The Benign 'Pseudosarcoma'
- Nodular fasciitis is a BENIGN, SELF-LIMITING proliferation of MYOFIBROBLASTS - the classic 'PSEUDOSARCOMA', repeatedly mistaken for a sarcoma because of its rapid growth and cellular, mitotically active appearance. Long taught as a REACTIVE lesion, it is now known to be CLONAL and therefore NEOPLASTIC - a TRANSIENT clonal neoplasm that grows fast, plateaus and involutes rather than progressing.
- It presents as a RAPIDLY GROWING, usually SMALL (typically under 3-4 cm), SOLITARY, sometimes tender subcutaneous or fascial NODULE, classically on the VOLAR FOREARM, trunk or (in children) the HEAD and NECK; the rapid growth is the main feature that raises alarm for malignancy.
- Despite being mitotically active, it is GENETICALLY a transient self-limiting neoplasm characterised by a USP6 GENE REARRANGEMENT - most commonly the MYH9-USP6 fusion - demonstrable by molecular testing (USP6 FISH). USP6 rearrangement argues STRONGLY AGAINST sarcoma and SUPPORTS the diagnosis in the right morphological context, but it is SHARED with myositis ossificans, primary aneurysmal bone cyst and postoperative spindle cell nodule, so it does not by itself establish which USP6-associated lesion this is.
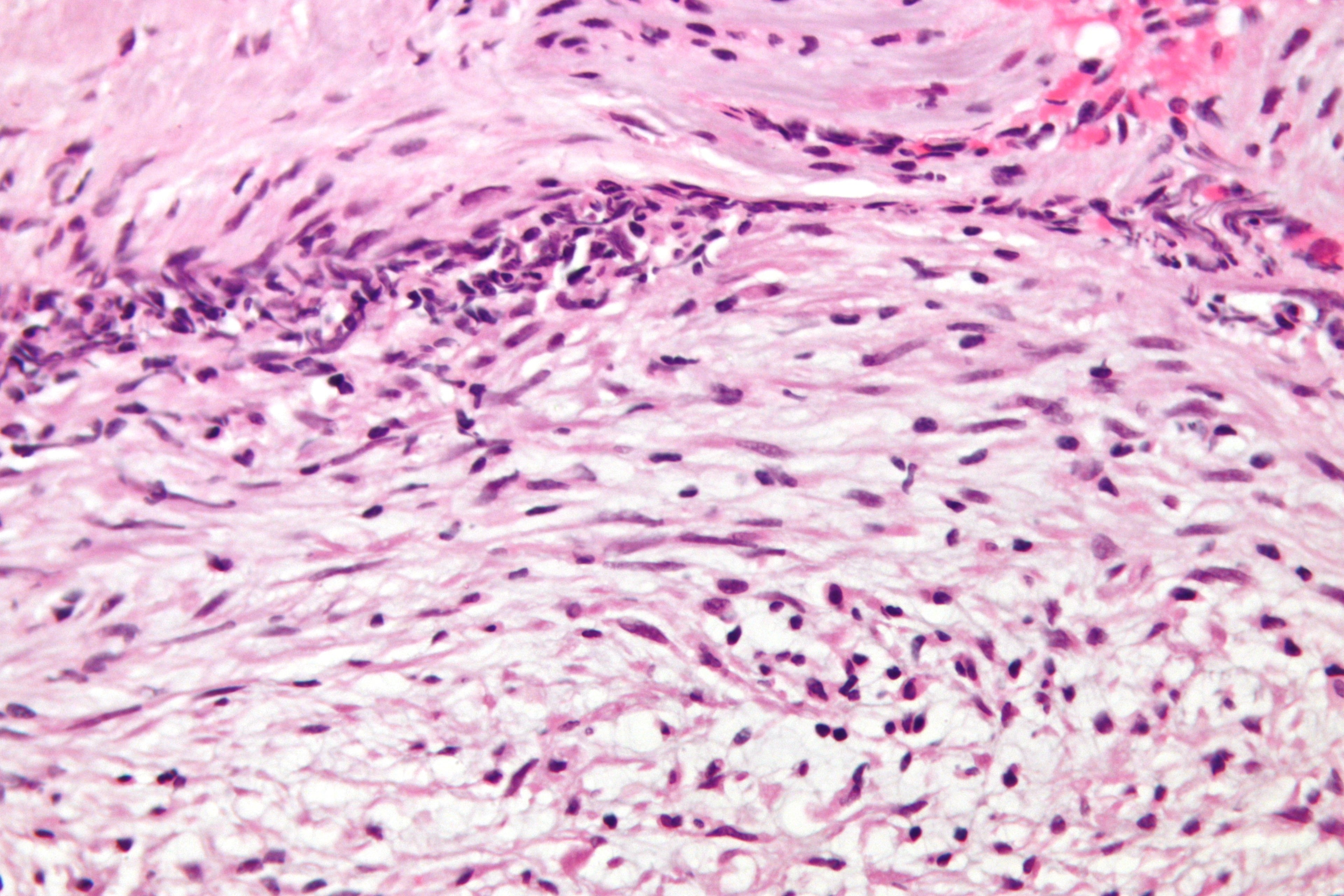
- HISTOLOGY shows plump, uniform SPINDLE (myofibroblast) cells arranged in a loose, feathery 'TISSUE-CULTURE' pattern with a myxoid stroma, scattered EXTRAVASATED red blood cells, and frequent but NORMAL (non-atypical) MITOSES - the lack of nuclear atypia and atypical mitoses helps distinguish it from a true sarcoma.
- Its BEHAVIOUR is benign: it does NOT metastasise, frequently REGRESSES SPONTANEOUSLY, and rarely recurs even after marginal/incomplete excision - so AGGRESSIVE treatment is unnecessary and harmful.
