Ogden Classification of Tibial Tubercle Avulsion Fractures
A Type III fracture is intra-articular and requires ORIF for anatomic reduction regardless of displacement. A Type IIA or IIB fracture with displacement also needs fixation. The examiner expects you to state the classification clearly, explain the Osgood-Schlatter connection, and describe your fixation strategy. Watch for compartment syndrome — the anterior tibial recurrent artery runs posterior to the tibial tubercle and can bleed into the anterior compartment, especially with Type III patterns.
The Ogden Classification
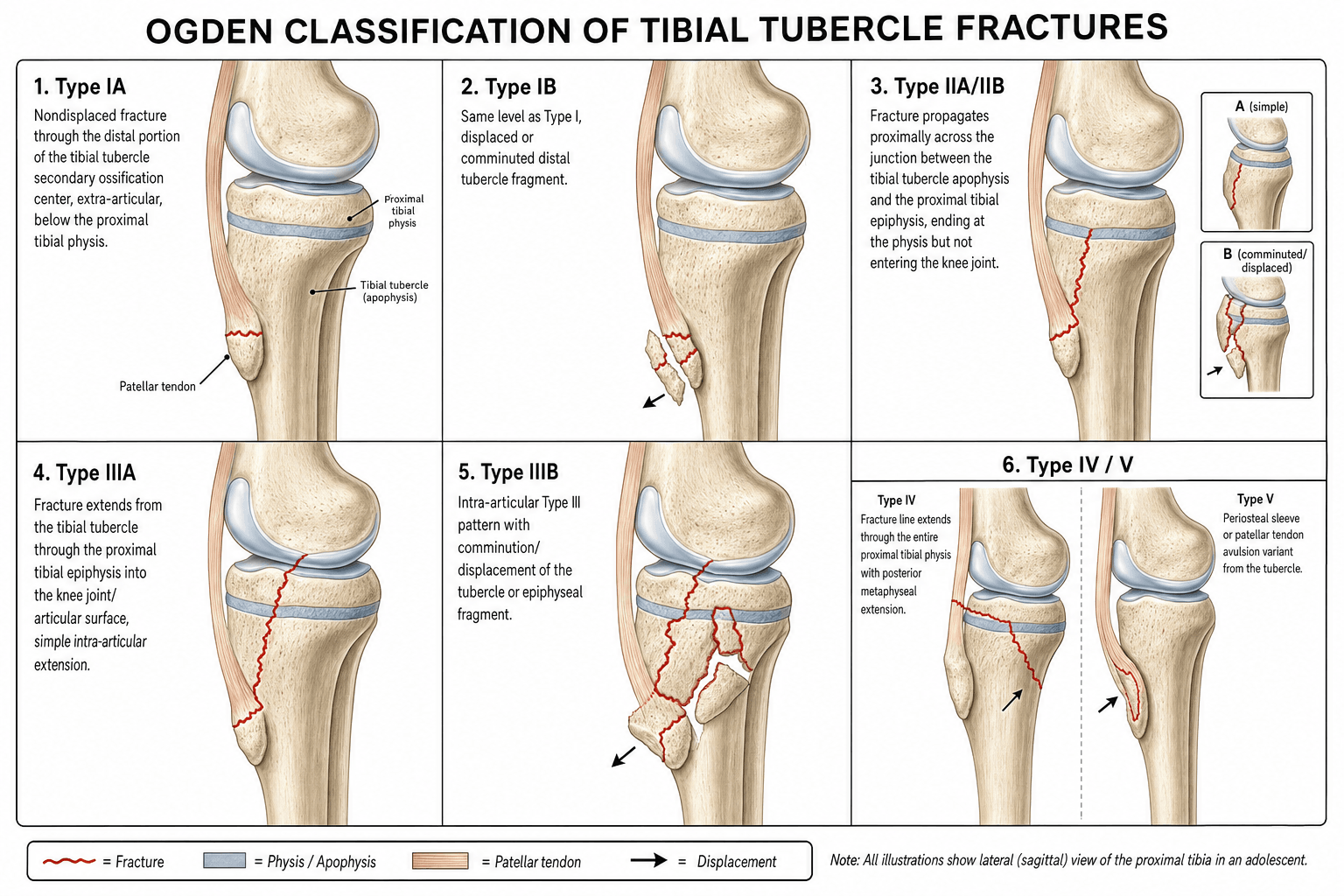

The Ogden classification (Ogden, 1980) stratifies tibial tubercle avulsion fractures by how far the fracture line extends proximally from the secondary ossification center of the tubercle into the epiphysis and joint. The classification correlates directly with fracture severity, surgical urgency, and prognosis.
