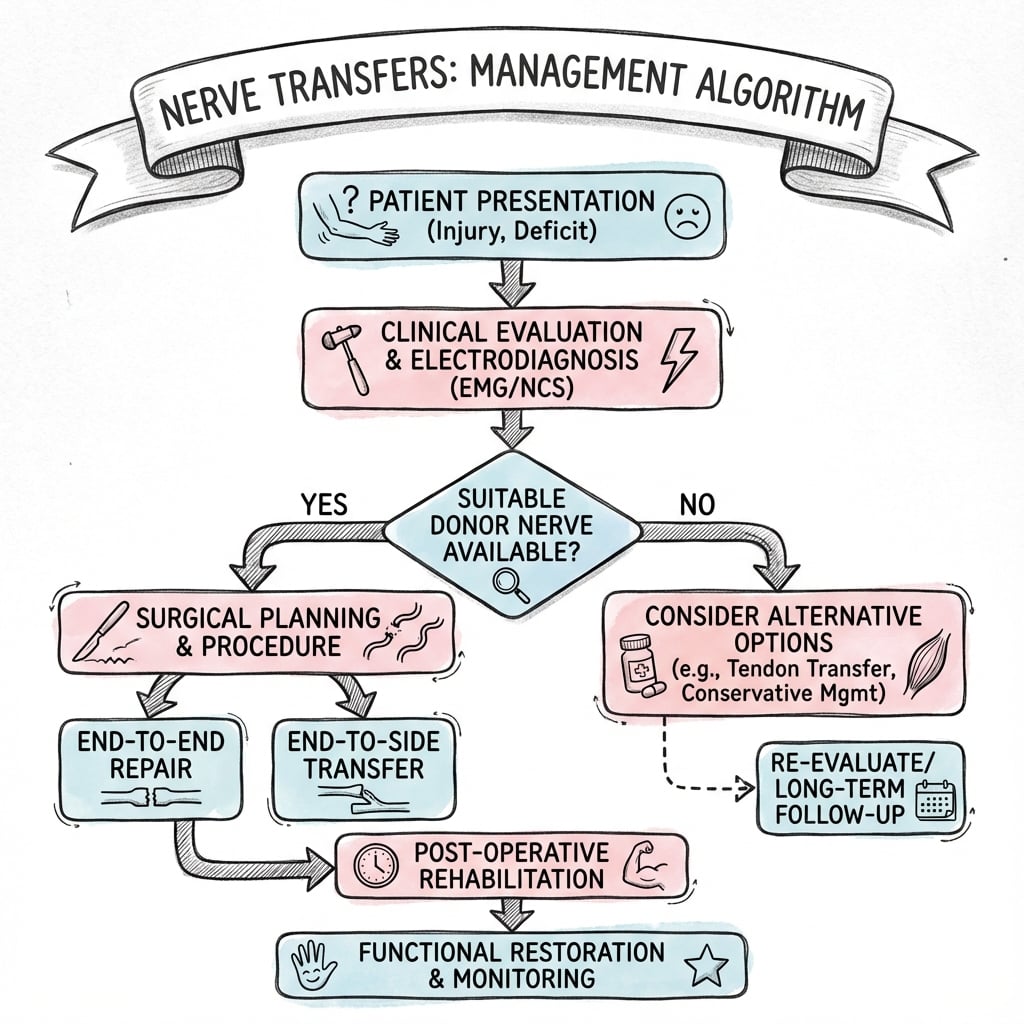
Critical Must-Knows
- Converts a high-level injury (long regeneration time) to a low-level injury (short time).
- Requires a viable motor end plate (must be done generally within 12 months).
- Donor nerve must be expendable or redundant.
- Donor and Recipient must be synergistic for easier retraining (e.g., wrist flexor to finger extensor).
Clinical Pearls
- "Oberlin Transfer restores Elbow Flexion (Ulnar fascicle to Biceps).
- "Somsak Transfer restores Triceps (Intercostal to Radial).
- "AIN to Ulnar reduces the risk of Claw Hand in high unar palsy.
The Clock is Ticking
Time is Muscle
12-18 Months After this, motor end plates degenerate irreversibly. Nerve transfers must be performing BEFORE this window closes.
