Type II High Risk | Age Determines Treatment | Collar vs Fusion
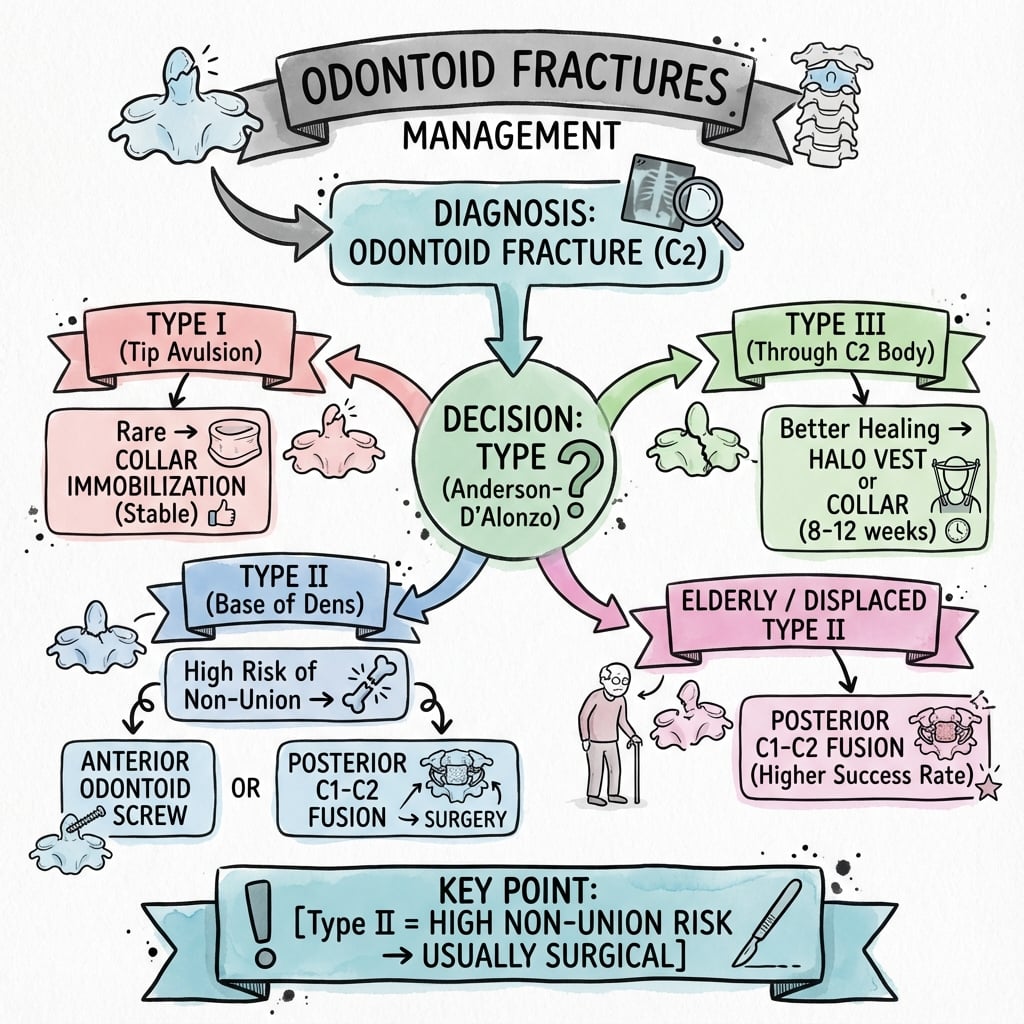
- Type II is most common (60%) and most problematic (40% nonunion with collar)
- Type III heals well with collar - fracture into cancellous C2 body
- Elderly Type II - consider primary posterior C1-C2 fusion (Harms/Magerl)
- Anterior odontoid screw preserves rotation for acute displaced Type II (young)
- Transverse ligament integrity determines stability
- “Type II is at watershed blood supply zone - high nonunion risk
- “Age over 65, displacement over 5mm, angulation over 10° = surgical factors
- “Harms technique (C1 lateral mass + C2 pedicle screws) is gold standard posterior
- “Anterior screw contraindicated in Type IIA, barrel chest, posterior oblique line
Type II (waist) has 30-40% nonunion rate with collar. Watershed blood supply at dens base. Most controversial treatment decisions revolve around this type.
Type III extends into C2 body = cancellous bone with good blood supply. 85% union with rigid collar. Usually non-operative unless significant displacement.