- Fracture Extent
- Through the secondary ossification center only (the tubercle fragment is cartilaginous and separated from the epiphysis)
- A — Undisplaced
- Long leg cast in full extension, 4 to 6 weeks
- B — Displaced
- Closed reduction and casting if achievable; ORIF if reduction is unstable or lost
- Fracture Extent
- Extends across the junction between the secondary and primary ossification centers into the proximal tibial epiphysis (larger fragment including bone)
- A — Undisplaced
- Long leg cast in full extension, 4 to 6 weeks; close monitoring for late displacement
- B — Displaced
- ORIF with cannulated screws, anterior-to-posterior direction; may need plate supplementation
- Fracture Extent
- Extends through the epiphysis into the knee joint (intra-articular, involving the tibial plateau surface)
- A — Undisplaced
- Low threshold for ORIF; cast if truly undisplaced and joint surface is congruent on CT
- B — Displaced
- ORIF mandatory: anatomic articular reduction, joint inspection, cannulated screw fixation with possible buttress plate
Isolated tubercle · Into epiphysis · Into jointThe three core types — fracture extent
Hook:Each type is A (undisplaced) or B (displaced); the further proximal the crack travels, the larger the fragment and the greater the surgical challenge. (Later additions: IV = through the whole physis, V = periosteal sleeve.)
Beyond the classic three: later modifications added Type IV (the fracture propagates posteriorly through the entire proximal tibial physis, behaving like a Salter-Harris injury of the whole proximal tibia) and Type V (a periosteal-sleeve or combination pattern). The original Ogden I–III remains the exam-standard, but recognise IV/V if shown a fracture that exits through the posterior physis rather than the tubercle.
The Type II fragment is larger than the Type I fragment because it includes bone from the proximal tibial epiphysis, not just the secondary ossification centre. The Type III fragment is the largest because it extends to the articular surface. A bigger fragment means more potential for instability and more surgical challenge.
Osgood-Schlatter Disease and the Fracture Pattern

Osgood-Schlatter disease is a chronic traction apophysitis at the tibial tubercle caused by repetitive quadriceps loading during the adolescent growth spurt. The same biomechanical mechanism that produces Osgood-Schlatter disease predisposes to an acute tibial tubercle avulsion fracture, and the stage of apophyseal maturation determines the fracture pattern.
Mature apophysis → more proximal fractureOsgood-Schlatter and fracture pattern
Hook:The acute avulsion is the end of the Osgood-Schlatter spectrum — chronic overload weakens the tubercle, then a single violent quadriceps contraction avulses it.
Key points for the exam:
- A history of Osgood-Schlatter disease means the apophysis is at least partially fused, making Type II or III more likely than Type I.
- Conversely, a patient with no prior Osgood-Schlatter symptoms and a younger skeletal age (12 to 14 years) is more likely to sustain a Type I fracture through the still-cartilaginous secondary centre.
- The chronic inflammation and fragmentation of the tubercle in Osgood-Schlatter disease may leave the bone weaker structurally, lowering the force threshold for an acute avulsion.
- The fracture represents an acute failure of a structure that has been weakened by chronic overload — the end of a spectrum, not a separate pathology.