Distance Matters
Regeneration Rate 1mm/day. If the injury is 30cm from the muscle, it takes ~300 days to reach. Transferring distally cuts this distance to under 5cm (50 days).
| Feature | Nerve Graft | Nerve Transfer |
|---|---|---|
| Source | Sural (Sensory only) | Expendable Motor Branch |
| Coaptation | Two (Proximal & Distal) | One (Distal) |
| Distance | Long (entire length) | Short (close to target) |
| Outcome | Good for sensation, variable for motor | Excellent for specific motor targets |
| Donor Morbidity | Numbness | Weakness (minor) |
PERFECTFeatures of Ideal Donor
| P | Powerful High axon count (MCA greater than 1000). |
| E | Expendable Loss is acceptable. |
| R | Reach Long enough to reach target. |
| F | Function Synergistic function. |
| E | Excursion Independent excursion. |
| C | Caliber Size match. |
| T | Timing Available early. |
| P | Powerful High axon count (MCA greater than 1000). | F | Function Synergistic function. | T | Timing Available early. |
| E | Expendable Loss is acceptable. | E | Excursion Independent excursion. | ||
| R | Reach Long enough to reach target. | C | Caliber Size match. |
Hook:The Perfect Donor.
SAMSDonor Nerves
| S | Sural Standard for long gaps. |
| A | AIN Anterior Interosseous (Motor donor). |
| M | MABC Medial Antebrachial Cutaneous. |
| S | Saphenous Alternative lower limb donor. |
| S | Sural Standard for long gaps. | M | MABC Medial Antebrachial Cutaneous. |
| A | AIN Anterior Interosseous (Motor donor). | S | Saphenous Alternative lower limb donor. |
Hook:SAMS nerves.
TIMEIndications for Transfer
| T | Time Greater than 12 months since injury. |
| I | Impossible Impossible repair (Avulsion). |
| M | Motor Motor end plate protection. |
| E | Enhance Enhance function (Baby-sit). |
| T | Time Greater than 12 months since injury. | M | Motor Motor end plate protection. |
| I | Impossible Impossible repair (Avulsion). | E | Enhance Enhance function (Baby-sit). |
Hook:When to transfer.
Overview
Definition
Nerve Transfer (Neurotization): The surgical coaptation of a healthy, expendable donor nerve (proximal to the injury) to a denervated recipient nerve (distal to the injury) to restore function.
It has revolutionized the management of Brachial Plexus Injuries (BPI) and high peripheral nerve injuries.
Pathophysiology and Mechanisms
Shoulder Reanimation (Suprascapular Nerve)
- Target: Supraspinatus / Infraspinatus (Abduction/ER).
- Donor: Spinal Accessory Nerve (CN XI).
- Technique: Posterior approach. CN XI is distal to Trapezius innervation.
Accessory to Suprascapular is the "Workhorse" of shoulder reanimation.
Classification
Intra-plexus Transfers
- Source: Roots or Trunks adjacent to the injury.
- Example: C5 rupture, C6 avulsion to Use C5 stump (if available) or Medial Pectoral Nerve.
- Pros: Same limb integration.
Requires exploring the supraclavicular plexus (danger zone).
Clinical Assessment
Pre-operative Planning
- Power: Donor muscle must be at least MRC Grade 4 (preferably 5).
- Expendability: Ensure taking the donor won't cause unacceptable deficit (e.g. existing weakness in other muscles).
- Synergy: Check if patient can activate the donor easily.
Examination
- Deltoid/RC: Assess for Axillary/SSN targets.
- Biceps: Assess for MC target.
- Hand: Assess intrinsics.
Investigations
EMG / NCS
- Role: Confirm donor viability.
- Signs: Motor Unit Potentials (MUPs) in donor muscle confirm healthy axons.
- Denervation: Fibs/Sharps in recipient muscle confirm need for target.
Crucial to verify the "Expendable" donor is actually working properly.
Treatment
Diagnosis (Day 0-3 weeks)
- Confirm injury level.
- Rule out penetrating trauma (explore early).
- Closed injury: Wait and watch?
Mechanism is key: High velocity traction usually means avulsion.