Elderly (over 65) have higher nonunion with collar alone. Strong consideration for primary posterior C1-C2 fusion. Balance surgical risk vs nonunion morbidity.
Anterior odontoid screw: Preserves C1-C2 rotation, for acute Type II. Posterior C1-C2 fusion (Harms): For nonunion, elderly, Type IIA. Sacrifices rotation.
- Pattern
- Tip avulsion
- Union Rate (Collar)
- 95%+
- Treatment
- Collar 6-8 weeks
- Pattern
- Waist/base
- Union Rate (Collar)
- 60%
- Treatment
- Anterior screw or collar
- Pattern
- Waist/base
- Union Rate (Collar)
- 40-50%
- Treatment
- Posterior C1-C2 fusion
- Pattern
- Comminuted
- Union Rate (Collar)
- Poor
- Treatment
- Posterior fusion (no screw)
- Pattern
- Into C2 body
- Union Rate (Collar)
- 85%+
- Treatment
- Collar 10-12 weeks
TIP-WAIST-BODYAnderson-D'Alonzo Types
Hook:TIP is rare, WAIST is problematic, BODY heals well!
DOGSType II Surgical Factors
Hook:If the patient has DOGS factors, consider surgery!
BARRELAnterior Screw Contraindications
Hook:BARREL chest or reverse oblique = no anterior screw!
ADITransverse Ligament Assessment
Hook:ADI over 3mm = TAL is not okay!
Overview and Epidemiology
Odontoid fractures have a bimodal age distribution:
- Young adults: High-energy trauma (MVA, sports)
- Elderly: Low-energy falls, osteoporotic bone
In the elderly, odontoid fractures are the most common cervical fracture pattern. Treatment decisions must balance surgical risk against nonunion morbidity.
- Young: High-energy - MVA, diving, sports
- Elderly: Low-energy falls
- Hyperflexion: Anterior displacement
- Hyperextension: Posterior displacement
- Rotational component: May be present
- Head injury: Common with high-energy
- Other C-spine fractures: 10-20%
- Vertebral artery injury: Rare but assess
- Thoracolumbar fractures: Check whole spine
Anatomy and Biomechanics
C2 (Axis) Anatomy
The C2 vertebra (axis) is unique:
- Odontoid process (dens) projects superiorly into the ring of C1
- Articulates with anterior arch of C1 (atlas)
- Held by transverse ligament posteriorly
- 50% of cervical rotation occurs at C1-C2
Blood Supply
The base of the dens (Type II level) is a watershed zone between:
- Ascending arteries from C2 body (supply base)
- Apical arcade and posterior descending (supply tip)
This explains the high nonunion rate in Type II fractures - poor blood supply at fracture site.
- Source
- Apical arcade
- Implication
- Type I heals well
- Source
- Watershed zone
- Implication
- Type II high nonunion
- Source
- Vertebral body vessels
- Implication
- Type III good healing
Key Ligaments
- Primary stabilizer of C1-C2
- Holds dens against C1 anterior arch
- Rupture = atlantoaxial instability
- Check ADI on lateral X-ray/CT
- ADI over 3mm = TAL injury
- Connect dens tip to occipital condyles
- Limit axial rotation
- Type I fractures = alar ligament avulsion
- Check for occipitocervical instability
Rule of Thirds
At the C1 level, the spinal canal is divided:
- 1/3 odontoid process
- 1/3 spinal cord
- 1/3 free space (CSF)
This "physiological reserve" explains why neurological injury is relatively rare in odontoid fractures despite significant displacement - there is room for the cord to escape.