A violent adolescent quadriceps contraction can fail at several points; examiners expect you to localise it and to know the dangerous mimic:
- Patellar sleeve avulsion fracture — the patellar-side equivalent: an osteochondral "sleeve" pulled off the inferior pole of the patella by the same mechanism. Like the tubercle fragment it is mostly cartilage, so radiographs underestimate it (only a small fleck shows); look for patella alta and loss of active extension — displaced sleeves need ORIF.
- Proximal tibial physeal (Salter-Harris) fracture — the dangerous mimic to separate from a tubercle avulsion: this is a fracture through the whole proximal tibial physis, and its key hazard is vascular — the popliteal artery is tethered behind the proximal tibia and can be injured (contrast with the tubercle avulsion, where it is the anterior tibial recurrent artery / anterior compartment that is at risk). Ogden Type IV blurs into this pattern, so always assess the distal pulses and the whole physis.
- Ununited Osgood-Schlatter ossicle — a chronic painful ossicle at the tubercle without an acute avulsion (no extensor lag, no acute displacement).
- Associated injuries to actively seek (especially Type III) — patellar or quadriceps tendon avulsion, collateral or cruciate ligament tears, and meniscal damage.
The unifying point: examine and image to find where the extensor mechanism failed — tubercle, inferior patella (sleeve), the tendon, or the whole proximal tibial physis — because the proximal-tibial-physeal pattern carries a popliteal-artery risk the tubercle avulsion does not.
Treatment by Classification
- Treatment
- Long leg cast in full extension for 4 to 6 weeks, then progressive knee mobilisation
- Key Points
- Repeat radiographs at 1 to 2 weeks to exclude late displacement; most common pattern in younger adolescents
- Treatment
- ORIF if closed reduction fails or is unstable; closed reduction and casting if reducible and stable
- Key Points
- Closed reduction in extension; if the fragment stays reduced, cast; if not, open fixation with cannulated screws from anterior to posterior
- Treatment
- Long leg cast in full extension for 4 to 6 weeks; close monitoring for late displacement
- Key Points
- Larger fragment than Type I — higher load on the repair; consider CT to confirm joint surface integrity
- Treatment
- ORIF with cannulated screws directed anterior to posterior, crossing the fracture line as lag screws
- Key Points
- Supplement with tension band wiring or a small anterior plate if fragment comminution makes screw hold inadequate; protect the physis
- Treatment
- Low threshold for ORIF; consider MRI or CT to confirm articular congruity
- Key Points
- Even minimal displacement of an intra-articular fragment may warrant fixation; if truly undisplaced and congruent, cast in extension
- Treatment
- ORIF mandatory: anatomic reduction of the articular surface under direct vision, joint inspection for loose bodies
- Key Points
- Lateral parapatellar or direct anterior approach; cannulated lag screws plus possible buttress plate; washout the joint; assess for meniscal injury
All displaced tibial tubercle fractures (Types IB, IIB, IIIB) require fixation. The extensor mechanism is disrupted and the patellar tendon is pulling the fragment proximally. A displaced fracture treated in a cast alone will heal in a displaced position, producing patella alta, an extensor lag, and anterior knee pain. Fixation restores extensor mechanism continuity and allows early mobilisation.
Surgical technique principles:
- Patient supine, tourniquet on the upper thigh
- Direct anterior longitudinal incision over the tibial tubercle; for Type III, extend with a lateral parapatellar approach to access the joint
- Evacuate the haemarthrosis and inspect for loose bodies and meniscal injury (Type III)
- Reduce the fragment anatomically under direct vision; confirm articular congruity
- Fixation: 4.0 mm or 4.5 mm cannulated lag screws inserted anterior-to-posterior, engaging the posterior cortex; add washers if the anterior cortex is comminuted
- In Type III, consider a small buttress or anti-glide plate anteriorly for additional stability
- Assess range of motion and extensor mechanism continuity on table
- Post-operative: long leg cast or hinged brace initially, then progress to active mobilisation at 2 to 3 weeks

Clinical Presentation and Examination
Tibial tubercle fractures occur almost exclusively in adolescent males aged 12 to 16 years during the terminal phase of proximal tibial physeal closure. The injury is caused by a sudden violent extension force — typically jumping, sprinting, or landing from a height — that overcomes the tensile strength of the patellar tendon insertion into the partially fused apophysis.
