Most Common Benign Bone Tumor | Cartilage-Capped Exostosis | Malignant Transformation Risk 1%
- Most common benign bone tumor - represents 35% of all benign bone lesions
- Stops growing at skeletal maturity - continued growth after maturity suggests malignancy
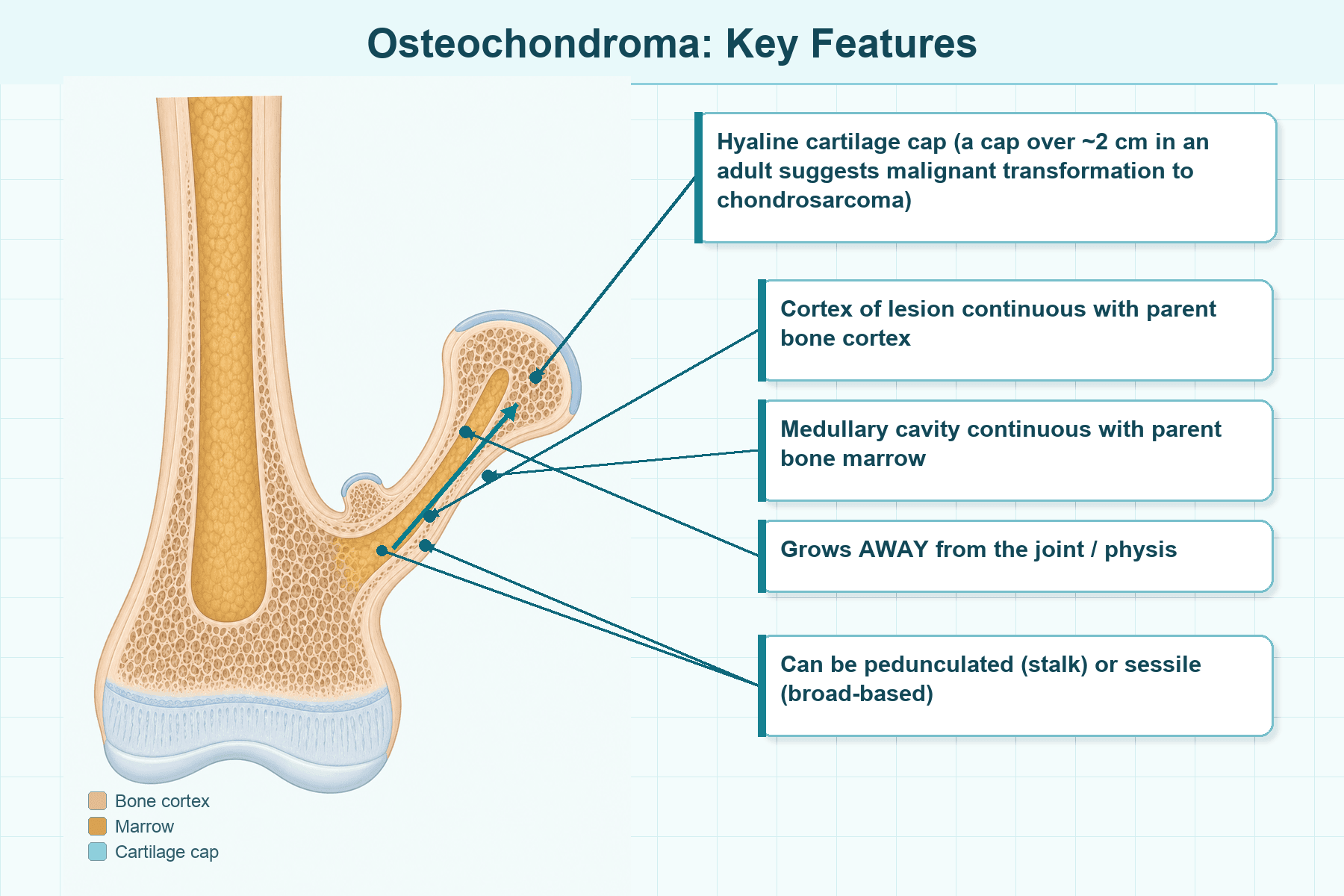
- Cartilage cap under 2cm in adults is reassuring; greater than 2cm raises malignancy concern
- HME has autosomal dominant inheritance with 5-25% malignant transformation risk
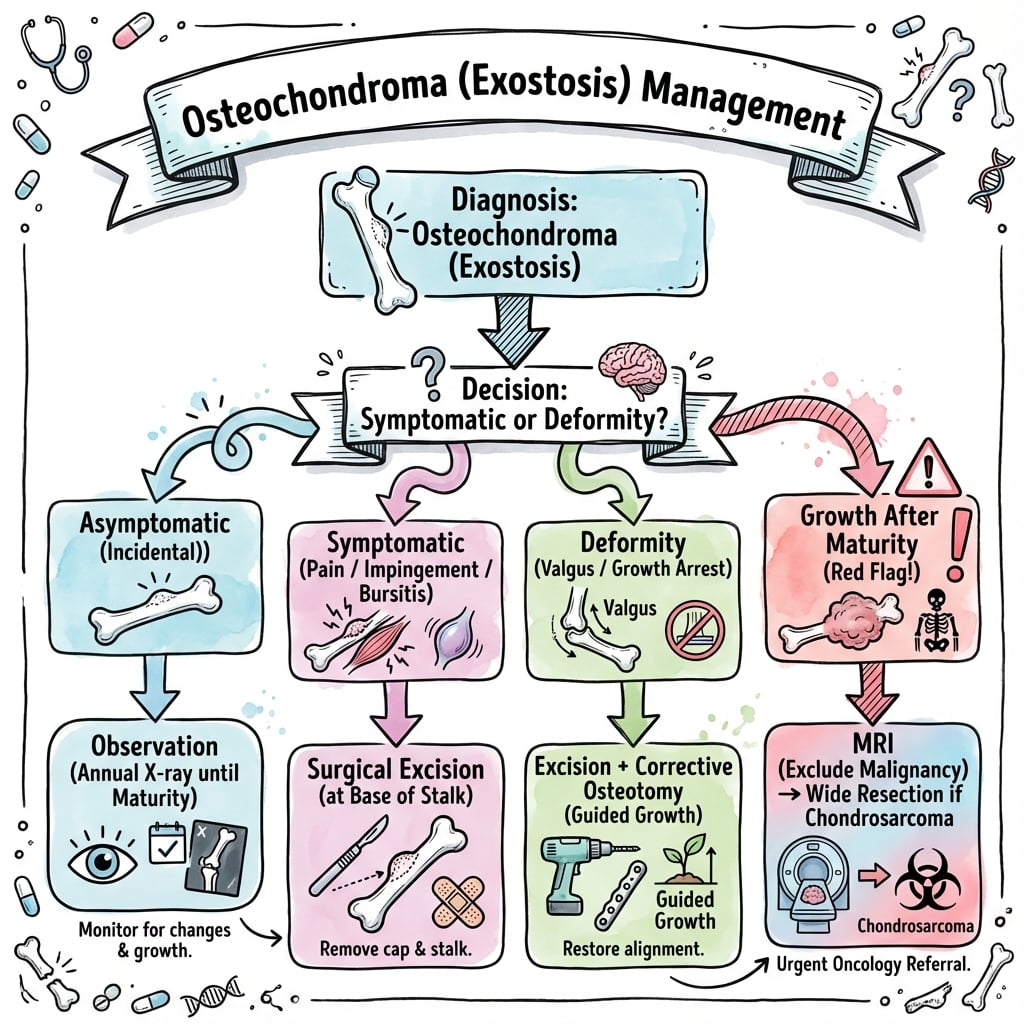
- Surgical indications: pain, neurovascular compromise, cosmesis, or suspected malignancy
- “Examiners ask about continued growth after skeletal maturity - this is sarcomatous change until proven otherwise
- “Know imaging features of malignancy: cartilage cap greater than 2cm, irregular calcification, soft tissue mass
- “EXT1 and EXT2 mutations cause hereditary multiple exostoses (HME)
- “Distinguish from parosteal osteosarcoma - osteochondroma has cortical and medullary continuity
Growth after skeletal maturity. Any osteochondroma that continues enlarging after physeal closure must be biopsied. Also suspect if cartilage cap greater than 2cm on MRI in adults.
