OCD | Juvenile vs Adult | Stable vs Unstable | MFC
- Lateral aspect of medial femoral condyle is the most common location (75%) - classic site
- Juvenile (open physis) has significantly better prognosis than adult form
- Stable lesions in juveniles can heal conservatively with activity modification (50-70%)
- Unstable or adult lesions usually require surgery (drilling, fixation, or excision)
- MRI is gold standard to assess stability (fluid behind fragment = unstable)
- “Wilson sign: pain with IR at 90 then relieved with ER (impinges ACL on MFC)
- “Classic location: lateral aspect of MFC
- “T2 MRI shows fluid under fragment ('rim sign') = unstable
- “Juvenile stable: rest 3-6 months first line
Lateral aspect of medial femoral condyle (75%). Other sites: lateral femoral condyle (20%), patella, trochlea, tibial plateau (rare). Classic location is PCL origin on MFC.
Juvenile = open physis = better prognosis. Can heal with conservative treatment. Adult = closed physis = often needs surgery. Physis status is the most important prognostic factor.
MRI is key. High T2 signal behind fragment (rim sign) = fluid = unstable. Intact cartilage surface with no fluid = stable. Cystic changes = unstable.
Stable juvenile: conservative. Unstable or adult: surgery. Options include drilling (retrograde/transarticular), fixation (compression screws), or excision (if unsalvageable).
- Physis
- Open
- Stability
- Stable
- Treatment
- Conservative (3-6mo)
- Prognosis
- Good (50-70% heal)
- Physis
- Open
- Stability
- Unstable
- Treatment
- Surgery (Fixation)
- Prognosis
- Good if fixed
- Physis
- Closed
- Stability
- Stable
- Treatment
- Surgery (Drilling/Fix)
- Prognosis
- Fair
- Physis
- Closed
- Stability
- Unstable
- Treatment
- Surgery (Fix/Excision)
- Prognosis
- Poor (OA risk)
MFCOCD Location
Hook:MFC lateral wall is classic location!
FLUIDMRI Signs of Instability
Hook:FLUID on MRI means unstable lesion!
Overview and Epidemiology
Osteochondritis dissecans (OCD) is an acquired idiopathic lesion of subchondral bone that can affect the overlying articular cartilage. It ranges from softening of the cartilage to complete detachment of a bony fragment (loose body). The knee is the most common location (75% of all OCD).
Etiology
Cause uncertain (multifactorial):
- Repetitive microtrauma: Most accepted theory (active adolescents)
- Vascular insufficiency: Ischemia of subchondral bone
- Genetic factors: Familial clustering reported
- Ossification: Aberrant ossification centre
Active adolescent male. Most common presentation is a 10-20 year old male athlete with vague knee pain.
Epidemiology
- Incidence: 15-30 per 100,000
- Age: Juvenile (open physis) vs Adult (closed physis)
- Gender: Male greater than Female (2:1)
- Bilateral: 20-30% of cases (always xray other knee)
Pathophysiology and Mechanisms
Anatomy
Classic Location:
- Medial Femoral Condyle (MFC): 75% of cases
- Specific Site: Lateral aspect of the MFC (lateral wall of intercondylar notch)
- Other Sites: Lateral femoral condyle (20%), Patella (5%), Trochlea (less than 1%)
Why Lateral MFC?
- Impingement of the Tibial Spine or PCL against the lateral aspect of the MFC during knee motion
- Occurs near the insertion of the PCL
Pathophysiology
- Subchondral Bone Event: Ischemia or stress fracture of subchondral bone
- Overlying Cartilage: Initially intact (stable)
- Separation: Bone fragment separates from parent bone
- Instability: Cartilage breach allows fluid ingress (unstable)
- Loose Body: Fragment detaches completely
Physis Status: Open physis (Juvenile OCD) has much better healing potential due to vascularity. Closed physis (Adult OCD) rarely heals without intervention.
VIAGRAOCD Etiology
Hook:The etiology of OCD is multifactorial (VIAGRA).
Classification Systems

Anatomic Location Classification
Location on Condyle:
- 1: Central
- 2: Lateral (Classic - aligned with tibial spine)
- 3: Inferocentral
- 4: Central anterior
- 5: Anterior lateral
Type 2 corresponds to the classic lateral aspect of MFC.
Location helps predict prognosis.
The ROCK Arthroscopic Classification
The global-practice section names the ROCK group (Research in OsteoChondritis of the Knee) and its arthroscopic, probe-based classification — a modern, reproducible system worth knowing alongside the older Guhl/ICRS and Cahill schemes.
- The principle. ROCK divides lesions at arthroscopy (by probing) into two families — immobile (stable) and mobile (unstable) — because mobility on probing, not appearance alone, drives the drilling-versus-fixation decision.
- Immobile (stable) lesions — drilled if they fail non-operative care:
- Cue ball — intact, normal-looking cartilage, no demarcation.
- Shadow — a subtle demarcation visible through intact cartilage.
- Wrinkle in the rug — a raised fissure or buckle of the cartilage surface, still stable.
- Mobile (unstable) lesions — need fixation or restoration:
- Locked door — a demarcated lesion that cannot be hinged open on probing.