Classification Systems
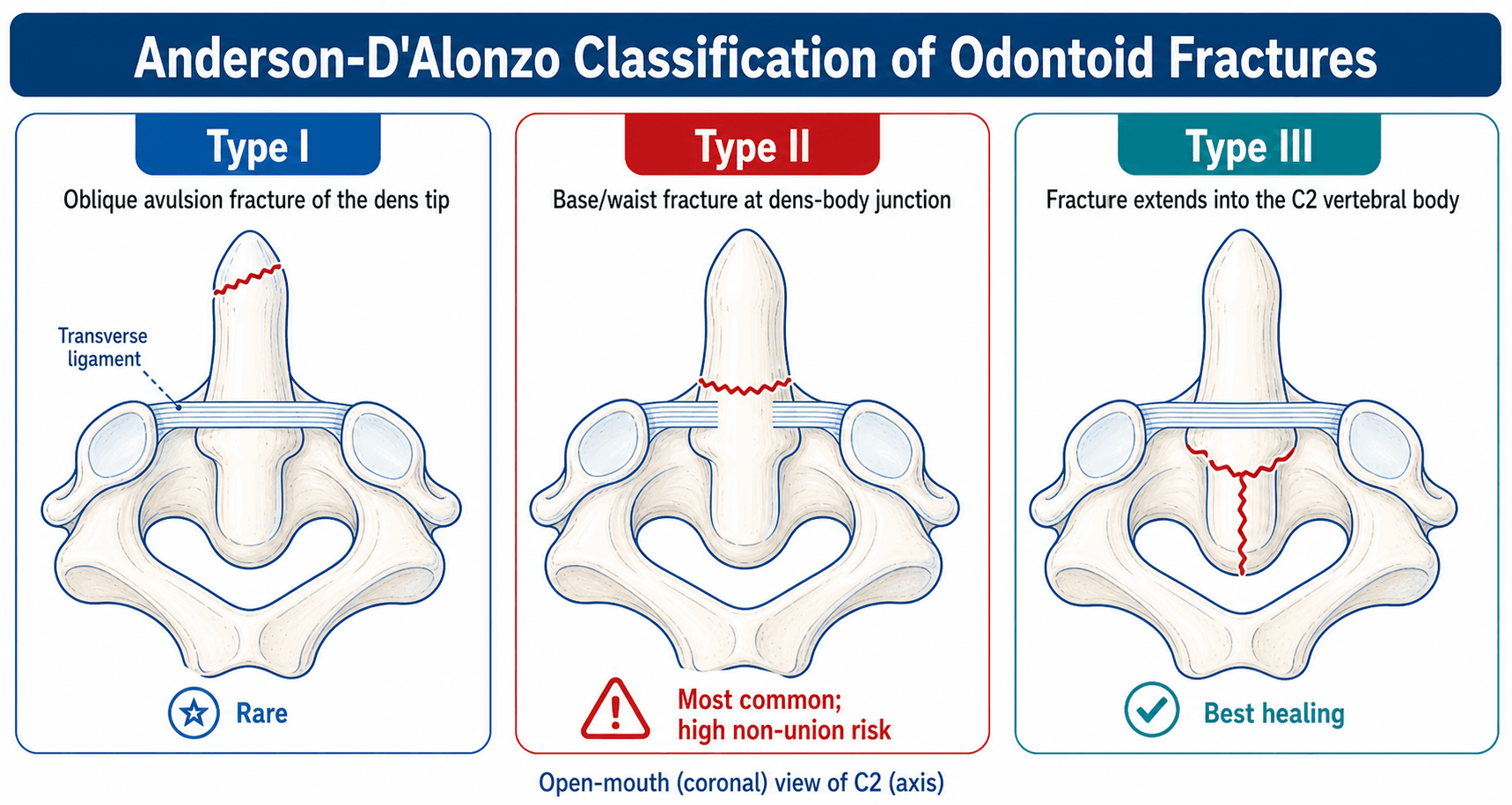
Anderson-D'Alonzo Classification (1974)
The standard classification for odontoid fractures:
- Location
- Tip avulsion
- Frequency
- 5%
- Stability
- Stable
- Treatment
- Collar 6-8 weeks
- Location
- Base of dens
- Frequency
- 60%
- Stability
- Unstable
- Treatment
- Collar vs surgery
- Location
- Type II + comminution
- Frequency
- Rare
- Stability
- Very unstable
- Treatment
- Posterior fusion
- Location
- Into C2 body
- Frequency
- 35%
- Stability
- Often stable
- Treatment
- Collar 10-12 weeks
Classification Imaging Examples

Clinical Assessment
- Mechanism: MVA vs fall (age-dependent)
- Neck pain: Posterior or suboccipital
- Neurological symptoms: Rare (cord has space)
- Head injury: Common with high-energy
- Previous neck problems: Degenerative disease
- Immobilization: Maintain until cleared
- Palpation: C2 spinous process tenderness
- Neurology: Full cord and root exam
- Vascular: Rarely affected
- Other injuries: Full trauma survey
Despite significant displacement, neurological injury is uncommon (less than 10%) because of:
- Large spinal canal at C1-C2 (rule of thirds)
- Gradual displacement allows cord adaptation
- If neuro deficit present, suspect cord injury - urgent decompression may be needed
Red Flags
Urgent features requiring immediate attention:
- Neurological deficit (rare but urgent)
- Rapidly progressive symptoms
- Respiratory compromise (high cord injury)
- Vascular symptoms (vertebral artery)
- Polytrauma with hemodynamic instability
Investigations
Imaging Protocol
CT is gold standard for diagnosis. Shows fracture type, displacement, angulation, and comminution. Sagittal reconstructions essential for fracture line orientation (Grauer classification).