Hereditary Multiple Exostoses: Autosomal dominant (EXT1/EXT2). 5-25% malignant transformation vs 1% for solitary lesions. Screen annually with clinical exam.
Cortical and medullary continuity with parent bone. Cartilage cap visible on MRI. No need for biopsy unless malignancy suspected.
4 main indications: Pain, neurovascular compression, cosmetic deformity, or concern for malignant transformation. Excise with cartilage cap intact.
- Cap Thickness
- Under 2cm
- Management
- Observation only
- Key Pearl
- Will stop growing at skeletal maturity
- Cap Thickness
- Under 2cm
- Management
- Surgical excision
- Key Pearl
- Remove entire cartilage cap to prevent recurrence
- Cap Thickness
- Greater than 2cm
- Management
- MRI + biopsy + wide excision
- Key Pearl
- Suspect secondary chondrosarcoma
EXOSTOSISFeatures of Osteochondroma
Hook:Think EXOSTOSIS - this IS the name for the bony outgrowth! Growth STOPS at skeletal maturity unless malignant.
PNCCIndications for Surgical Excision
Hook:PNCC - Pain, Nerves/vessels, Cosmetic, Cancer worry - these are your reasons to operate.
CAPSRed Flags for Malignant Transformation
Hook:Think CAPS - the cartilage CAP is the key! Thick caps, growing caps after maturity = secondary chondrosarcoma.
Overview and Epidemiology
Osteochondroma is the most common benign bone tumor, accounting for 35% of all benign osseous lesions and 8-9% of all bone tumors. It represents a developmental anomaly arising from aberrant cartilage at the growth plate periphery, not a true neoplasm. The lesion grows by enchondral ossification and ceases growth at skeletal maturity - any growth after physeal closure is highly suspicious for malignant transformation to secondary chondrosarcoma.
- Age: 10-20 years (during active growth)
- Gender: Male predominance 2:1
- Location: Metaphysis of long bones (70%)
- Most common sites: Distal femur, proximal tibia, proximal humerus
- Growth pattern: Enlarges during skeletal growth
- Maturity: Stops growing when physis closes
- Recurrence: 2% if incompletely excised
- Transformation: 1% solitary, 5-25% in HME
Pathophysiology and Genetics
Developmental Anomaly
Osteochondroma arises from aberrant cartilage that herniates through a defect in the perichondral ring of the growth plate. This displaced cartilage maintains growth potential and undergoes enchondral ossification, forming a cartilage-capped bony projection that is continuous with the underlying bone cortex and medullary cavity.
Osteochondroma is considered a developmental error rather than a true tumor. The lesion grows by the same mechanism as normal physeal growth and stops enlarging at skeletal maturity. This distinguishes it from neoplastic processes that continue growing regardless of skeletal age.
Genetic Basis of HME
- Location: EXT1 on chromosome 8q24; EXT2 on 11p11-13
- Function: Encode glycosyltransferases for heparan sulfate synthesis
- Inheritance: Autosomal dominant with high penetrance
- Loss of heterozygosity: Required for lesion development
- Screening: First-degree relatives of HME patients
- Malignancy risk: 5-25% in HME vs 1% solitary
- Growth disturbance: Forearm and lower leg deformities
- Genetic counseling: 50% transmission risk to offspring
Malignant Transformation
Secondary chondrosarcoma develops in 1% of solitary osteochondromas and 5-25% of HME cases. Transformation typically occurs in adulthood and is heralded by renewed growth, increasing pain, or enlarging cartilage cap. The chondrosarcoma is usually low-grade (Grade 1), but wide excision is required for cure.
Pathology
Gross Pathology
The lesion consists of a cartilage cap (hyaline cartilage) overlying a bony stalk. The stalk is composed of normal trabecular bone and marrow, continuous with the parent bone. The cartilage cap is covered by a fibrous perichondrium.
Thickness: Cap is typically 3-10 mm in adults. Pediatric caps can be up to 20-30 mm during active growth.