- Trapdoor — a fragment that hinges open on probing.
- Crater — a detached fragment/loose body leaving an empty crater.
- Why it matters. It gives a shared vocabulary that correlates with intra-operative stability better than MRI alone (recall the poor juvenile MRI specificity) and maps directly to treatment: immobile → drilling; mobile → fixation of a salvageable fragment, or restoration of an unsalvageable crater.
Q: How does the ROCK arthroscopic classification stratify knee OCD? A: By probe mobility into immobile/stable (cue ball, shadow, wrinkle in the rug) and mobile/unstable (locked door, trapdoor, crater). Immobile lesions that fail conservative care are drilled; mobile lesions need fixation (salvageable) or restoration (unsalvageable crater) — probing is more reliable than a juvenile MRI rim.
Clinical Assessment
History
- Pain: Vague, poorly localized knee pain
- Activity-related: Worse with impact/sports
- Swelling: Intermittent effusion, especially after activity
- Mechanical symptoms: Catching, locking (suggests unstable flap or loose body)
- Onset: Insidious, durable
Physical Examination
Inspection:
- Quadriceps atrophy (if chronic)
- Effusion (mild to moderate)
- Gait: Antalgic, tibial external rotation (to avoid impingement)
Palpation:
- Wilson's Sign: Specific but low sensitivity
- Tenderness: Over the classical site (medial femoral condyle) with knee flexed 90°
Manoeuvre: Knee flexed 90°. Internally rotate tibia. Extend knee. Positive: Pain at ~30° flexion (tibial spine impinges on MFC lesion). Relief: External rotation relieves pain (moves spine away from lesion). Note: Classic sign, but notoriously unreliable.
Investigations
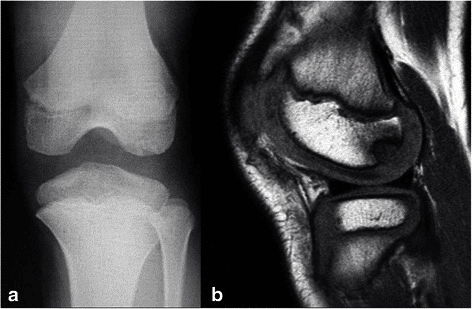
Plain Radiographs
Views: AP, Lateral, Tunnel (Notch), Skyline Findings:
- Tunnel view is most sensitive for classic MFC lesions
- Lucency: Crescent-shaped radiolucent area
- Sclerosis: Rim of sclerosis suggests chronicity
- Loose body: Calcified body in joint
- Physis: Check status (Open vs Closed)
X-rays are the initial screening tool.

Differential Diagnosis
- Key Distinguishing Features
- Adolescent athlete, vague pain, classic lateral MFC site
- Imaging Clue
- Crescent lucency + sclerotic rim; T2 rim if unstable
- Key Distinguishing Features
- Asymptomatic, posterior LFC/MFC, child under 10
- Imaging Clue
- Irregular ossification, normal cartilage, resolves with growth
- Key Distinguishing Features
- Acute trauma/patellar dislocation, haemarthrosis
- Imaging Clue
- Acute defect, no sclerotic rim, fat-fluid level
- Key Distinguishing Features
- Older adult, sudden medial pain, weight-bearing MFC
- Imaging Clue
- Subchondral oedema/collapse, no fragment rim
- Key Distinguishing Features
- Risk factors, often bilateral/multifocal
- Imaging Clue
- Serpiginous double-line sign on MRI
- Key Distinguishing Features
- Lateral pain/clunk, may coexist with lateral OCD
- Imaging Clue
- Bow-tie sign on multiple sagittal cuts
Distal femoral ossification irregularity in children under 10 mimics OCD on the posterior condyle but is asymptomatic, has intact cartilage, and resolves with growth. Do not over-treat it.
Management Algorithm
OCD Management Pathway
Diagnose on X-ray/MRI. Determine if Juvenile (Open Physis) or Adult (Closed). Assess stability on MRI (Fluid signal).
If Juvenile + Stable: Activity modification (no impact) for 3-6 months. Serial X-ray/MRI. Success 50-70%.
If Unstable, Adult, or Failed Conservative: Surgery indicated. Assess fragment salvageability arthroscopically.
Good bone stock + cartilage: Preservation surgery. Retrograde drilling (stable), Screw/Pin Fixation (unstable).
Fragment necrotic/comminuted: Remove loose body. Perform Marrow Stimulation (Microfracture) or OATS/ACI for large defects.
Follow the pathway based on stability and physis status.
DFSSurgical Indications
Hook:Operate for DFS - Detached, Failed conservative, Skeletal maturity.
FIXTreatment Options
Hook:FIX the fragment if possible!
Surgical Technique
Retrograde Drilling
Indication: Stable lesion, failed conservative (usually Juvenile). Goal: Create vascular channels for healing without breaching cartilage. Technique:
- Fluoroscopic assistance
- K-wire drilled from extra-articular femur into the lesion
- Avoid penetrating articular surface
- Stimulates healing response
Drilling brings vascularity to the lesion.