On examination:
- Swelling and marked tenderness directly over the tibial tubercle
- A palpable gap or step between the displaced tubercle fragment and the proximal tibia in displaced fractures
- Inability to perform an active straight-leg raise or extend the knee against gravity (extensor mechanism disrupted)
- A knee effusion is present in Type III fractures (haemarthrosis from the intra-articular component) and may also be seen in Type II
- In Type I fractures, the extensor lag may be subtle and the clinical picture can mimic a bad episode of Osgood-Schlatter disease
TACKExamination checklist
Hook:TACK the four checks: tubercle, active extension, compartments, knee effusion — the compartment check is the one that saves the leg.
A normal extensor mechanism on examination does not exclude a Type I undisplaced fracture — the extensor lag may be minimal. Maintain a high index of suspicion in any adolescent with acute-onset tubercle pain after a jumping or landing injury, regardless of extension strength.
The lateral film makes the diagnosis, but the high-yield teaching is what it MISSES:
- The view: a true lateral with slight internal rotation best profiles the tubercle (the tuberosity sits slightly lateral, so an externally-rotated/oblique film can hide it); add an AP, and a contralateral comparison film is useful in the immature knee.
- The pitfall — radiographs UNDERESTIMATE the fragment: in the younger adolescent much of the avulsed fragment is still unossified cartilage, so the bony fleck seen on plain film is smaller than the true fragment and the real displacement (and any joint or sleeve extension) can be missed. An apparently trivial fleck can be a large displaced cartilaginous avulsion — this is the classic exam trap.
- MRI (or ultrasound) reveals the true cartilaginous fragment and the extensor-mechanism/soft-tissue injury; CT is used for Type III to quantify the articular step and comminution and plan fixation (the systematic-review evidence supports advanced imaging for intra-articular patterns).
- Patella alta on the lateral (a proximally migrated patella, e.g. a raised Insall-Salvati ratio) confirms extensor-mechanism displacement and the need for fixation.
- A lipohaemarthrosis (fat–fluid level) signals an intra-articular (Type III) fracture.
Complications and Pitfalls
- Compartment syndrome is the most feared complication. The anterior tibial recurrent artery passes posterior to the tibial tubercle and can be torn by the fracture displacement, causing a haematoma in the anterior compartment. Monitor compartment pressures hourly for the first 24 hours in all operated patients and maintain a low threshold for fasciotomy.
- Malunion with patella alta. A displaced fracture that heals in a displaced position effectively lengthens the patellar tendon, producing patella alta, reduced quadriceps mechanical advantage, and chronic anterior knee pain. Prevented by anatomic reduction and fixation.
- Extensor mechanism weakness. Incomplete reduction or fixation failure leads to a persistent extensor lag. The patient cannot straight-leg raise against gravity and has difficulty climbing stairs or rising from a chair.
- Knee stiffness. Prolonged immobilisation, especially in Type III fractures where the joint capsule is violated, produces arthrofibrosis. Early mobilisation after stable fixation reduces this risk.
- Prominent hardware. Cannulated screw heads and washers are subcutaneous over the tibial tubercle and may be symptomatic, particularly in thin patients. Hardware removal is commonly required once union is confirmed (usually 6 to 9 months).
- Premature physeal closure. Violating the proximal tibial physis with screws or hardware placed too proximally can arrest growth on the anterior tibial tubercle portion of the physis, producing a progressive recurvatum deformity. Place fixation distal to the physis whenever possible.
- Re-fracture. Return to sport too early or hardware removal before solid bony union risks a repeat avulsion. Wait for radiographic union and clinical resolution of tenderness before clearing sport.
Viva practice
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 14-year-old male footballer presents after landing awkwardly from a jump. He felt a sudden pop at the front of his knee and cannot extend the knee. Examination shows a swollen, tender tibial tubercle with a palpable step and a moderate knee effusion. Radiographs show a displaced fracture of the tibial tubercle with a fragment that appears to extend to the articular surface of the tibia. How would you classify, investigate, and manage this?”