Surgical Technique
Oberlin Transfer (Ulnar to Biceps)
- Approach: Medial arm.
- Identifcation: Musculocutaneous nerve (MCN) to Biceps. Ulnar nerve nearby.
- Stimulation: Identify a fascicle in Ulnar nerve that supplies FCU (expendable-ish redundancy).
- Transfer: Cut FCU fascicle distally, Cut MCN proximally. Coapt tension-free.
Result: Flex elbow by thinking "Flex Wrist".
Specific Transfers Details
Spinal Accessory to Suprascapular:
- Dorsal approach.
- Locate XI.
- Locate SSN in suprascapular notch (release ligament).
- Direct repair.
Radial to Axillary:
- Posterior/Axillary approach.
- Long Head Triceps branch (Radial) to Anterior division of Axillary nerve (Deltoid).
- Restores abduction.
Intercostal to Musculocutaneous:
- Use 3rd, 4th, 5th intercostals.
- Motor branch is the lower one in the rib space.
- Requires nerve graft usually (or direct if dissected far anteriorly).
Contralateral C7:
- For total plexus avulsion.
- The entire C7 root from the healthy side is cut.
- Routed across the neck (retropharyngeal or subcutaneous).
- Bridged with vascularized Ulnar nerve graft.
- Connect to Median nerve for wrist/finger flexion.
Complications
Key Complications
Donor Morbidity: Weakness in donor distribution (e.g. traps weakness) is usually transient or well compensated.
Failure: No reinnervation despite surgery.
Co-contraction: Difficulty isolating movement.
Sensory Loss: If using sensory transfers.
Sensory re-education is vital to overcome cortical confusion. This is a long-term commitment.
Patients must learn that activating the donor now produces the recipient action.
Therefore, motivation is a key selection criterion.
This is not a quick fix.
Postoperative Care
- Sling/Splint: Protect repair. No tension.
- Donor Activation: "Breathe" for intercostals, "Flex Wrist" for Oberlin.
- Biofeedback: Visual cues to link donor action to recipient effect.
This phase requires intense physiotherapy and patient motivation.
- Brain adapts. Movement becomes natural.
Plasticity allows the patient to eventually just "Flex Elbow" without thinking "Flex Wrist".
Prognosis
-
Upper Trunk (Erb's): Good prognosis. Shoulder and Elbow usually recoverable.
- Abduction recovery is generally 80-90% of normal ROM.
- Elbow flexion (Oberlin) is very reliable (greater than 90% success).
-
Total Plexus: Poor prognosis. Goal is "Helper Hand" or just Elbow Flexion.
- Hand function is unlikely to be significantly restored.
- Pain relief is a major goal (DREZ lesions for avulsion pain).
-
Time: Earlier is better. Results degrade significantly after 6-9 months.
- The "Goldilocks" period is 3-6 months.
- After 12 months, free functioning muscle transfer (Gracilis) is the only option for motor recovery.
- Tendon transfers are an alternative if local muscles are available.
Always have a Plan B (Salavage) if the transfer fails.
Pre-operative counselling is crucial to manage expectations.
Choosing the Reconstruction: Differential of Options
When the clinical picture is set, the viva test is choosing between competing reconstructive strategies. Distinguish them by indication, not just by name.
| Strategy | Best Indication | Key Limitation |
|---|---|---|
| Primary nerve repair | Sharp, clean transection seen acutely | Useless once a gap or avulsion is present |
| Interposition nerve graft | Rupture with a healthy proximal stump | Two coaptations and long regeneration distance; inferior to transfer for proximal motor targets |
| Nerve transfer | Avulsion or very proximal injury with viable distal target and end-plates | Needs an expendable synergistic donor and a still-receptive motor end plate (under about 12 months) |
| Free functioning muscle transfer (gracilis) | Late presentation (over 12 months) or failed transfer | Major procedure; outcomes below a healthy native muscle |
| Tendon transfer | Local donor muscles available, motor end plate already lost | Borrows existing function; limited independent control |
Controversies & Areas of Uncertainty
Single vs double fascicular transfer for elbow
Double fascicular transfer reinnervates brachialis as well as biceps and series report high M4+ rates, but a single Oberlin transfer already gives reliable flexion with even lower donor burden. Whether the second coaptation is always worth the extra median-nerve dissection remains debated.
