Benign Peripheral Nerve Sheath Tumor | NF1 Association | MPNST Risk
Anatomical Classification
Critical Must-Knows
- Neurofibroma consists of Schwann cells, fibroblasts, and perineural cells in myxoid matrix
- Plexiform neurofibromas are pathognomonic for NF1 and have 8-13% lifetime MPNST risk
- Histology shows wavy nuclei, myxoid stroma, and diffuse S100 positivity without Antoni patterns
- Rapid growth, pain, neurological deficit suggest malignant transformation to MPNST
- Localized neurofibromas can be excised; plexiform require careful surveillance
Clinical Pearls
- "Distinguish from schwannoma: neurofibroma cannot be separated from nerve, Schwann cell plus fibroblast mix
- "Plexiform neurofibroma creates bag of worms appearance, virtually diagnostic of NF1
- "MPNST arises in 8-13% of plexiform neurofibromas, heralded by pain and rapid growth
- "Complete excision of localized neurofibroma requires sacrificing nerve fascicles
Critical Neurofibroma Exam Points
Malignant Transformation
Plexiform neurofibromas in NF1 have 8-13% lifetime MPNST risk. Red flags: rapid growth, pain, neurological deficit, size over 5cm. PET-CT and MRI with contrast help detect transformation.
NF1 Association
Plexiform neurofibromas are pathognomonic for NF1. Multiple cutaneous neurofibromas also suggest NF1. Screen for cafe-au-lait spots, axillary freckling, Lisch nodules, family history.
Histological Features
Wavy nuclei in myxoid matrix with diffuse S100 positivity. Mixed Schwann cells and fibroblasts (unlike pure Schwann cell schwannoma). No Antoni A/B patterns or Verocay bodies.
Surgical Principles
Localized: simple excision with nerve sacrifice. Plexiform: observation or debulking for symptoms. Cannot separate from nerve (unlike schwannoma). High recurrence in diffuse type (20-40%).
NERVENeurofibroma Key Features
| N | NF1 association Plexiform type pathognomonic for neurofibromatosis type 1 |
| E | Embedded in nerve Cannot be separated from nerve (vs schwannoma which shells out) |
| R | Rope-like plexiform Bag of worms appearance along nerve distribution |
| V | Variable S100 staining Diffuse but patchy S100 positivity (Schwann cells plus fibroblasts) |
| E | Eight to thirteen percent MPNST Lifetime malignant transformation risk in plexiform type |
| N | NF1 association Plexiform type pathognomonic for neurofibromatosis type 1 | V | Variable S100 staining Diffuse but patchy S100 positivity (Schwann cells plus fibroblasts) |
| E | Embedded in nerve Cannot be separated from nerve (vs schwannoma which shells out) | E | Eight to thirteen percent MPNST Lifetime malignant transformation risk in plexiform type |
| R | Rope-like plexiform Bag of worms appearance along nerve distribution |
Hook:NERVE tumors: Neurofibroma embedded in nerve with NF1 association and MPNST risk!
WAVYHistological Triad
| W | Wavy nuclei Serpentine, buckled nuclei characteristic of Schwann cells |
| A | Admixed cell types Schwann cells plus fibroblasts plus perineural cells (not pure) |
| V | Vague borders Poorly circumscribed, infiltrative growth pattern |
| Y | Yielding myxoid matrix Abundant myxoid stroma with fine collagen fibers |
| W | Wavy nuclei Serpentine, buckled nuclei characteristic of Schwann cells | V | Vague borders Poorly circumscribed, infiltrative growth pattern |
| A | Admixed cell types Schwann cells plus fibroblasts plus perineural cells (not pure) | Y | Yielding myxoid matrix Abundant myxoid stroma with fine collagen fibers |
Hook:WAVY nuclei in myxoid matrix with admixed cells - hallmark of neurofibroma!
RAPIDMPNST Red Flags
| R | Rapid growth Growth over weeks to months in previously stable lesion |
| A | Aching pain New onset pain in previously painless neurofibroma |
| P | Positron uptake on PET SUV over 3.5 suggests malignancy |
| I | Irregular margins Loss of circumscription, infiltrative borders on MRI |
| D | Deficit neurological Progressive motor or sensory deficit |
| R | Rapid growth Growth over weeks to months in previously stable lesion | I | Irregular margins Loss of circumscription, infiltrative borders on MRI |
| A | Aching pain New onset pain in previously painless neurofibroma | D | Deficit neurological Progressive motor or sensory deficit |
| P | Positron uptake on PET SUV over 3.5 suggests malignancy |
Hook:RAPID changes in neurofibroma require urgent MPNST workup!
Overview and Epidemiology
Neurofibroma is a benign peripheral nerve sheath tumor arising from a mixture of Schwann cells, fibroblasts, and perineural cells within a myxoid stromal matrix. It represents approximately 5% of all benign soft tissue tumors. The tumor occurs in three distinct clinical forms: localized (solitary), diffuse, and plexiform, each with different associations, behavior, and treatment implications.