- The cardinal pitfall is OVERTREATMENT: because it mimics a sarcoma clinically and histologically, accurate DIAGNOSIS (biopsy with immunohistochemistry and USP6 testing) is essential so the patient can be managed CONSERVATIVELY - by observation (allowing spontaneous resolution) or a simple marginal EXCISION - rather than undergoing wide excision or radiotherapy intended for a malignant tumour.
- “Nodular fasciitis = benign self-limiting myofibroblastic proliferation - the classic PSEUDOSARCOMA (mimics sarcoma).
- “Rapidly growing small (under 3-4 cm) solitary nodule (volar forearm/trunk/head-neck); USP6 (MYH9-USP6) rearrangement supports it and argues against sarcoma - but is SHARED with myositis ossificans and ABC.
- “Histology: tissue-culture spindle cells, myxoid stroma, mitoses but NO atypia. Manage CONSERVATIVELY (spontaneous resolution / simple excision) - avoid overtreatment as sarcoma.
Rapid growth plus a cellular, mitotically active histology make nodular fasciitis look like a sarcoma - the classic 'pseudosarcoma'.
It is a self-limiting lesion with a USP6 rearrangement and no nuclear atypia that often regresses spontaneously - clonal in origin but transient in behaviour, so manage it conservatively and avoid overtreatment.
Clinical Features & the Pseudosarcoma Trap
Nodular fasciitis typically presents as a rapidly growing, small (usually under 3-4 cm), solitary and sometimes tender subcutaneous or fascial nodule, classically on the volar forearm, trunk, or - in children - the head and neck. The combination of rapid growth and a cellular, mitotically active histology makes it the classic 'pseudosarcoma', frequently misdiagnosed as a malignant soft-tissue tumour and subjected to unnecessary aggressive treatment. Recognising that a rapidly enlarging nodule can be this benign, self-limiting lesion - and confirming it before acting - is the key clinical point.
Reactive or Neoplastic? And What USP6 Does and Does Not Prove
Two questions here are asked precisely because the honest answers are more interesting than the textbook labels, and a candidate who gives the old answer to either sounds a decade out of date.