MRI for transverse ligament and other soft tissue assessment. Required if ADI increased or instability suspected. Also shows cord edema if neurological concerns.
Only when fracture healed or stability confirmed. Assess for atlantoaxial instability. Never in acute setting with unstable fracture.
Key Measurements
- Normal
- Under 3mm (adult)
- Abnormal
- Over 3mm
- Significance
- TAL rupture
- Normal
- 0
- Abnormal
- Over 5mm
- Significance
- Surgical indication
- Normal
- 0
- Abnormal
- Over 10°
- Significance
- Surgical indication
- Normal
- Over 13mm
- Abnormal
- Under 13mm
- Significance
- Cord compression risk
CT: Best for bony detail, fracture classification, surgical planning MRI: Required for TAL integrity, cord assessment, and if CT findings don't explain symptoms
Always get CT first - MRI alone may miss subtle fractures.
Differential Diagnosis
The radiographic appearance of the dens can be deceptive. Several entities mimic or coexist with an acute odontoid fracture and must be actively distinguished, because the management differs substantially.
- Distinguishing Feature
- Sharp lucent line at dens base, soft-tissue swelling
- Clue on Imaging
- Cortical disruption, prevertebral haematoma, marrow oedema on STIR
- Pitfall
- Best diagnostic standard
- Distinguishing Feature
- Smooth corticated ossicle, hypertrophied anterior C1 arch
- Clue on Imaging
- Rounded margins, no oedema, often wide gap
- Pitfall
- Mistaken for acute nonunion - it is chronic
- Distinguishing Feature
- Small ossicle above a normal dens body
- Clue on Imaging
- Above the level of the transverse ligament, stable
- Pitfall
- Usually incidental, not unstable
- Distinguishing Feature
- Apparent lucency from overlapping arches or teeth
- Clue on Imaging
- Disappears on a true open-mouth or CT view
- Pitfall
- False-positive fracture call on plain film
- Distinguishing Feature
- Torticollis, asymmetric dens-lateral mass spacing
- Clue on Imaging
- Dynamic CT shows fixed rotation
- Pitfall
- Coexists with trauma in children
- Distinguishing Feature
- Lytic destruction, age-atypical pain
- Clue on Imaging
- Bone destruction without clear trauma, marrow replacement on MRI
- Pitfall
- Low-energy fracture can be the first sign of malignancy
An os odontoideum has smooth corticated margins and no marrow oedema, indicating chronicity, whereas an acute fracture has sharp irregular edges and prevertebral soft-tissue swelling. Treating a chronic, well-compensated os odontoideum as an acute fracture - or vice versa - is a common examination error. Dynamic flexion-extension imaging (when safe) clarifies whether it is stable.
Worth knowing as a condition, not just a differential line: os odontoideum is a rounded, well-corticated ossicle separated from a hypoplastic dens by a wide gap above the level of the transverse ligament, with a characteristically hypertrophied anterior C1 arch. Its origin is debated - congenital (failed fusion of the dens ossification centres) versus post-traumatic (an unrecognised childhood dens fracture that healed as a rounded nonunion) - and it is associated with Down syndrome, Klippel-Feil, Morquio and skeletal dysplasias. Two morphologies: orthotopic (ossicle in the normal dens position, moving with the C1 arch) and dystopic (ossicle fused to the clivus/occiput, the more unstable). The clinical problem is atlantoaxial instability: because the dens-equivalent is not anchored to C2, the transverse ligament loses its post, so flexion-extension views and the space available for the cord (posterior atlanto-dental interval) matter more than the ADI. Management: an asymptomatic, stable, incidental os odontoideum may be observed with activity precautions, but instability, neurological symptoms or signs, or a reduced space available for the cord mandate posterior C1-C2 fusion. The exam point is distinguishing it from an acute Type II (corticated/chronic vs sharp/oedematous) and not collaring a chronic unstable lesion that actually needs fusion.