Clinical Significance
Neurofibromas are clinically important because: (1) plexiform neurofibromas are virtually pathognomonic for NF1; (2) they have significant malignant transformation risk to MPNST in NF1 patients (8-13% lifetime risk); (3) unlike schwannomas, they cannot be separated from parent nerve requiring nerve sacrifice; and (4) diffuse cutaneous neurofibromas cause significant morbidity and disfigurement.
Demographics
- Age: Solitary type 20-40 years; NF1-associated from childhood
- Sex: Equal male to female distribution
- Location: Any nerve; plexiform favors large nerves and plexuses
- NF1: 50% of plexiform, less than 5% of solitary
Clinical Forms
- Localized (Solitary): Single lesion, not NF1-associated (90%)
- Diffuse: Plaque-like skin lesions, young adults
- Plexiform: Multiple fascicles, bag of worms, pathognomonic NF1
- Multiple cutaneous: Suggests NF1 diagnosis
Pathophysiology and Molecular Biology
Cellular Origin and Composition
Neurofibromas arise from the peripheral nerve sheath and consist of a heterogeneous cell population including Schwann cells, fibroblasts, perineural-like cells, and mast cells embedded within a myxoid collagenous matrix. This mixed cellular composition distinguishes neurofibromas from schwannomas, which contain only Schwann cells.
NF1 and Malignant Transformation
Patients with NF1 have germline mutations in the NF1 tumor suppressor gene (chromosome 17q11.2) encoding neurofibromin, a RAS-GTPase activating protein. Loss of neurofibromin leads to constitutive RAS activation. Plexiform neurofibromas in NF1 have 8-13% lifetime risk of malignant transformation to MPNST, particularly with additional mutations in TP53 and CDKN2A/B.
Neurofibroma vs Schwannoma Cellular Composition
| Feature | Neurofibroma | Schwannoma |
|---|---|---|
| Cell types | Schwann cells plus fibroblasts plus perineural cells | Pure Schwann cells |
| Separation from nerve | Cannot be separated (intrinsic) | Can be dissected free (eccentric) |
| S100 pattern | Diffuse but patchy (50-90% cells) | Uniform strong (100% cells) |
| Capsule | Poorly defined, infiltrative | Well-defined capsule |
| Antoni patterns | Absent | Present (Antoni A and B areas) |
| Verocay bodies | Absent | Present in Antoni A areas |
| NF association | Plexiform type pathognomonic for NF1 | NF2 association (bilateral vestibular schwannomas) |
Molecular Pathogenesis
NF1 Gene and Pathway
- Gene: NF1 on chromosome 17q11.2
- Protein: Neurofibromin (RAS-GAP)
- Function: Inactivates RAS signaling
- Loss: Constitutive RAS-MAPK activation
MPNST Transformation
- First hit: Germline NF1 mutation (inherited)
- Second hit: Somatic NF1 loss of heterozygosity
- Additional: TP53, CDKN2A/B, SUZ12 mutations
- Result: Progression to high-grade sarcoma
Classification and Clinical Types
Neurofibroma Clinical Types
| Type | Clinical Features | NF1 Association | Location | Malignant Risk | Treatment |
|---|---|---|---|---|---|
| Localized (Solitary) | Single nodule, skin or nerve, painless | Rare (less than 5%) | Any peripheral nerve, dermis | Less than 1% | Excision if symptomatic |
| Diffuse | Plaque-like, skin thickening | Occasional (10-20%) | Head/neck, trunk | Less than 5% | Wide excision, high recurrence (20-40%) |
| Plexiform | Bag of worms, multiple fascicles | Pathognomonic (100% if present) | Large nerves and plexuses | 8-13% lifetime | Observation, debulking for symptoms, MPNST surveillance |
Localized (Solitary) Neurofibroma
Localized neurofibromas present as single, slowly growing, painless nodules typically in young to middle-aged adults (20-40 years). They arise within the dermis (cutaneous) or along peripheral nerves (intraneural). Most are sporadic without NF1 association.
Clinical Features:
- Soft, mobile subcutaneous or dermal nodule
- Skin lesions may have buttonhole sign (invagination with pressure)
- Painless unless compressing adjacent structures
- Size typically 1-3cm
- Do not transilluminate (unlike schwannomas which may)
Diffuse Neurofibroma
Diffuse neurofibromas present as poorly defined, plaque-like thickenings of skin and subcutaneous tissue. They typically occur in children and young adults, often involving the head, neck, or trunk. They have infiltrative growth pattern making complete excision difficult.
Clinical Features:
- Ill-defined, soft tissue swelling
- Skin thickening with loss of normal texture
- May cause hypertrophy of underlying tissues
- Hyperpigmentation common
- Disfiguring lesions
Plexiform Neurofibroma
Plexiform neurofibromas are pathognomonic for NF1 when present. They involve multiple nerve fascicles along the length of a nerve or plexus, creating a characteristic bag of worms appearance. They are typically congenital or develop in early childhood.
Clinical Features:
- Rope-like or bag of worms masses
- Palpable along nerve distribution
- May cause limb overgrowth and elephantiasis
- Can involve deeper structures (mediastinum, retroperitoneum)
- Often associated with overlying hyperpigmented skin
Pathognomonic Sign
The presence of a plexiform neurofibroma is virtually diagnostic of NF1. If you identify a bag of worms mass involving multiple nerve fascicles, NF1 should be strongly suspected and the patient evaluated for other diagnostic criteria including cafe-au-lait spots, axillary/groin freckling, Lisch nodules, and family history.