"Is nodular fasciitis reactive or neoplastic?" For most of its history it was taught as a reactive proliferation, often attributed to trauma, and the older name - pseudosarcomatous fasciitis - carries that assumption. The discovery of a recurrent USP6 gene rearrangement settled it the other way: the lesion is clonal, and a clonal proliferation is by definition a neoplasm. What makes it unlike other neoplasms is that it stops. The accepted description is a transient clonal neoplasm - grouped with its relatives as a USP6-associated neoplasm - and the mechanism proposed for the self-limitation is that the fusion drives a burst of proliferation that is not sustained, so the lesion grows fast, plateaus and involutes rather than progressing.
The correct answer is therefore: neoplastic in origin, benign in behaviour, and self-limiting by nature - which is exactly why a lesion can be genuinely clonal and still safe to watch. "Reactive" is the outdated term and "sarcoma" is the wrong end of the spectrum; the truth sits between them and is more useful than either.
"So does USP6 confirm the diagnosis?" Not on its own, and this is the more important correction, because USP6 rearrangement is shared across a family of lesions rather than being specific to nodular fasciitis:
- USP6 status
- Rearranged in the majority; MYH9::USP6 the commonest fusion
- What separates it from nodular fasciitis
- The reference lesion - tissue-culture pattern, small, fast, soft tissue
- USP6 status
- Rearranged in a SUBSET
- What separates it from nodular fasciitis
- ZONAL maturation with peripheral ossification and a lucent centre; a trauma history; radiographic evolution over weeks
- USP6 status
- Rearranged in about 70%
- What separates it from nodular fasciitis
- Arises in BONE, expansile with blood-filled cavities and fluid-fluid levels
- USP6 status
- Rearranged in a subset
- What separates it from nodular fasciitis
- Arises at a site of previous surgery or trauma - and is mistaken for recurrent tumour rather than for primary sarcoma
- USP6 status
- Rearranged in a subset
- What separates it from nodular fasciitis
- Site and morphology
A positive USP6 result therefore does two things well and one thing badly. It argues strongly against sarcoma, which is the question that actually matters clinically, and it supports the diagnosis in the right morphological context. It does not by itself distinguish nodular fasciitis from myositis ossificans or from an aneurysmal bone cyst - those are separated by site, radiology and morphology, not by the molecular test. Answering "USP6 confirms it" without that caveat invites the follow-up about myositis ossificans, which shares the abnormality. (The shared genetics are set out in Myositis Ossificans and Aneurysmal Bone Cyst.)
A negative result is also weaker than it looks. Fusion partners other than MYH9 exist, FISH does not detect every rearrangement, and a proportion of otherwise typical lesions test negative - so a negative USP6 in a lesion with classic morphology does not overturn the diagnosis.
Diagnosis & Management
- Diagnosis: clinical suspicion of a rapidly growing nodule, supported by imaging, and confirmed by biopsy with immunohistochemistry (myofibroblastic - SMA positive; negative for malignant markers) and USP6 molecular testing (FISH) - demonstrating the USP6/MYH9-USP6 rearrangement strongly supports the benign diagnosis and prevents misdiagnosis.
- Management: because it is self-limiting, options are observation (allowing spontaneous resolution, especially in children and cosmetically sensitive sites) or simple marginal EXCISION if symptomatic or diagnostically uncertain; intralesional corticosteroid is an alternative.
- Avoid overtreatment: do NOT perform a wide excision or give radiotherapy intended for sarcoma; recurrence is rare even after incomplete excision.
- Follow-up: reassure, and review to confirm resolution/no recurrence.
What "observe it" actually involves. Observation is a management plan with conditions attached, not a decision to do nothing, and it is only safe once the diagnosis is secure on morphology and molecular testing. Three things make it work:
- A defined starting point. Record the size in two dimensions, ideally with ultrasound rather than a clinical estimate, so that "smaller" is a measurement rather than an impression. Photograph a cutaneous lesion.
- Planned review rather than open-ended reassurance. Bring the patient back to re-measure. A lesion that is stable or shrinking is behaving as expected and can continue to be watched; the interval is a clinical judgement, but the review must be booked rather than left to the patient to request.