Management Algorithm
Collar/Halo Treatment
- Rigid collar for 6-8 weeks
- Excellent union rate (95%+)
- Check for occipitocervical instability (alar ligaments)
- Rigid collar (Philadelphia, Miami J) or Halo
- Best for: Young, minimal displacement (under 5mm), transverse line
- Union rate 50-60% (lower in elderly)
- Close follow-up with CT at 6 and 12 weeks
- Rigid collar for 10-12 weeks (longer due to larger fracture)
- Excellent union rate (85%+)
- Halo rarely needed
- Collar
- Moderate
- Halo
- Best
- Collar
- Better
- Halo
- Poor
- Collar
- Fewer
- Halo
- Pin infections, loosening
- Collar
- Better
- Halo
- High complication rate
- Collar
- 50-60%
- Halo
- 60-70%
Halo vest in elderly (over 65) has high complication rate (40%+) including:
- Pin loosening, infection
- Respiratory complications
- Falls and further injury
- Poor tolerance
In elderly with Type II, primary posterior fusion often preferred over Halo.
Surgical Technique
Patient Positioning
- Supine on radiolucent table
- Head extended (chin tuck to expose neck)
- Shoulder roll
- Arms at sides (or taped down)
- C-arm access for AP and lateral
- Prone on Jackson or Mayfield frame
- Head neutral or slight flexion
- Mayfield pins or Gardner-Wells tongs
- Arms tucked
- Fluoroscopy or navigation
Proper positioning is essential for safe screw placement and to prevent intraoperative complications.
The Harms construct relies on a C2 screw, but in a substantial minority the C2 pedicle is too narrow (under about 4-5 mm) or the vertebral artery is "high-riding" (a high, medially-placed VA groove that thins the C2 isthmus) - placing a pedicle screw then risks catastrophic vertebral artery injury. Always template the C2 isthmus/pedicle and the VA foramen on the pre-operative CT. The graded alternatives when the pedicle is unsafe are: a C2 pars (Magerl-type) screw (shorter, staying posterolateral to the VA - lower VA risk but less purchase), or a C2 translaminar (intralaminar) screw (placed down the lamina, entirely avoiding the VA foramen - the safest for the VA but biomechanically weaker and dependent on laminar thickness). If even these are not feasible, fall back to C1-C2 wiring (Gallie/Brooks) supplemented by an orthosis, or extend to occipitocervical fixation if the C1 lateral mass is also compromised. This is the answer to "what if the C2 pedicle is under 4 mm?" - step down from pedicle to pars to translaminar screw, guided by the CT.
Complications
- Incidence
- 30-40% (collar)
- Prevention
- Patient selection, surgery for high-risk
- Management
- Posterior fusion
- Incidence
- Variable
- Prevention
- Maintain reduction
- Management
- Osteotomy if symptomatic
- Incidence
- 0.5-2%
- Prevention
- Preoperative CT planning
- Management
- Angiography, observation
- Incidence
- 5-10%
- Prevention
- Fluoroscopy/navigation
- Management
- Revision if symptomatic
- Incidence
- 10-20%
- Prevention
- Gentle retraction
- Management
- Usually temporary
- Incidence
- 2-5%
- Prevention
- Bone graft, rigid fixation
- Management
- Revision fusion
Nonunion Management
- Confirm nonunion on CT (over 6 months, no bridging bone)
- Assess instability with flexion-extension views
- Check transverse ligament on MRI
- Posterior C1-C2 fusion (Harms technique) is gold standard
- Anterior screw rarely works for nonunion (fibrous tissue)
- Consider occipitocervical fusion if C1 lateral mass compromised
Postoperative Care
Postoperative Protocol
Collar for all surgical patients. Wound care. DVT prophylaxis. Pain management.
Collar continues. X-rays at 2 and 6 weeks. Gentle ROM when comfortable. Physio for surrounding muscles.
CT at 6 weeks to assess fusion/healing. If progressing, continue collar. If not, reassess plan.
If CT shows union/fusion, wean collar. Flexion-extension X-rays to confirm stability. Physio for ROM and strengthening.
Collar Duration by Treatment
- Collar Duration
- 6-8 weeks
- Follow-up
- CT at 6 weeks
- Collar Duration
- 6-8 weeks
- Follow-up
- CT at 6 weeks for fusion
- Collar Duration
- 8-12 weeks
- Follow-up
- May need Halo if unstable
- Collar Duration
- 10-12 weeks (Type II/III)
- Follow-up
- CT at 6 and 12 weeks
Outcomes and Prognosis
Union Rates
- Collar
- 95%+
- Halo
- N/A
- Surgery
- N/A
- Collar
- 60%
- Halo
- 70%
- Surgery
- 90-95%
- Collar
- 40-50%
- Halo
- 50% (high complications)
- Surgery
- 90-95%
- Collar
- 85%+
- Halo
- 90%+
- Surgery
- 95%+
Mortality
- Elderly Type II: 15-25% 1-year mortality
- Nonunion contributes to mortality
- Balance surgical risk vs nonunion morbidity
- Function often limited with fibrous union
- Lower mortality in elderly (some studies)
- Early mobilization reduces complications
- Perioperative risk must be considered
- Better long-term function if fusion achieved
The elderly Type II dilemma:
- High nonunion with collar (40%)
- High Halo complication rate (40%)
- Surgical risk must be balanced
Recent evidence favors primary posterior fusion in fit elderly patients - better union, earlier mobilization, lower long-term mortality.