Histology
- Hyaline cartilage cap: Chondrocytes in lacunae
- Perichondrium: Fibrous covering over cartilage
- Enchondral ossification: Active at base of cap during growth
- Normal bone: Trabecular bone and marrow in stalk
- Hypercellularity: Increased chondrocyte density
- Nuclear atypia: Enlarged, hyperchromatic nuclei
- Myxoid change: Degeneration of cartilage matrix
- Permeative growth: Invasion into adjacent soft tissue
Biopsy of the cartilage cap is challenging - active enchondral ossification in pediatric patients can show cellular atypia that mimics low-grade chondrosarcoma. Correlation with imaging (cap thickness) and clinical features (age, growth pattern) is essential. Biopsy is only indicated if malignancy is suspected.
Classification and Morphology
Morphological Classification
- Description
- Narrow stalk with bulbous cap
- Location
- Metaphysis of long bones
- Clinical Notes
- Easier to excise, less deformity
- Description
- Broad-based attachment
- Location
- Flat bones (scapula, pelvis)
- Clinical Notes
- Higher malignancy risk due to thicker cap
Pedunculated lesions are more common in long bones and point away from the adjacent joint due to muscle traction during growth. Sessile lesions have broader bases and are more common in flat bones (pelvis, scapula) - these carry slightly higher malignant transformation risk due to typically thicker cartilage caps.
Skeletal Deformity in Multiple Osteochondromas (HME)
Beyond malignancy risk, the major morbidity of HME is growth-plate tethering deformity. The forearm is the classic site and has its own named classification.
- Main lesion / pattern
- Osteochondroma at the DISTAL ULNA with ulnar shortening
- Key feature
- Relative ulnar shortening, radial bowing, ulnar tilt of the distal radius (pseudo-Madelung); radial head reduced
- Main lesion / pattern
- Radial head DISLOCATION with an osteochondroma at the PROXIMAL RADIUS
- Key feature
- Dislocated radial head + proximal radius lesion
- Main lesion / pattern
- Radial head DISLOCATION without a proximal radius lesion
- Key feature
- Dislocation driven by ulnar shortening alone
- Main lesion / pattern
- Osteochondroma at the DISTAL RADIUS with relative radial shortening
- Key feature
- Distal radius lesion, ulna relatively spared
HME tethers physes asymmetrically, producing characteristic deformities: forearm (ulnar shortening/radial bowing/radial head subluxation, reduced forearm rotation - managed per Masada type by osteochondroma excision, ulnar lengthening, radial osteotomy or hemiepiphysiodesis); ankle valgus (from distal fibular shortening/distal tibial physeal involvement - treated with medial distal-tibial hemiepiphysiodesis (guided growth) in the growing child, or supramalleolar osteotomy near maturity); genu valgum (medial distal-femoral/proximal-tibial guided growth or osteotomy); coxa valga and acetabular dysplasia; and limb-length discrepancy. The governing principle is guided growth (hemiepiphysiodesis) while physes are open, corrective osteotomy nearer maturity - which is why HME children need monitoring of alignment and limb length throughout growth, not just malignancy surveillance.
Clinical Presentation
- Painless mass: Most common presentation (found incidentally)
- Mechanical pain: Impingement on adjacent structures
- Snapping: Tendon or muscle irritation over lesion
- Fracture: Pedunculated stalk fracture (rare, usually painless)
- Growth concerns: Parents notice enlarging mass in child
- Palpable mass: Firm, non-tender, fixed to bone
- Size: Variable (1-10 cm typical)
- Location: Metaphyseal region of long bones
- Neurovascular: Check for compression symptoms
- Joint motion: Assess for mechanical block
Red Flag Symptoms (Malignant Transformation)
Any of these findings in an adult with known osteochondroma requires urgent imaging and possible biopsy:
- New or increasing pain not explained by mechanical factors
- Growth after skeletal maturity - lesion should be quiescent after physeal closure
- Rapidly enlarging mass - suggests aggressive cartilage proliferation
- Neurovascular symptoms - new onset compression or ischemia
Complications of Osteochondroma
- Mechanism
- Friction over bony prominence
- Management
- Excision of lesion if symptomatic
- Mechanism
- Mass effect on adjacent structures
- Management
- Surgical decompression/excision
- Mechanism
- Trauma to pedunculated lesion
- Management
- Usually non-operative, excision if symptomatic
- Mechanism
- Physeal tethering in HME
- Management
- Guided growth or osteotomy
Imaging and Diagnosis
Plain Radiographs
Radiographic Features
Cortex of lesion is continuous with cortex of parent bone. The medullary cavity of the lesion also merges with the host bone medullary canal. This is the diagnostic hallmark.