- Explicit criteria that end observation, given to the patient as well as recorded. Observation stops and the case is reassessed - with repeat imaging, review of the original material, and referral through a sarcoma pathway if not already done - if the lesion continues to enlarge beyond the expected early growth phase, exceeds the size expected of this diagnosis, becomes fixed to deep structures, develops new pain or neurological symptoms, or simply fails to regress over a period the clinician judges reasonable.
The safeguard in all of this is that the alternative diagnoses do not behave this way: a sarcoma does not involute. Continued growth is the finding that must never be attributed to a lesion whose defining feature is that it stops.
Recurrence should change your mind, not just your plan. Recurrence after excision is genuinely rare, and its rarity is the point: a lesion that recurs should prompt review of the original histology by a specialist soft-tissue pathologist rather than simply a second excision, because the likeliest explanation for a recurring "nodular fasciitis" is that the first diagnosis was wrong.
The single most important message is that nodular fasciitis is BENIGN and self-limiting, yet its rapid growth and cellular histology lead to it being mistaken for a sarcoma and overtreated. The safeguard is accurate pathological diagnosis - including USP6 molecular testing - before any aggressive treatment, and conservative management thereafter. Equally, a rapidly growing soft-tissue mass should never be assumed benign without proper assessment, so any soft-tissue lump that is large (over about 5 cm), deep, or enlarging should be referred and worked up through a sarcoma pathway, with the diagnosis of nodular fasciitis confirmed on biopsy/USP6 rather than presumed.
The Pseudosarcoma Family and the Spindle-Cell Differential
Nodular fasciitis is the classic pseudosarcoma, but it is not the only one, and knowing which other benign mimics and which true sarcomas sit alongside it is what turns a diagnosis into a differential. The unifying discriminator is that nodular fasciitis and the other benign pseudosarcomas have mitoses but NO nuclear atypia, whereas true sarcomas show atypia and atypical mitoses.
- Discriminating clue
- Rapid, small; tissue-culture spindle cells, mitoses but NO atypia; USP6 (MYH9-USP6)
- What it means for management
- Observation or simple excision - never wide margins
- Discriminating clue
- Reactive, benign; large ganglion-like giant cells; older adults
- What it means for management
- (benign reactive - conservative)
- Discriminating clue
- Pressure/immobility sites (elderly); zonal fibrinoid necrosis
- What it means for management
- (benign reactive - conservative)
- Discriminating clue
- Trauma history; ZONAL maturation with peripheral ossification
- What it means for management
- Benign - let it mature; biopsy or excise early and the immature centre mimics sarcoma
- Discriminating clue
- Infiltrative, locally aggressive, recurs; nuclear beta-catenin (CTNNB1)
- What it means for management
- Benign but locally aggressive - does not metastasise, yet recurs after excision; increasingly observed or treated medically rather than resected
- Discriminating clue
- Nuclear ATYPIA + atypical mitoses; herringbone / CD34+ storiform / curvilinear vessels
- What it means for management
- Malignant - staging, planned biopsy through a resectable tract, and wide excision at a sarcoma unit. This is the one the others must not be mistaken for
Variants and Sites of Nodular Fasciitis
Beyond the common subcutaneous and fascial sites there are recognised variants by depth and location - each still benign, USP6-driven and managed conservatively, but each capable of alarming if not recognised.
Subcutaneous (the commonest), then intramuscular and fascial forms. Classic sites are the volar forearm and trunk, and the head and neck in children.
- Intravascular fasciitis - arising in or around a vessel wall (can alarm further).
- Cranial fasciitis - infants/young children, involving the scalp and outer skull and able to erode the calvarium (do not mistake for an aggressive lesion).
- Intra-articular nodular fasciitis, and ossifying fasciitis (with metaplastic bone, overlapping myositis ossificans).
Whatever the depth or site - subcutaneous, intramuscular, intravascular, or cranial fasciitis eroding an infant's skull - it remains a benign, USP6-driven, self-limiting lesion managed conservatively. Recognising the variant is what prevents overtreatment in an unusual location.
Mnemonics & Memory Aids
PSEUDO
Hook:Nodular fasciitis is the PSEUDO-sarcoma: benign, USP6, self-resolving.