Clinical Presentation and Diagnosis
History
Typical Presentation
- Solitary: Painless subcutaneous nodule, incidental finding
- Plexiform: Congenital or childhood mass, family history NF1
- Symptoms: Usually asymptomatic unless compressive
- Growth: Slow, stable (rapid growth suggests MPNST)
Red Flag Symptoms
- Pain: New onset or worsening (suggests MPNST)
- Rapid growth: Size increase over weeks to months
- Neurological deficit: Motor weakness or sensory loss
- Systemic: Weight loss, fatigue (advanced MPNST)
Physical Examination
Inspection:
- Size, location, overlying skin changes
- Multiple lesions suggest NF1
- Cafe-au-lait spots (6 or more over 5mm prepubertal, over 15mm postpubertal)
- Axillary or inguinal freckling (Crowe sign)
- Lisch nodules on slit lamp examination (iris hamartomas)
Palpation:
- Soft, non-tender mass (tenderness suggests MPNST)
- Buttonhole sign: cutaneous neurofibroma invaginates with pressure
- Bag of worms: multiple nodules along nerve (plexiform type)
- Cannot be separated from nerve (unlike schwannoma)
- Tinel sign may be present but less prominent than schwannoma
Special Tests:
- Assess motor and sensory function of affected nerve
- Document any neurological deficits
- Measure limb circumference if hypertrophy present
NF1 Diagnostic Criteria
A patient is diagnosed with NF1 if they have 2 or more of the following:
- Six or more cafe-au-lait spots: over 5mm prepubertal or over 15mm postpubertal
- Two or more neurofibromas of any type or one plexiform neurofibroma
- Axillary or inguinal freckling
- Optic glioma
- Two or more Lisch nodules (iris hamartomas)
- Distinctive osseous lesion: sphenoid dysplasia, tibial pseudarthrosis, or bowing
- First-degree relative with NF1 by above criteria
Investigations and Imaging
Laboratory Tests
Routine:
- Complete blood count: baseline (usually normal)
- Basic metabolic panel: preoperative assessment
- Genetic testing: NF1 gene sequencing if clinical diagnosis uncertain
Histopathology:
- Core needle biopsy for deep lesions over 5cm
- Excisional biopsy for accessible superficial lesions
- Immunohistochemistry: S100 to confirm nerve sheath origin
Biopsy Considerations
Biopsy of suspected plexiform neurofibromas should be performed carefully as they are highly vascular and may bleed significantly. Image-guided core needle biopsy is preferred over open biopsy for deep lesions. Always consider MPNST in the differential for atypical or rapidly growing lesions.
Imaging Studies
Imaging Modalities for Neurofibroma
| Modality | Findings | Indication | Limitations |
|---|---|---|---|
| MRI (T1-weighted) | Isointense to muscle, well-defined | Lesion characterization, MPNST surveillance | Cannot reliably distinguish benign from malignant |
| MRI (T2-weighted) | Hyperintense, target sign (central low signal) | Best for anatomical delineation | Target sign only in 50% of cases |
| MRI with contrast | Variable enhancement; MPNST shows heterogeneous uptake | Differentiate from MPNST | Some benign neurofibromas also enhance |
| PET-CT | SUV less than 2.5 benign; over 3.5 suggests MPNST | MPNST surveillance in high-risk patients | False positives with inflammation |
| Ultrasound | Hypoechoic, well-defined, posterior enhancement | Superficial lesion assessment, biopsy guidance | Limited for deep or large lesions |
MRI Target Sign:
- Central hypointensity on T2-weighted images
- Corresponds to fibrous tissue and collagen
- Peripheral hyperintensity from myxoid matrix
- Seen in approximately 50% of neurofibromas
- Not pathognomonic but suggestive
Histopathology and Immunohistochemistry
Macroscopic Appearance:
- Poorly circumscribed, fusiform expansion of nerve
- Cannot be separated from nerve fascicles
- Cut surface: grey-white, gelatinous, mucoid
- Plexiform type: multiple nodules like bag of worms
Microscopic Features:
Histological Features
| Feature | Description | Clinical Significance |
|---|---|---|
| Wavy nuclei | Serpentine, buckled nuclei characteristic of Schwann cells | Classic feature shared with schwannoma |
| Mixed cellularity | Schwann cells plus fibroblasts plus perineural cells plus mast cells | Distinguishes from pure Schwann cell schwannoma |
| Myxoid matrix | Abundant loose myxoid stroma with fine collagen fibers | Creates soft consistency clinically |
| No Antoni patterns | Absent Antoni A (compact) and Antoni B (loose) areas | Differentiates from schwannoma |
| No Verocay bodies | Absent nuclear palisading structures | Further evidence against schwannoma |
| Poorly circumscribed | Infiltrative growth into surrounding tissues | Cannot achieve clean surgical margins |
Immunohistochemistry:
- S100 protein: Positive in 50-90% of cells (patchy, not diffuse like schwannoma)
- CD34: Positive in fibroblast component
- EMA (epithelial membrane antigen): Highlights perineural cells
- Neurofilament: Positive in entrapped axons
- Ki-67: Low proliferation index (less than 5%); high in MPNST (over 10%)
Histological Diagnosis
The diagnosis of neurofibroma requires recognition of wavy nuclei in myxoid matrix with mixed Schwann cells and fibroblasts, diffuse (but patchy) S100 positivity, and absence of Antoni patterns or Verocay bodies. If these features are atypical or show high cellularity, increased mitoses, or necrosis, consider MPNST.