Cartilage cap is not visible on plain X-ray unless it contains calcifications. Cap thickness can only be assessed with MRI.
Pedunculated lesions point away from the nearest joint due to muscle pull during growth. Sessile lesions are broad-based.
Punctate, irregular calcifications within soft tissue suggest malignant transformation. Benign caps show organized ring-and-arc calcification if any.
MRI - Gold Standard for Cap Assessment
- Cartilage cap under 2cm in adults (under 3cm in children acceptable)
- Smooth, regular cap with homogeneous signal
- No soft tissue mass beyond cartilage cap
- T2 high signal in cartilage (normal hyaline cartilage)
- Cartilage cap greater than 2cm in adults (suspicious)
- Irregular, nodular cap with heterogeneous signal
- Soft tissue mass extending beyond cap
- Destruction of underlying bone cortex
Cartilage cap thickness greater than 2cm in a skeletally mature patient is concerning for malignant transformation. This should prompt biopsy. In children and adolescents, caps up to 3cm may be acceptable as the cartilage is still actively growing. Serial MRI is useful to document stability.
CT Scan
Indications for CT:
- Assessment of cortical breach or bone destruction
- Preoperative planning for complex anatomy (pelvis, scapula)
- Evaluation of calcification pattern in cartilage cap
CT is less useful than MRI for measuring cartilage cap but superior for bone detail.
Differential Diagnosis
- Key Distinguishing Feature
- NO cortical/medullary continuity
- Imaging Clue
- Lesion wraps around bone, distinct from cortex
- Key Distinguishing Feature
- Zonal phenomenon (mature periphery)
- Imaging Clue
- History of trauma, maturation pattern
- Key Distinguishing Feature
- Scalloping of cortex, no continuity
- Imaging Clue
- Small, often in hand/foot


Management Algorithm
Observation Protocol
Indications for observation:
- Asymptomatic lesion in child or adolescent
- Small size with no neurovascular compromise
- Typical imaging appearance (cortical continuity, thin cap)
- No growth after skeletal maturity
Surveillance Schedule
Clinical examination yearly during growth. X-ray if symptoms develop or size changes noted.
Once growth plates close and lesion is stable, discharge with instructions to return if new symptoms develop.
Annual clinical exam for life. Baseline MRI of any large or symptomatic lesions. Repeat MRI if growth or pain develops.
For solitary osteochondroma, once skeletal maturity is reached and the lesion is asymptomatic, no further routine follow-up is needed. Educate patient to return if new growth or pain. For HME, lifelong clinical surveillance is recommended due to higher malignancy risk.
Management of Malignant Transformation
- Treatment
- Wide excision with negative margins
- Margin Goal
- Wide margin (5-10mm normal tissue)
- Treatment
- Wide excision +/- adjuvant therapy
- Margin Goal
- Wide margin, consider limb salvage vs amputation
Prognosis: Low-grade secondary chondrosarcoma has excellent prognosis with wide excision - 90% 5-year survival. High-grade lesions have poorer outcomes and may require chemotherapy/radiation (though chondrosarcoma is relatively chemo-resistant).