“A 13-year-old boy presents with acute-onset pain and swelling over the tibial tubercle after sprinting. He has a history of Osgood-Schlatter disease. Radiographs show an undisplaced crack through the tibial tubercle that appears to cross into the proximal tibial epiphysis but does not reach the joint. What is the classification, what does the Osgood-Schlatter history tell you, and how would you manage him?”
Exam cheat sheet
The three types (each with A/B subtypes)
- Type I: fracture through the secondary ossification centre only (isolated tubercle fragment)
- Type II: fracture extends across the secondary-to-primary junction into the proximal tibial epiphysis
- Type III: fracture extends into the knee joint (intra-articular) — always ORIF
- A subtype: undisplaced (cast immobilisation); B subtype: displaced (ORIF)
Osgood-Schlatter and fracture pattern
- Chronic traction apophysitis predisposes to acute avulsion fracture
- Mature or fused apophysis directs the fracture proximally (Type II or III)
- Immature cartilaginous apophysis produces a Type I pattern
- A patient with known Osgood-Schlatter is more likely to sustain Type II or III
Treatment principles
- Undisplaced (all A subtypes): long leg cast in full extension, 4 to 6 weeks
- Displaced (all B subtypes): ORIF with cannulated lag screws anterior-to-posterior
- Type III: ORIF mandatory regardless of displacement — anatomic articular reduction, joint inspection
- Compartment monitoring for 24 hours post-injury or post-op
Complications
- Compartment syndrome from anterior tibial recurrent artery injury (most feared)
- Malunion with patella alta and extensor lag
- Premature physeal closure from hardware placed across the physis
- Prominent hardware requiring secondary removal
Evidence
Fractures of the tibial tuberosity in adolescents
- Reviewed 14 adolescents (15 tibial-tuberosity physeal fractures) and devised a modified classification emphasising intra-articular extension and tuberosity comminution.
- Surgical indications were anterosuperior displacement of a fragment and extension through the proximal tibial ossification centre into the joint; closed or open reduction gave satisfactory results.
- Noted an increased association with pre-existing Osgood-Schlatter disease, and that genu recurvatum is unlikely because most injuries occur as the physis is normally closing.
Type III fractures of the tibial tubercle in adolescents
- 15 surgically treated Type III avulsions reviewed at a mean of 9.6 years; six had a history of Osgood-Schlatter disease.
- All but one healed; complications included one compartment syndrome (with tibialis anterior avulsion), one refracture, and bursitis over prominent screws requiring removal in five.
- No angular or recurvatum deformity; a 1.0–1.8 cm leg-length discrepancy occurred in four patients (two over-, two under-growth).
Outcomes and complications of tibial tubercle fractures in pediatric patients: a systematic review
- Systematic review of 23 studies (336 fractures, mean age 14.6 years); Type III was the most common pattern (50.6%).
- Associated-injury rate 4.1% (highest in Type III); compartment syndrome in 3.57%; fracture healing in 99.4%; return to pre-injury activity and knee ROM ~98% regardless of type.
- Overall complication rate 28.3% — most often implant removal for bursitis (55.8%), then tenderness/prominence and refracture.
According to PubMed, the classification is from Ogden, Tross & Murphy 1980 (J Bone Joint Surg Am 1980;62(2):205-15; PMID 7358751). Type III outcomes are from Wiss et al. 1991 (DOI 10.1097/00005131-199112000-00015), the compartment-syndrome/anterior-tibial-recurrent-artery association from Pape et al. 1993 (PMID 8403649), a management review from McKoy & Stanitski 2003 (DOI 10.1016/s0030-5898(02)00061-5), and the systematic review (Type III most common 50.6%, compartment syndrome 3.57%, complications 28.3%) from Pretell-Mazzini et al. 2016 (DOI 10.1097/BPO.0000000000000488).