Differential Diagnosis
Differential Diagnosis of Neurofibroma
| Condition | Clinical Clues | Histology | Imaging | S100 Staining |
|---|---|---|---|---|
| Schwannoma | Eccentric, can be shelled out, Tinel sign | Pure Schwann cells, Antoni A/B, Verocay bodies | Target sign on MRI, cystic degeneration common | Diffuse uniform 100% positive |
| MPNST | Rapid growth, pain, neurological deficit, NF1 | High cellularity, mitoses over 4 per 10 HPF, necrosis | Heterogeneous, irregular margins, SUV over 3.5 | Variable 50-70%, focal |
| Perineurioma | Young adults, superficial nerves, painless | Perineurial cells, whorled pattern | Target sign similar to neurofibroma | Negative; EMA positive |
| Lipoma | Soft, mobile, no Tinel sign | Mature adipocytes without atypia | Fat signal on MRI, suppresses on fat sat | Negative |
| Ganglion cyst | Transilluminates, fluctuant, joint-associated | Mucin-filled cyst without epithelial lining | Homogeneous T2 hyperintense, no enhancement | Negative |
| Desmoid tumor | Firm, fixed, young adults, trauma history | Fibroblastic proliferation, infiltrative | T2 heterogeneous, low to intermediate signal | Negative; beta-catenin positive |
Do Not Miss MPNST
The most critical differential diagnosis is distinguishing benign neurofibroma from malignant peripheral nerve sheath tumor (MPNST). Red flags include: (1) rapid growth; (2) pain or neurological deficit; (3) size over 5cm; (4) heterogeneous enhancement on MRI; (5) PET SUV over 3.5; (6) histology showing high cellularity, mitoses, or necrosis. If any red flags present, urgent referral to sarcoma center is mandatory.
Management Algorithm
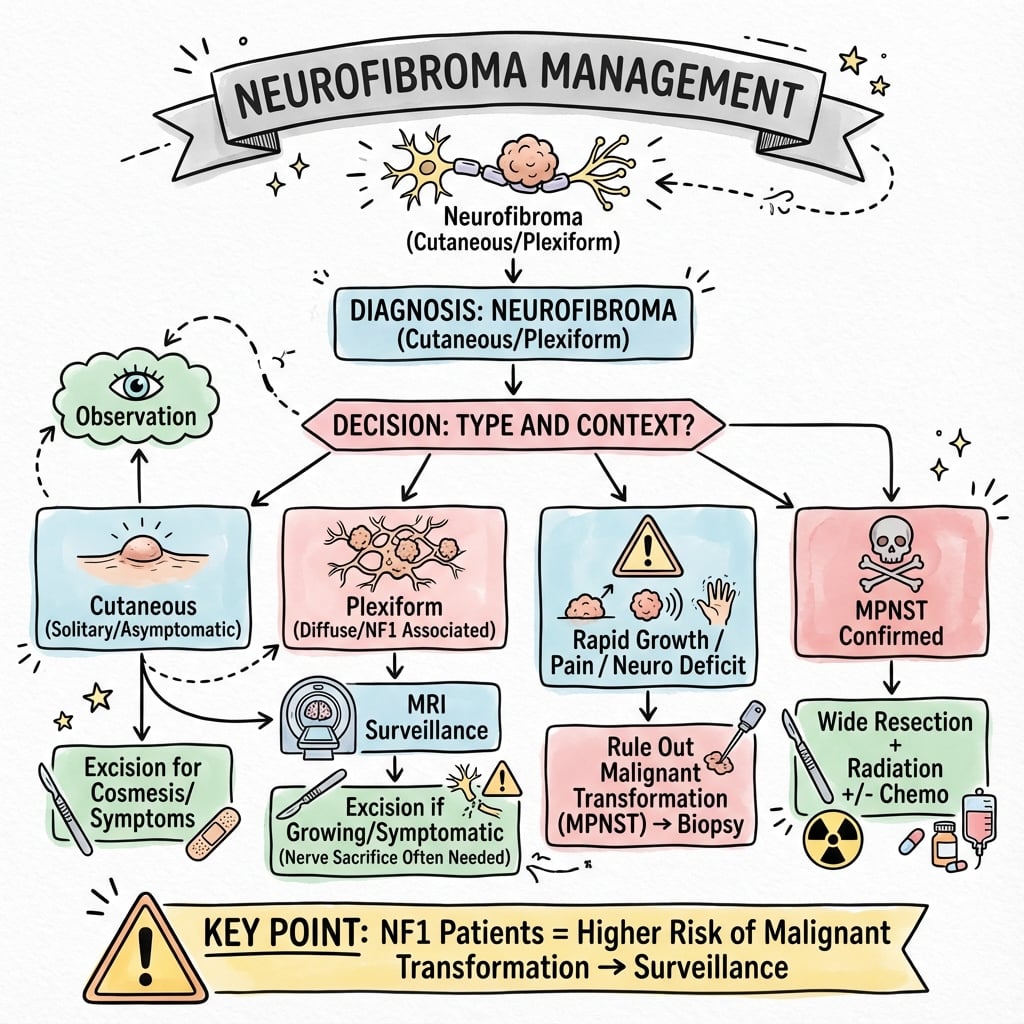
Treatment Algorithm
- Confirm diagnosis: clinical examination and imaging
- Determine type: localized, diffuse, or plexiform
- Screen for NF1 if plexiform or multiple lesions
- Assess symptoms: pain, neurological deficit, cosmetic concern
Initial assessment establishes treatment pathway.