Complications
Surgical Complications
- Neurovascular injury: Risk depends on location; common peroneal nerve at proximal fibula, axillary nerve at proximal humerus
- Incomplete excision: Failure to remove entire cartilage cap leads to recurrence (2%)
- Fracture through stalk: May occur during manipulation of pedunculated lesions
- Recurrence: 2% if cartilage cap incompletely excised
- Wound infection: Standard surgical site infection rates (2-3%)
- Hematoma: Rare; usually self-limiting
- Pathologic fracture: Through weakened bone at excision site (rare)
Disease-Related Complications
- Mechanism
- Secondary chondrosarcoma develops in cartilage cap
- Management
- Wide excision with negative margins
- Prevention
- Surveillance for red flags; intervene if cap greater than 2cm
- Mechanism
- Friction over bony prominence creates fluid-filled sac
- Management
- Excision of lesion if symptomatic
- Prevention
- Cannot be prevented; patient education
- Mechanism
- Mass effect on adjacent vessels/nerves
- Management
- Surgical decompression and excision
- Prevention
- Early intervention for enlarging lesions
- Mechanism
- Physeal tethering in HME
- Management
- Guided growth or osteotomy
- Prevention
- Early recognition and intervention
- Mechanism
- Forearm and lower leg most common in HME
- Management
- Corrective osteotomy if functional impairment
- Prevention
- Regular monitoring during growth
Malignant transformation to secondary chondrosarcoma is the most serious complication. Risk is 1% for solitary lesions and 5-25% for HME. Key indicators: growth after skeletal maturity, new pain in adult, cartilage cap greater than 2cm on MRI. Wide excision is curative for low-grade lesions (90% 5-year survival).
Outcomes and Prognosis
Surgical Outcomes
Recurrence: 2% if cartilage cap incompletely excised. Nearly 0% if complete excision achieved. Recurrences typically occur within 2 years and may require re-excision.
Complications:
- Neurovascular injury: Rare (under 1%) if careful dissection
- Wound infection: 2-3% (standard surgical site infection rates)
- Pathologic fracture through excision site: Rare, more common with large sessile lesions
Long-term Prognosis
For solitary osteochondroma, prognosis is excellent. Most lesions are asymptomatic and require no treatment. Those requiring excision have excellent outcomes with low recurrence.
For HME, quality of life is impaired by multiple lesions, skeletal deformities (forearm, lower leg), and lifelong malignancy surveillance. Genetic counseling is important for family planning.
Guidelines, Registries & Global Practice
Global Epidemiology
- Solitary osteochondroma: most common benign bone tumour worldwide; true prevalence underestimated as most are asymptomatic
- Multiple osteochondromas (MO/HME): estimated prevalence around 1 in 50,000 in populations of European descent
- Higher reported rates in some isolated and indigenous populations (founder effect)
- Sex: male predominance for solitary lesions and for symptomatic MO disease
- Solitary: approximately 1% lifetime risk of secondary chondrosarcoma
- MO/HME: widely quoted at 1-5% in modern series, historically reported up to 25%
- EXT1 genotype and axial/pelvic lesions carry the highest risk
- Median age at transformation in the 30s - surveillance must extend into adulthood
Society Guidance - Side by Side
- Diagnosis
- Plain film usually diagnostic; MRI to measure cartilage cap if growing or painful
- Surveillance
- Active surveillance for asymptomatic lesions; cap measurement to triage
- Surgery / Referral
- Refer suspected secondary chondrosarcoma to a specialist bone-sarcoma centre before any biopsy
- Diagnosis
- Suspected primary bone cancer pathway triggered by an enlarging or painful bony mass in an adult
- Surveillance
- Urgent imaging within defined cancer-pathway timeframes
- Surgery / Referral
- Biopsy and definitive surgery only at a recognised bone-tumour unit
- Diagnosis
- Imaging-led diagnosis; biopsy reserved for malignancy concern
- Surveillance
- Observation for typical asymptomatic lesions
- Surgery / Referral
- Wide excision for confirmed secondary chondrosarcoma; en-bloc principles
- Diagnosis
- Osteochondroma classified as benign; secondary peripheral chondrosarcoma graded 1-3
- Surveillance
- Grading drives prognosis and margin planning
- Surgery / Referral
- Atypical cartilaginous tumour / grade 1 distinguished from higher-grade disease
Across all major frameworks the principle is identical: do not biopsy a suspected cartilage malignancy outside a specialist bone-sarcoma unit. A poorly placed biopsy tract can compromise later limb-salvage surgery. The 2cm adult cartilage-cap threshold and growth-after-maturity are the shared triggers for referral.