Guidelines, Registries & Global Practice
- Most common cervical fracture in patients over 70 worldwide
- Incidence rising with ageing populations across high-income countries
- Type II predominates (about 60% of dens fractures)
- Low-energy falls in the elderly now outnumber high-energy injuries
- Up to 80% of geriatric cases are osteoporotic-bone fractures
- Major trauma / spinal unit referral for all odontoid fractures
- CT first, MRI for ligament and cord assessment
- Elderly falls pathways should actively screen the C-spine
- Shared decision-making essential in frail elderly patients
Side-by-Side Society Guidance
- Emphasis
- Evidence-based management of dens fractures
- Type II Elderly Stance
- Surgery recommended for displacement over 5mm or age over 50; halo or surgery both options
- Emphasis
- Upper cervical injury classification, operative algorithms
- Type II Elderly Stance
- Favours operative stabilisation in unstable type II, individualised in frail elderly
- Emphasis
- Spinal injury assessment and major trauma pathways
- Type II Elderly Stance
- Multidisciplinary decision; nonoperative acceptable if surgery high-risk
- Emphasis
- Geriatric trauma, fragility-fracture care
- Type II Elderly Stance
- Early mobilisation prioritised; stable nonunion an accepted goal if unfit
Registry and Resource-Setting Notes
- No dedicated dens-fracture implant registry exists; outcome data derive from prospective cohorts such as the AOSpine North America Geriatric Odontoid Fracture (GOF) study rather than arthroplasty-style registries.
- High-resource settings: ready CT/MRI access, navigation or fluoroscopy for screw placement, and early posterior C1-C2 fixation in fit elderly.
- Limited-resource settings: reliance on plain radiographs and rigid collars, restricted MRI for ligament assessment, and a lower threshold for nonoperative management - making accurate stability assessment and falls prevention even more important.
Controversies and Areas of Uncertainty
Odontoid fracture management is one of the most genuinely contested areas in spinal trauma. A strong viva candidate can articulate where the evidence is soft and argue both sides.
The AOSpine GOF data suggest a 30-day survival advantage and higher fusion with surgery, but selection bias is unavoidable - fitter patients are offered surgery. No randomised trial has settled the question, and the competing systematic review found stable nonunion is an acceptable goal with under 5% needing revision.
In frail elderly patients, stable fibrous nonunion may give equivalent function and pain to bony union. Chasing radiographic union with high-risk surgery or prolonged halo may add morbidity without functional benefit.
Anterior screw preserves rotation but fails in osteoporotic bone, reverse-oblique lines and chronic fractures. Posterior C1-C2 fusion is more reliable but sacrifices rotation. The trade-off (motion vs union reliability) is unresolved for the borderline young-elderly patient.
Halo offers marginally better immobilisation but with high complication rates in the elderly. Many units have largely abandoned the halo in older patients, yet high-quality comparative data remain limited.
State the principle first ("treatment is individualised because the evidence is observational, not randomised"), then give the balance (survival/fusion advantage of surgery vs selection bias and the acceptability of stable nonunion), and finish with a patient-specific plan. Examiners reward candidates who acknowledge uncertainty rather than dogmatically insisting on one answer.
MCQ Practice Points
Q: Which odontoid fracture type has the highest nonunion rate?
A: Type II - fracture through the waist/base of the dens. This is at the watershed blood supply zone, leading to 30-40% nonunion with collar treatment. Type I and III have much higher union rates.
Q: What percentage of cervical rotation occurs at C1-C2?
A: 50% - This is why anterior odontoid screw fixation (which preserves the joint) is preferred over posterior fusion (which sacrifices rotation) when feasible.