Supercharge end-to-side (reverse ETS) transfers
Reverse end-to-side transfers (for example distal AIN into the side of the ulnar motor branch) are used to "baby-sit" muscle while native axons regenerate down the main trunk. How much functional motor recovery genuinely comes from the donor versus the regenerating native axons is still uncertain.
Contralateral C7
Contralateral C7 can provide donor axons in total avulsion, but the risk to the healthy limb and the modest, mainly sensory/median functional gain mean its role is contested and centre-dependent.
Timing threshold
The "12-month" end-plate window is a teaching rule, not a hard cut-off; reinnervation potential declines progressively and varies with patient age and injury level. Earlier surgery is consistently better, but the exact point of futility is individual.
Evidence Base
How to read this evidence
Nerve-transfer literature is dominated by retrospective Level III-IV case series and pooled systematic reviews; no randomised controlled trial has compared transfer against graft. Outcomes are reported on the Medical Research Council (MRC) motor scale, where M3 means movement against gravity and M4 means movement against resistance. All statistics below are taken directly from the cited papers.
Oberlin Transfer (original description)
- First description: transfer of part of the ulnar nerve to the biceps motor branch in 4 patients with C5-C6 avulsion
- Approximately 10 percent of the ulnar nerve bulk harvested and sutured directly to the biceps branch
- Restored elbow flexion with no significant impairment of hand function
Oberlin Transfer (consolidating series)
- 18 patients (8 with C5-C6, 10 with C5-C6-C7 paralysis)
- 7 of 8 C5-C6 patients recovered useful elbow flexion after the transfer alone
- Results were poorer and often needed a supplementary Steindler when surgery was delayed beyond a few months
Double Fascicular Transfer (Mackinnon technique)
- 6 patients: expendable fascicles from BOTH ulnar and median nerves transferred to the biceps and brachialis branches
- Mean recovery of elbow flexion was MRC grade 4 plus
- No motor or sensory donor deficit; pinch and grip unchanged or improved
Double Fascicular Transfer (larger series)
- 29 patients; 28 (97 percent) regained elbow flexion
- 8 reached M5, 15 reached M4, 4 reached M3
- No functional deficit in the ulnar or median donor distributions
Nerve Transfers vs Nerve Grafting (upper plexus)
- Systematic review of 31 studies in traumatic upper-trunk (C5-C6) palsy
- M4+ elbow flexion: 247 of 299 (83 percent) after transfer vs 32 of 57 (56 percent) after grafting
- Dual transfer for shoulder gave M4+ abduction in 74 percent vs 46 percent for grafting
Triceps-to-Axillary (Leechavengvongs / Somsak group)
- Anatomic feasibility study in 36 cadaveric shoulder girdles
- Nerve to the long head of triceps reaches the anterior branch of the axillary nerve via a posterior approach without grafting
- Donor carries roughly 1,233 axons against approximately 2,704 in the axillary anterior branch
Intercostal-to-Biceps Transfer
- 17 patients with avulsion injury; intercostal neurotisation of biceps, mean 5-year follow-up
- 8 of 17 (47 percent) achieved good or excellent elbow flexion
- Results improved when surgery was done under 5 months and in patients under 50 years
Distal Median-to-Ulnar (AIN) Transfer
- Technical description of AIN to deep motor branch of ulnar nerve to restore intrinsic function
- Combined with median third-webspace sensory transfer for ulnar volar sensation
- Reduces denervation time for distal intrinsics in proximal (Sunderland IV-V) ulnar injury
Nerve Reconstruction vs Free Muscle Transfer (late cases)
- Systematic review, 103 patients presenting at 12 months or later
- Upper-trunk M3+ elbow flexion: 53 percent after nerve reconstruction vs 100 percent after free functional muscle transfer
- For total plexus injuries, free muscle transfer outperformed nerve reconstruction (78 vs 37 percent M3+)
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: The Erb's Palsy
"A 25-year-old male motorcyclist presents with a C5/C6 avulsion injury 4 months post-accident. No recovery. Examination shows deltoid/biceps paralysis. Hand is normal."