- Low risk: Solitary, asymptomatic, stable size, no NF1
- Intermediate risk: Diffuse type, cosmetic concern, no NF1
- High risk: Plexiform with NF1, size over 5cm, rapid growth, pain
Risk guides surveillance intensity.
- Observation: Asymptomatic solitary neurofibroma, stable plexiform
- Surgical excision: Symptomatic, cosmetic concern, diagnostic uncertainty
- MPNST surveillance: High-risk plexiform in NF1 (annual MRI, PET)
Treatment individualized to patient needs.
Treatment by Neurofibroma Type
| Type | First-Line Treatment | Surgical Approach | Recurrence Risk | Follow-Up |
|---|---|---|---|---|
| Localized (Solitary) | Observation if asymptomatic; excision if symptomatic | Simple excision with nerve sacrifice of involved fascicles | Less than 5% | None if completely excised |
| Diffuse | Wide excision if symptomatic or cosmetic concern | Wide excision with margin, may need reconstruction | 20-40% (infiltrative growth) | Clinical surveillance for recurrence |
| Plexiform (NF1) | Observation; debulking only if compressive symptoms | Subtotal resection preserving nerve function | Variable (incomplete excision expected) | Annual MRI and PET-CT for MPNST surveillance |
Conservative Management
Indications for Observation:
- Asymptomatic localized neurofibroma
- Stable plexiform neurofibroma in NF1 patient
- No evidence of malignant transformation
- Small lesions (less than 3cm) without functional impact
Surveillance Protocol for High-Risk Patients (NF1 with Plexiform):
- Clinical examination every 6-12 months
- Baseline MRI with contrast at diagnosis
- Annual MRI for lesions over 3cm or symptomatic
- PET-CT if concern for MPNST (SUV over 3.5 suspicious)
- Patient education on red flag symptoms: pain, rapid growth, deficit
Surgical Management
Indications for Surgery
Absolute Indications:
- Suspected malignant transformation (MPNST)
- Progressive neurological deficit
- Severe pain unresponsive to conservative measures
- Diagnostic uncertainty (rule out malignancy)
Relative Indications:
- Symptomatic compression of adjacent structures
- Cosmetic disfigurement causing psychological distress
- Functional impairment (limited range of motion, daily activities)
- Patient preference for asymptomatic but growing lesion
Contraindications:
- Medical comorbidities precluding surgery
- Extensive plexiform neurofibroma where resection would cause severe deficit
- Multiple small asymptomatic lesions in NF1
Surgical decision-making balances symptom relief against risk of neurological deficit from nerve sacrifice.
Novel and Emerging Therapies
MEK Inhibitors (Selumetinib)
- Indication: Progressive symptomatic plexiform neurofibromas in NF1 children
- Mechanism: Inhibits MEK in RAS-MAPK pathway
- Efficacy: 70% partial response, tumor volume reduction
- FDA approval: 2020 for pediatric NF1 plexiform
Future Therapies
- mTOR inhibitors: Sirolimus trials for plexiform neurofibromas
- HDAC inhibitors: Epigenetic modulation trials
- Immunotherapy: PD-1 inhibitors for MPNST
- Gene therapy: NF1 gene replacement (preclinical)
Complications and Prognosis
Complications of Neurofibroma
Complications by Type
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Malignant transformation (MPNST) | 8-13% lifetime in NF1 plexiform; less than 1% sporadic | NF1, plexiform type, size over 5cm, radiation | Urgent referral to sarcoma center, wide excision with adjuvant therapy |
| Recurrence after excision | Less than 5% localized; 20-40% diffuse; variable plexiform | Incomplete excision, diffuse or plexiform type | Re-excision if symptomatic, surveillance if asymptomatic |
| Neurological deficit | Expected with nerve sacrifice; 10-20% plexiform debulking | Intraneural location, sacrifice of motor fascicles | Rehabilitation, splinting, gabapentin for pain |
| Disfigurement and psychosocial impact | Common in multiple cutaneous and plexiform NF1 | Visible location, multiple lesions, NF1 | Psychological support, selective excision, MEK inhibitors |
| Surgical complications | Bleeding 5%, infection less than 5%, wound dehiscence rare | Vascular plexiform lesions, poor wound healing | Standard surgical techniques, meticulous hemostasis |
Prognosis
Localized (Solitary) Neurofibroma:
- Excellent prognosis with complete excision
- Recurrence less than 5% if marginal margins achieved
- No malignant transformation risk in non-NF1 patients
- No systemic surveillance required
Diffuse Neurofibroma:
- Good overall prognosis but high local recurrence (20-40%)
- Infiltrative growth makes complete excision difficult
- Low malignant transformation risk (less than 5%)
- Clinical surveillance for recurrence recommended
Plexiform Neurofibroma in NF1:
- 8-13% lifetime risk of MPNST transformation
- Cannot be completely excised without major neurological deficit
- Require lifelong MPNST surveillance (annual MRI and PET-CT)
- MEK inhibitors (selumetinib) may reduce tumor burden and symptoms
- NF1-associated MPNST carries a poor prognosis (5-year survival approximately 21%, versus 42% for sporadic MPNST), so early detection is critical
Controversies and Areas of Uncertainty
ANNUBP - the malignant grey zone
The category atypical neurofibromatous neoplasm of uncertain biologic potential (ANNUBP, defined by CDKN2A/B loss and atypia short of MPNST) is now recognised by WHO, but thresholds for resection and surveillance of these premalignant lesions are not standardised.