FAST but SAFE
Hook:Nodular fasciitis grows FAST but is SAFE (benign) - confirm with USP6.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a small, rapidly growing nodule in the forearm. How would the diagnosis of nodular fasciitis be made, and why does it matter?”
“Why is nodular fasciitis called a 'pseudosarcoma', and how do you avoid overtreating it while not missing a real sarcoma?”
Nature
- Benign, self-limiting myofibroblastic proliferation - CLONAL/neoplastic, not reactive
- The classic PSEUDOSARCOMA (benign but mimics sarcoma)
- Does not metastasise; often regresses spontaneously
Clinical
- Rapidly growing, small (usually under 3-4 cm), solitary nodule
- Volar forearm, trunk; head/neck in children
- Rapid growth is the feature that raises malignancy concern
Histology & genetics
- Plump spindle (myofibroblast) cells in a tissue-culture pattern
- Myxoid stroma, extravasated red cells, mitoses but NO atypia
- USP6 rearrangement (MYH9-USP6 fusion) - SUPPORTS the diagnosis and argues against sarcoma, but is shared with myositis ossificans and primary ABC
Management
- Confirm with biopsy + USP6 (avoid misdiagnosis as sarcoma)
- Conservative: observation (spontaneous resolution) or simple excision
- Avoid wide excision/radiotherapy; recurrence rare; but never presume benign without work-up
Evidence & Key Studies
Breast nodular fasciitis: a case report and review (USP6 FISH and pseudosarcoma diagnosis)
- Nodular fasciitis is a benign soft-tissue lesion that can occur anywhere and clinically mimics a malignant tumour.
- Accurate diagnosis with immunohistochemistry or USP6 FISH analysis is critical to prevent misdiagnosis and overtreatment.
- Simple excision was the definitive treatment, with histology confirming the benign diagnosis.
Clinicopathological characteristics and favourable prognosis of paediatric cutaneous nodular fasciitis
- Cutaneous nodular fasciitis is a benign myofibroblastic proliferation commonly misdiagnosed as malignancy due to rapid growth and histology, with a predilection for the head and neck in children.
- USP6 rearrangement (particularly MYH9-USP6 fusion) was present in the majority, and spontaneous resolution occurred in non-surgically managed cases.
- Screening for USP6 rearrangement and conservative management avoid overtreatment, especially in cosmetically sensitive areas.
USP6-associated neoplasm: postoperative spindle cell nodule and the transient clonal neoplasm concept
- Seven postoperative spindle cell nodules - all arising after previous surgery or trauma - were highly cellular and mitotically active with NO cytological atypia, pleomorphism or aberrant mitoses.
- SMA showed the tram-track pattern in every case and ALK was entirely negative; USP6 rearrangement was confirmed by FISH in all seven, with an MYH9::USP6 fusion identified in only one.
- Proposes grouping these under 'USP6-associated neoplasm', signifying a TRANSIENT CLONAL NEOPLASTIC lesion - the framing that replaces the older 'reactive' description of nodular fasciitis.
- Illustrates that USP6 rearrangement extends beyond nodular fasciitis, so the test supports rather than establishes the specific diagnosis.
The benign-but-malignancy-mimicking nature, the diagnostic value of USP6 FISH and the risk of overtreatment come from the cited Cheng case/review, and the USP6/MYH9-USP6 rearrangement with spontaneous resolution and conservative management from the cited Zhao paediatric series. The myofibroblastic biology, the tissue-culture histology and the pseudosarcoma concept are standard, well-established soft-tissue-pathology teaching. The transient-clonal-neoplasm framing, the tram-track SMA pattern and the extension of USP6 rearrangement beyond nodular fasciitis come from the cited Sun series. That USP6 is shared with myositis ossificans and with primary aneurysmal bone cyst - which is why it supports rather than establishes the diagnosis - follows Myositis Ossificans and Aneurysmal Bone Cyst. (See also Soft Tissue Masses and Sarcoma Referral, Desmoid Tumour, Fibrosarcoma, Dermatofibrosarcoma Protuberans and Myxofibrosarcoma.)