Registries & Resource-Setting Variation
- Disease-specific registries (e.g. the Registry of Multiple Osteochondromas, Rizzoli) underpin natural-history and transformation data
- National bone-tumour networks (UK, several European countries) centralise sarcoma care
- Genetic databases catalogue EXT1/EXT2 variants for diagnosis and counselling
- No arthroplasty-style implant registry applies, as treatment is excisional
- High-resource: MRI cap measurement, EXT genotyping, multidisciplinary sarcoma boards, limb salvage
- Limited-resource: plain radiographs and clinical surveillance are the mainstay; MRI and genetics may be unavailable
- Shared minimum standard: recognise red flags (growth after maturity, new pain, palpable enlargement) and refer
- Telemedicine and regional referral increasingly bridge access gaps for suspected malignancy
- Risk of incomplete excision and recurrence (around 2%)
- Site-specific neurovascular injury risk
- Risk of underlying malignancy if cartilage cap greater than 2cm (document pre-operative imaging)
- For MO/HME patients: counsel about lifelong surveillance and autosomal dominant inheritance
Record cartilage cap thickness on MRI in adults, the rationale for observation versus surgery, and (for MO/HME) family history and the genetic counselling offered.
Controversies & Areas of Uncertainty
- The classic 2cm adult threshold is a pragmatic rule, not an absolute cut-off
- Murphey's original archival data used 1.5cm; later MRI series favour 2cm in adults
- Caps change with technique (ultrasound vs MRI) and slice plane, so serial change matters more than any single number
- Growth after maturity outweighs a static cap measurement as a red flag
- Historical figures of up to 25% came from referral-centre cohorts with selection bias
- Contemporary population-based estimates cluster around 1-5% lifetime risk
- EXT1 genotype, pelvic/axial sites and large sessile lesions concentrate the risk
- The right denominator (all MO patients vs those reaching sarcoma units) remains debated
- No randomised evidence defines the optimal interval or imaging modality for MO surveillance
- Whole-body MRI is attractive but cost and access limit routine use
- Most centres rely on symptom-driven imaging plus periodic clinical review
- Over-surveillance risks incidental findings and patient anxiety
- The line between grade 1 secondary chondrosarcoma and a benign reactive cap is genuinely difficult
- WHO now uses atypical cartilaginous tumour for some low-grade appendicular lesions
- Pediatric caps showing cellular atypia can mimic low-grade malignancy histologically
- Imaging-pathology-clinical correlation, not histology alone, drives the call
MCQ Practice Points
Q: What is the most common benign bone tumor? A: Osteochondroma - accounts for 35% of all benign bone tumors and 8-9% of all bone tumors. Peak age 10-20 years during active skeletal growth.
Q: What is the pathognomonic imaging feature of osteochondroma? A: Cortical and medullary continuity with the parent bone. The cortex of the lesion is continuous with the cortex of the underlying bone, and the medullary cavity merges with the host bone marrow.
Q: What cartilage cap thickness raises concern for malignant transformation in an adult? A: Greater than 2cm in a skeletally mature patient. Caps under 2cm are reassuring. In children, caps up to 3cm may be acceptable during active growth.
Q: What genes are mutated in Hereditary Multiple Exostoses? A: EXT1 (chromosome 8q24) and EXT2 (chromosome 11p11-13). These genes encode glycosyltransferases required for heparan sulfate synthesis. Inheritance is autosomal dominant.
Q: When does osteochondroma stop growing? A: At skeletal maturity when the growth plates close. Any growth after physeal closure is concerning for malignant transformation to secondary chondrosarcoma.
Q: What is essential during surgical excision to prevent recurrence? A: Complete removal of the entire cartilage cap with the base of the stalk. Recurrence rate is 2% with incomplete excision, nearly 0% with complete excision.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy presents with a painless mass on his distal femur noticed by his mother. X-ray shows a pedunculated lesion with cortical and medullary continuity with the femur. What is your diagnosis and management?”