How aggressive should plexiform surgery be?
Debulking relieves symptoms but recurrence is high and complete excision risks major deficit. With effective MEK inhibition, the balance between upfront surgery and medical therapy for symptomatic plexiform disease is shifting and remains debated.
Optimal imaging for transformation
FDG-PET (SUVmax cut-offs and tumour-to-liver ratio) improves MPNST detection but with false positives; whole-body MRI quantifies tumour burden. The ideal surveillance interval and modality combination are not settled.
Duration and role of MEK inhibitors
Selumetinib shrinks plexiform neurofibromas, but optimal treatment duration, rebound after cessation, adult efficacy and whether it reduces MPNST risk are all unresolved.
Evidence Base and Landmark Studies
Selumetinib in Children with Inoperable Plexiform Neurofibromas (Phase 2)
- Open-label phase 2 trial of oral selumetinib in 50 children with NF1 and symptomatic inoperable plexiform neurofibromas
- 35 of 50 children (70%) achieved a confirmed partial response, with 28 durable for at least 1 year
- Clinically meaningful improvements in tumour-related pain, quality of life, strength and range of motion
- Pivotal trial underpinning the 2020 FDA approval of selumetinib for paediatric NF1 plexiform neurofibroma
Activity of Selumetinib in NF1-Related Plexiform Neurofibromas (Phase 1)
- Phase 1 dose-finding trial of selumetinib in 24 children with NF1 and inoperable plexiform neurofibromas
- Maximum tolerated dose 25 mg/m2 twice daily; confirmed partial response in 17 of 24 children (71%)
- No disease progression observed during the reported follow-up period
- Established the dose and proof-of-concept that preceded the phase 2 registration trial
Lifetime MPNST Risk in Neurofibromatosis Type 1
- Population-based study (4.1 million, NW England) establishing a lifetime MPNST risk of 8-13% in NF1
- Median age at MPNST diagnosis 26 years in NF1 versus 62 years in sporadic MPNST
- 5-year survival only 21% for NF1-associated MPNST versus 42% for sporadic MPNST
- Findings justify lifelong surveillance and a low threshold for investigating new symptoms
UK Consensus Guidelines for Diagnosis and Management of NF1
- Consensus statement from the UK Neurofibromatosis Association Clinical Advisory Board
- Codifies the diagnostic criteria, major differential diagnoses and complication monitoring for NF1
- Recommends multidisciplinary surveillance and prompt assessment of suspicious lesions
- Widely cited international framework for structured NF1 follow-up
Pathology of Peripheral Nerve Sheath Tumours: Diagnostic Overview
- Authoritative review of diagnostic criteria for neurofibroma, schwannoma and perineurioma
- Neurofibroma: admixed Schwann cells, fibroblasts and perineurial-like cells, infiltrating the nerve
- Schwannoma: pure Schwann cells with Antoni A/B areas and Verocay bodies, shells out from nerve
- Provides guidance for grading atypical neurofibroma and separating it from low-grade MPNST
WHO Classification of Tumours: Soft Tissue and Bone (5th Edition)
- Defines neurofibroma subtypes: localized, diffuse, plexiform and atypical neurofibromatous neoplasm of uncertain biologic potential (ANNUBP)
- Plexiform neurofibroma is essentially pathognomonic for NF1
- ANNUBP recognised as an intermediate, premalignant step toward MPNST
- Histology: wavy nuclei, myxoid/collagenous matrix, mixed cellularity, patchy S100
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Solitary Neurofibroma Management
"A 35-year-old man presents with a 2cm painless mass in the volar forearm present for 3 years, slowly growing. Examination reveals a soft, non-tender subcutaneous nodule with a positive Tinel sign over the median nerve. MRI shows a well-defined T2 hyperintense lesion with target sign involving the median nerve. How would you manage this patient?"
Scenario 2: Plexiform Neurofibroma with MPNST Concern
"A 28-year-old woman with known NF1 presents with a plexiform neurofibroma in the left brachial plexus, present since childhood. Over the past 6 months, she reports rapid increase in size and new onset pain. MRI shows heterogeneous enhancement and the lesion has grown from 8cm to 12cm. PET-CT shows SUV of 4.2. How would you proceed?"