Scenario 2: High Ulnar Nerve
"Patient with a high ulnar nerve transection at the axilla. 6 months post-injury. Primary repair was done but prognosis is guarded."
Scenario 3: Total Plexus Avulsion
"A 22-year-old male sustained a motorcycle accident with complete C5-T1 avulsion injury. MRI shows pseudomeningoceles at all levels. He presents at 5 months with a flail arm."
MCQ Practice Points
Anatomy
Q: Which fascicle of the Ulnar nerve is used in the Oberlin transfer? A: The fascicle supplying the Flexor Carpi Ulnaris (FCU).
Physiology
Q: What is the maximum time window for successful motor nerve transfer? A: Generally 12-18 months before motor end plate fibrosis.
Complications
Q: What is the risk of using the Phrenic nerve as a donor? A: Hemidiaphragm paralysis (Reduced Vital Capacity).
Oberlin Transfer
Q: What is the Oberlin transfer and what does it restore? A: Transfer of Ulnar FCU fascicle to Biceps motor branch. Restores elbow flexion in C5/C6 injuries.
AIN Transfer
Q: What is the purpose of AIN to Ulnar motor transfer? A: Prevents clawing and restores pinch in high ulnar nerve injuries. Reinnervates intrinsic muscles before motor end plate fibrosis.
Regeneration Rate
Q: What is the rate of nerve regeneration after repair? A: Approximately 1mm per day (1 inch per month). This determines the urgency of distal transfers for long injuries.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Traumatic adult brachial plexus injury is overwhelmingly a disease of young men: most series report a male-to-female ratio of roughly 4-9 to 1 with peak incidence in the late teens to mid-30s.
- High-energy motorcycle and road-traffic trauma is the dominant mechanism worldwide, accounting for the majority of supraclavicular avulsion injuries in most published cohorts.
- The burden is disproportionately high in regions with large motorcycle populations (parts of South and Southeast Asia, Latin America), which is also where several of the landmark distal-transfer techniques were developed and refined.
Side-by-Side Society / Group Practice (no formal RCT-based guideline exists):
| Domain | Common international position |
|---|---|
| Timing of referral | Sharp/penetrating injury: explore early (ideally within days). Closed injury with no recovery: refer by 3 months, operate by 3-6 months. |
| Investigation | CT myelography remains the reference for root avulsion; MR neurography is increasingly used and is less invasive. Baseline EMG/NCS deferred to about 3-4 weeks. |
| Upper-trunk reconstruction | Strong convergence (supported by Garg et al.) toward dual nerve transfer over long interposition grafts for shoulder and elbow. |
| Late presentation | Reserve donor nerves for free functioning muscle transfer rather than late nerve reconstruction (supported by Hoang/Seruya). |
Registry and Network Notes:
- Unlike arthroplasty, there is no large international implant-style registry for nerve transfers; evidence is pooled from high-volume centre series and systematic reviews.
- Dedicated multidisciplinary peripheral-nerve and brachial-plexus services (combining plastic, orthopaedic, hand and neurosurgery with specialist hand therapy) consistently report better and more reproducible outcomes than ad hoc care.
High- vs Limited-Resource Practice Variation:
- High-resource settings: routine microsurgical fascicular transfers, intra-operative nerve stimulation, MR neurography, and structured biofeedback rehabilitation over 12-24 months.
- Limited-resource settings: greater reliance on extra-plexus donors (intercostal, spinal accessory) and on tendon transfers or free muscle transfer where microsurgical theatre time, nerve stimulators or long-term therapy are scarce; later presentation is common, shifting the balance toward muscle transfer.
Clinical summary
Principles
- •Donor Expendability
- •Recipient Viability
- •Proximity (Distal target)
- •Synergy (Easier rehab)
Common Transfers
- •Oberlin: Ulnar to Biceps (Elbow flexion)
- •Somsak: Intercostal to MC (Elbow flexion)
- •XI to SSN: Shoulder reanimation
- •AIN to Ulnar: Intrinsic salvage
Timing
- •Early: 3-6 months (ideal)
- •Late: Greater than 12 months (Muscle transfer required)
- •Motor end plate fibrosis by 18 months
- •Regeneration: 1mm/day