“A 35-year-old woman with known osteochondroma of the proximal humerus since childhood presents with increasing pain and size of the lesion over 6 months. MRI shows cartilage cap thickness of 3.5cm. How do you proceed?”
“A 10-year-old boy presents with multiple bony prominences around his knees and ankles. His father had similar lesions. What is your diagnosis and how do you manage this patient and family?”
Key Facts
- Most common benign bone tumor (35% of all benign bone lesions)
- Peak age 10-20 years, male 2:1
- Metaphysis of long bones (distal femur, proximal tibia most common)
- Stops growing at skeletal maturity - growth after = malignancy
Diagnosis
- Cortical and medullary continuity = pathognomonic
- Cartilage cap under 2cm in adults (under 3cm in children)
- MRI gold standard for cap assessment
- No biopsy needed unless malignancy suspected
Malignant Transformation
- Solitary: 1% risk; HME: 5-25% risk
- Red flags: growth after maturity, cap greater than 2cm, new pain
- Secondary chondrosarcoma (usually low-grade)
- Wide excision curative - 90% 5-year survival for low-grade
Surgical Indications (PNCC)
- Pain (mechanical or mass effect)
- Neurovascular compromise
- Cosmetic deformity
- Concern for malignancy (cap greater than 2cm, growth)
HME
- EXT1/EXT2 mutations (autosomal dominant)
- Lifelong surveillance required (annual clinical exam)
- Manage skeletal deformities (forearm, lower leg)
- Genetic counseling - 50% transmission risk
Surgical Pearls
- Remove ENTIRE cartilage cap to prevent recurrence
- Recurrence 2% if incomplete, 0% if complete excision
- Send entire specimen to pathology intact
- If malignancy suspected, frozen section before closure
Evidence Base and Key Studies
Imaging of Osteochondroma - Radiologic-Pathologic Correlation
- Definitive AFIP radiologic-pathologic review of osteochondroma and its variants
- Cortical and medullary continuity with the parent bone is the pathognomonic hallmark
- Malignant transformation in roughly 1% of solitary lesions and 3-5% of HME
- Continued growth or a hyaline cap thicker than 1.5cm after skeletal maturity suggests malignancy
Severity of Disease and Risk of Malignant Change in HME - Genotype-Phenotype
- Prospective genotype-phenotype study of 172 individuals from 78 HME families
- EXT1 and EXT2 mutations were almost equally common (identified in 83%)
- EXT1 mutations produced significantly worse disease (stature, deformity, function) than EXT2
- Seven sarcomas arose in EXT1 carriers versus one in an EXT2 carrier
Secondary Peripheral Chondrosarcoma in Multiple Osteochondromas
- Single-institution series of 105 secondary peripheral chondrosarcomas in MO (1960-2019)
- Median age at diagnosis 34 years (range 13-63) - transformation can occur in young adults
- Pelvis was the most frequent site (44%), followed by the lower limb
- Most lesions were grade 1 (59) with grade 2 or 3 and partial resection predicting worse disease-free survival
Cartilage Cap Thickness Measurement - Benign vs Exostotic Chondrosarcoma
- Cartilage cap thickness measured by ultrasound versus pathology in 22 exostoses and 2 chondrosarcomas
- Mean measurement error under 2mm for caps less than 2cm thick
- Ultrasound accuracy exceeded CT and was comparable to MRI
- A thin cap suggests a benign exostosis whereas a thick cap suggests malignancy
Surgical Management of Chest Wall Osteochondroma in Children
- Series of 7 children operated for chest wall osteochondroma from a clinic cohort of 854 exostosis patients
- Indications were pain, diagnostic confirmation, recurrent pneumothorax, and malignancy
- No recurrence of exostosis on follow-up after excision
- No malignant transformation or intrathoracic complications occurred
Shoulder Exostoses as a Marker of EXT1 Genotype and Malignant Change
- Prospective HME database of 172 patients with 5361 palpable exostoses analysed
- Shoulder exostoses strongly predicted an EXT1 genotype (odds ratio 20.6)
- Scapular exostoses carried the highest probability of malignant change of any site
- Seven chondrosarcomas occurred (2 scapular, 1 proximal humeral)