Scenario 3: Multiple Neurofibromas - NF1 Diagnosis
"A 22-year-old presents with multiple subcutaneous nodules on the trunk and extremities noticed over the past 5 years. She has no family history of similar lesions. Examination reveals over 20 soft, mobile, non-tender subcutaneous masses ranging from 0.5-3cm. You also note 8 cafe-au-lait spots over 15mm and axillary freckling. What is your diagnosis and management approach?"
Guidelines, Registries & Global Practice
Global Epidemiology
- NF1 incidence: approximately 1 in 2500-3000 live births worldwide; one of the most common autosomal dominant disorders, with no consistent racial or ethnic predilection
- Penetrance: nearly complete by adulthood, but expression is highly variable even within families; roughly 50% of cases are de novo mutations
- Plexiform neurofibroma: present in 30-50% of NF1 patients on whole-body MRI; the dominant source of malignant transformation risk
Side-by-Side Guidance
Major Society / Consensus Positions on NF1 and Plexiform Neurofibroma
| Body | Diagnostic Framework | Surveillance / Treatment Emphasis |
|---|---|---|
| NIH / revised international criteria (Legius 2021) | Updated NF1 criteria; adds a pathogenic NF1 variant and choroidal anomalies as criteria | Genetic confirmation increasingly used where phenotype is incomplete |
| UK consensus (Ferner 2007) / BOA pathway | Clinical 2-of-7 criteria; structured complication monitoring | Annual review, low threshold for imaging and sarcoma MDT referral |
| European Reference Network (GENTURIS) / EFORT-aligned sarcoma pathways | Emphasis on ANNUBP as a premalignant intermediate | Whole-body MRI for high tumour burden; FDG-PET for transformation work-up |
| US (FDA / NCCN-aligned sarcoma practice) | WHO histological classification including ANNUBP | Selumetinib approved for symptomatic inoperable paediatric plexiform NF; wide excision plus radiotherapy for MPNST |
Registry and Cohort Evidence
- There is no dedicated arthroplasty-style implant registry for neurofibroma; the key population evidence comes from national NF1 registers and cancer registries (e.g. the NW England population study, French and German NF reference cohorts) that established the 8-13% lifetime MPNST risk and the poor survival of NF1-associated MPNST.
- Pharmacovigilance and post-marketing data for selumetinib are tracked through regulator and trial-network registries rather than orthopaedic implant databases.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: access to whole-body MRI, FDG-PET, MEK inhibitor therapy and dedicated multidisciplinary NF1/sarcoma clinics enables structured surveillance and early MPNST detection.
- Limited-resource settings: surveillance relies more on clinical examination and targeted ultrasound/MRI; MEK inhibitors are frequently unavailable or unaffordable, so management of plexiform disease remains observation and selective surgical debulking, with later-stage MPNST presentation.
- Universally, patient education on red-flag symptoms (new pain, rapid growth, neurological deficit) is the single most transferable, low-cost surveillance tool.
NEUROFIBROMA - Exam Day Summary
Clinical summary
Key Definitions
- •Benign peripheral nerve sheath tumor from Schwann cells, fibroblasts, perineural cells in myxoid matrix
- •Three types: Localized (solitary, sporadic), Diffuse (plaque-like), Plexiform (bag of worms, NF1)
- •90% S100 positive; wavy nuclei; NO Antoni patterns or Verocay bodies (vs schwannoma)
- •Cannot be separated from nerve (intraneural) - requires fascicular sacrifice for excision
NF1 Criteria (2 of 7 required)
- •6 plus cafe-au-lait spots (over 5mm pre-puberty, over 15mm post-puberty)
- •2 plus neurofibromas of any type OR 1 plexiform neurofibroma
- •Axillary or inguinal freckling (Crowe sign)
- •Optic glioma; 2 plus Lisch nodules; osseous lesion; 1st degree relative with NF1
MPNST Red Flags
- •Rapid growth over weeks-months; New onset or worsening pain; Neurological deficit
- •Size over 5cm; Heterogeneous MRI enhancement; PET SUV over 3.5
- •High cellularity, mitoses over 4/10 HPF, necrosis on histology
- •8-13% lifetime risk in NF1 plexiform; urgent sarcoma MDT referral
Imaging Pearls
- •MRI target sign: Central T2 hypointense (fibrous), peripheral hyperintense (myxoid) - 50% cases
- •T1 isointense to muscle; T2 hyperintense; variable enhancement
- •PET-CT: SUV less than 2.5 benign; over 3.5 MPNST concern
- •Plexiform: Bag of worms along nerve distribution on MRI
Treatment by Type
- •Localized: Observation if asymptomatic; excision with nerve sacrifice if symptomatic (less than 5% recurrence)
- •Diffuse: Wide excision if symptomatic; 20-40% recurrence (infiltrative growth)
- •Plexiform NF1: Observation plus MPNST surveillance (annual MRI, PET); debulking only for compression
- •MEK inhibitor (selumetinib) for progressive plexiform in NF1 children - 70% partial response
Histology vs Schwannoma
- •Neurofibroma: Mixed Schwann plus fibroblasts; wavy nuclei; myxoid; patchy S100; NO Antoni/Verocay
- •Schwannoma: Pure Schwann cells; Antoni A/B; Verocay bodies; uniform 100% S100
- •Neurofibroma: Cannot shell out (intraneural); Schwannoma: Can be dissected free (eccentric)
- •Both have wavy nuclei; differentiate by cellularity mix and Antoni patterns
Exam Traps to Avoid
- •Assuming neurofibroma can be shelled out like schwannoma (WRONG - intraneural, needs nerve sacrifice)
- •Missing NF1 diagnosis when plexiform or multiple lesions present
- •Not screening for MPNST in NF1 plexiform (8-13% lifetime risk, needs annual surveillance)
- •Offering wide excision for benign lesion (marginal margins adequate for localized type)
References
-
WHO Classification of Tumours Editorial Board. Soft Tissue and Bone Tumours. WHO Classification of Tumours. 5th ed. Lyon: IARC Press; 2020.