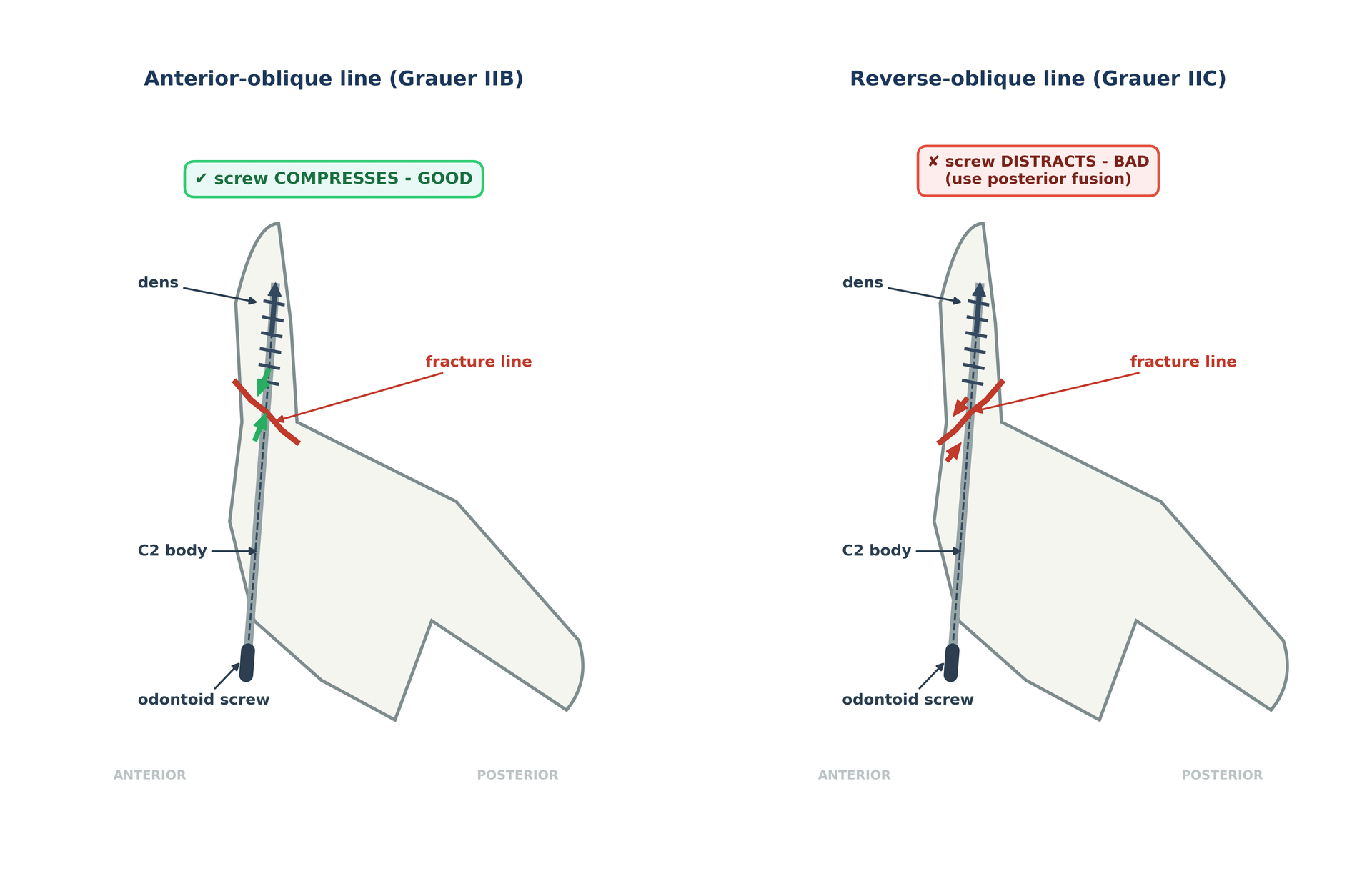
Q: What is a contraindication to anterior odontoid screw fixation?
A: Reverse oblique (posterior-superior to anterior-inferior) fracture line - The screw would distract rather than compress the fracture. Other contraindications: barrel chest, TAL rupture, elderly with osteoporosis, chronic nonunion.
Q: What ADI measurement suggests transverse ligament injury in an adult?
A: Greater than 3mm - Normal ADI in adults is under 3mm. In children, up to 5mm may be normal. Increased ADI indicates TAL incompetence and atlantoaxial instability.
Q: Why is Halo vest avoided in elderly patients with odontoid fractures?
A: High complication rate (40%+) - Including pin loosening, pin infection, respiratory complications, falls, and death. In elderly with Type II, primary posterior C1-C2 fusion often preferred.
Q: What is the fusion rate difference between single and double anterior odontoid screws?
A: No significant difference - Meta-analysis shows similar fusion rates (~90%). Single screw is technically easier and sufficient.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“78-year-old male fell at home. CT shows Type II odontoid fracture with 6mm posterior displacement. Neurologically intact. Past history of COPD and diabetes. How do you manage?”
“25-year-old male, MVA, Type II odontoid fracture, 4mm anterior displacement, transverse fracture line on CT. No TAL injury on MRI. Would you consider anterior screw fixation?”
“65-year-old female was treated with collar for Type II odontoid fracture 4 months ago. CT shows persistent fracture line with no bridging bone. She has ongoing neck pain. How do you assess and manage?”
Classification
- Type I: Tip (rare, stable, collar)
- Type II: Waist (60%, 40% nonunion, controversial)
- Type IIA: Comminuted Type II (posterior fusion)
- Type III: Into C2 body (85% union with collar)
Key Numbers
- ADI over 3mm = TAL injury (adult)
- Displacement over 5mm = surgical factor
- Angulation over 10° = surgical factor
- Age over 65 = increased nonunion risk
- 50% cervical rotation at C1-C2
Anterior Screw Contraindications (BARREL)
- B: Barrel chest
- A: Angulation posteriorly
- R: Reverse oblique fracture
- R: Ruptured TAL
- E: Elderly/osteoporotic
- L: Late presentation
Treatment by Type
- Type I: Collar 6-8 weeks
- Type II (young): Collar vs anterior screw
- Type II (elderly): Posterior fusion (Harms)
- Type IIA: Posterior fusion (no screw)
- Type III: Collar 10-12 weeks
Surgical Options
- Anterior screw: Preserves rotation, for ideal Type II
- Harms (C1-C2): Gold standard posterior, sacrifices rotation
- Magerl: Transarticular, higher VA risk
- Wiring: If screws not possible
Evidence Base
AOSpine GOF Mortality Study: Surgery vs Non-Op in the Elderly
- Retrospective multicentre cohort of 322 patients aged 65 or older with type II odontoid fracture (165 operative, 157 nonoperative). Nonoperative treatment carried higher 30-day mortality (adjusted HR 3.00, 95% CI 1.51-5.94) with a trend toward higher long-term mortality (HR 1.35, 95% CI 0.97-1.89). Overall 30-day mortality 14%, maximal follow-up mortality 44%.
AOSpine GOF Treatment Predictors
- Prospective multicentre cohort of 159 patients aged 65 or older with radiographically confirmed type II odontoid fracture. Independent predictors of treatment failure were older age (OR 1.08 per year), initial nonsurgical treatment (OR 3.09), male sex (OR 4.33) and baseline neurological comorbidity (OR 4.13). 12-month mortality 18.2%.
Nonunion Outcomes With Nonoperative Treatment
- Subgroup of the AOSpine GOF study (58 nonoperatively treated elderly type II fractures). 30% developed primary or secondary nonunion and 22% required delayed surgery, yet NDI and SF-36 outcomes did not differ by union status at 12 months.
Anterior Odontoid Screw Fixation (Landmark Series)
- 147 consecutive patients undergoing direct anterior odontoid screw fixation. Fusion rate 88% for recent fractures (6 months or less) but only 25% for remote fractures (18 months or more). Fusion was independent of patient age, sex and number of screws (one vs two); horizontal and posterior-oblique fracture lines fused better than anterior-oblique.
Age as a Risk Factor for Halo Failure
- Case-control study of 33 isolated type II dens fractures treated by halo immobilisation. Age over 50 years was a highly significant risk factor for nonunion (P = 0.002), with a 21-fold higher risk of halo failure. Sex, displacement amount and direction were not significant.
Transverse Atlantal Ligament Injury Classification
- Analysis of 39 transverse atlantal ligament injuries defined the Dickman classification: Type I (midsubstance disruption, n=16) cannot heal without internal fixation and needs early surgery; Type II (bony avulsion from the C1 tubercle, n=23) is initially treated in a rigid orthosis with a 74% success rate.
Harms Technique: Posterior C1-C2 Polyaxial Screw-Rod Fixation
- Original description of C1 lateral mass plus C2 pars/pedicle polyaxial screws connected by rods in 37 patients. Solid fusion was achieved in all patients with no vascular or neurological injury, and the technique allows intraoperative reduction without sacrificing the joint surfaces if temporary.