-
Ferner RE, Huson SM, Thomas N, et al. Guidelines for the diagnosis and management of individuals with neurofibromatosis 1. J Med Genet. 2007;44(2):81-88. doi:10.1136/jmg.2006.045906
-
Gross AM, Wolters PL, Dombi E, et al. Selumetinib in children with inoperable plexiform neurofibromas. N Engl J Med. 2020;382(15):1430-1442. doi:10.1056/NEJMoa1912735
-
Evans DG, Baser ME, McGaughran J, et al. Malignant peripheral nerve sheath tumours in neurofibromatosis 1. J Med Genet. 2002;39(5):311-314. doi:10.1136/jmg.39.5.311
-
Rodriguez FJ, Folpe AL, Giannini C, Perry A. Pathology of peripheral nerve sheath tumors: diagnostic overview and update on selected diagnostic problems. Acta Neuropathol. 2012;123(3):295-319. doi:10.1007/s00401-012-0954-z
-
Xu GZ, Li YH, Zhao DP, et al. Comparison of dumbbell-shaped schwannomas and neurofibromas in the upper extremities. Acta Neurochir (Wien). 2009;151(6):653-661. doi:10.1007/s00701-009-0280-8
-
Woodruff JM, Godwin TA, Erlandson RA, et al. Cellular schwannoma: a variety of schwannoma sometimes misinterpreted as a malignant tumor. Am J Surg Pathol. 1981;5(8):733-744.
-
Beert E, Brems H, Daniëls B, et al. Atypical neurofibromas in neurofibromatosis type 1 are premalignant tumors. Genes Chromosomes Cancer. 2011;50(12):1021-1032. doi:10.1002/gcc.20921
-
Mautner VF, Asuagbor FA, Dombi E, et al. Assessment of benign tumor burden by whole-body MRI in patients with neurofibromatosis 1. Neuro Oncol. 2008;10(4):593-598. doi:10.1215/15228517-2008-011
-
Salamon J, Veldhoen S, Apostolova I, et al. 18F-FDG PET/CT for detection of malignant peripheral nerve sheath tumours in neurofibromatosis type 1: tumour-to-liver ratio is superior to an SUVmax cut-off. Eur Radiol. 2014;24(2):405-412. doi:10.1007/s00330-013-3020-x
-
Farid M, Demicco EG, Garcia R, et al. Malignant peripheral nerve sheath tumors. Oncologist. 2014;19(2):193-201. doi:10.1634/theoncologist.2013-0328
-
Dunn GP, Spiliopoulos K, Plotkin SR, et al. Role of resection of malignant peripheral nerve sheath tumors in patients with neurofibromatosis type 1. J Neurosurg. 2013;118(1):142-148. doi:10.3171/jns.2012.9.JNS101610
-
Stucky CC, Johnson KN, Gray RJ, et al. Malignant peripheral nerve sheath tumors (MPNST): the Mayo Clinic experience. Ann Surg Oncol. 2012;19(3):878-885. doi:10.1245/s10434-011-1978-7
-
Dombi E, Baldwin A, Marcus LJ, et al. Activity of selumetinib in neurofibromatosis type 1-related plexiform neurofibromas. N Engl J Med. 2016;375(26):2550-2560. doi:10.1056/NEJMoa1605943
-
Fisher MJ, Avery RA, Allen JC, et al. Functional outcome measures for NF1-associated optic pathway glioma clinical trials. Neurology. 2013;81(21 Suppl 1):S15-S24. doi:10.1212/01.wnl.0000435745.95155.b8
-
Needle MN, Cnaan A, Dattilo J, et al. Prognostic signs in the surgical management of plexiform neurofibroma: the Children's Hospital of Philadelphia experience, 1974-1994. J Pediatr. 1997;131(5):678-682. doi:10.1016/s0022-3476(97)70092-1
-
Bhargava R, Parham DM, Lasater OE, et al. MR imaging differentiation of benign and malignant peripheral nerve sheath tumors: use of the target sign. Pediatr Radiol. 1997;27(2):124-129. doi:10.1007/s002470050082
-
Jett K, Friedman JM. Clinical and genetic aspects of neurofibromatosis 1. Genet Med. 2010;12(1):1-11. doi:10.1097/GIM.0b013e3181bf15e3