Complications
- Risk
- 30-50% in conservative
- Prevention/Management
- Select patients carefully, ensure compliance
- Risk
- If fragment detaches
- Prevention/Management
- Surgical removal
- Risk
- Long-term risk
- Prevention/Management
- Preserve meniscus, restore articular surface
- Risk
- Prominent screws
- Prevention/Management
- Countersink well, use bioabsorbable
Postoperative Care
Rehabilitation Protocol
-
Weight Bearing:
- Drilling: Immediate WBAT (stable)
- Fixation: Touch-down for 6 weeks (protect repair)
- Grafting: Non-weight bearing 6 weeks
-
Range of Motion:
- Early passive ROM (prevents stiffness)
- CPM often used for cartilage repair
-
Return to Sport:
- Conservative: 3-6 months (MRI healing)
- Surgical: 6-9 months (bone union on CT/MRI)
- Criteria: No pain, full ROM, radiographic healing
Outcomes and Prognosis
Prognostic Factors
- Age: Strongest predictor. Open physis = Good. Closed = Poor.
- Size: Smaller lesions (less than 2cm) heal better.
- Location: Classic MFC heals better than Patella/Trochlea.
- Stability: Stable heals better than unstable.
Success Rates
- Juvenile Conservative: 50-70% healing rate.
- Drilling: 80-90% success in failed conservative juvenile.
- Fixation: 80-90% success if bone quality good.
- Excision: Poor long-term results (OA risk), good short-term pain relief.
Predicting Healing: Lesion Size and Failure Predictors
The topic states that stable juvenile lesions heal roughly 50-70% of the time and that size is a key prognostic factor — but which lesions actually fail deserves spelling out, because it sets the surgical threshold and surveillance intensity.
- Normalise the size, do not just measure it. Lesion size is best expressed relative to the femoral-condyle width (a normalised ratio) rather than as an absolute millimetre value, because a given lesion is more significant in a smaller condyle. Larger normalised lesions are less likely to heal.
- The one-in-three rule. With a standardised non-operative protocol, roughly two-thirds of stable juvenile lesions heal by six months and about one-third fail — so a stable lesion justifies a non-operative trial but does not guarantee healing.
- Predictors of failure (which lower your threshold). Beyond a larger normalised size, an effusion (swelling) and mechanical symptoms (giving-way, catching, locking) at presentation predict failure to heal; notably, chronological age alone is a weaker predictor than physeal status and these lesion features.
- Practical use. A small, quiet, stable lesion in an open-physis knee can be watched with serial imaging and activity restriction; a large lesion with an effusion or mechanical symptoms should be counselled as high-risk for failing conservative care and moved earlier toward drilling.
Q: Which stable juvenile OCD lesions are least likely to heal non-operatively? A: Larger lesions (normalised to condyle width) and those presenting with an effusion or mechanical symptoms — about a third fail a 6-month trial. Age alone is a weaker predictor than physeal status and these features, so counsel large, swollen, mechanically-symptomatic lesions toward earlier drilling.
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence roughly 15-30 per 100,000 children and adolescents; rising with year-round single-sport participation worldwide.
- Peak age 10-15 years (juvenile, open physis); a smaller adult cohort presents with closed physes.
- Male predominance approximately 2:1; bilateral in 20-30% (image the contralateral knee).
- Classic site is the lateral aspect of the medial femoral condyle; lateral femoral condyle lesions associate with discoid meniscus.
Side-by-Side Guidance
- Stance
- Mostly inconclusive/consensus
- Emphasis
- MRI to characterise; nonoperative trial for stable immature lesions; surgery if unstable/failed
- Stance
- Arthroscopic classification + treatment algorithm
- Emphasis
- Probe-based stability assessment guides drilling vs fixation
- Stance
- Lesion- and skeletal-maturity-based
- Emphasis
- Preserve fragment where possible; restoration for unsalvageable defects
- Stance
- Skeletal maturity + stability driven
- Emphasis
- Open physis and stable = conservative first; closed/unstable = surgery
Registry and Restoration Data
- OCD is a leading indication for cartilage restoration registries (e.g. German KnorpelRegister DGOU, and ICRS-aligned datasets) tracking microfracture, OAT/mosaicplasty, ACI/MACI and osteochondral allograft outcomes.
- Registry signals mirror the literature: fragment preservation and osteochondral restoration outperform excision for long-term joint survival.
High- vs Limited-Resource Practice
MRI staging, arthroscopic probing, headless/bioabsorbable fixation and advanced restoration (OAT, ACI/MACI, allograft) are routinely available, enabling fragment-preserving and biologic strategies.
Where MRI and arthroscopy are scarce, diagnosis leans on tunnel-view radiographs and clinical judgement; treatment favours activity modification, open fixation, or excision when restoration is unavailable. Late presentation increases osteoarthritis risk.
Controversies and Areas of Uncertainty
Retrograde (extra-articular) drilling spares cartilage but is technically harder and needs fluoroscopy; transarticular drilling is simpler but breaches the surface. Studies show similar healing, so the choice is largely surgeon preference.
A bright T2 rim is non-specific in juveniles (only ~11% specific per Kijowski). Many "rim-positive" paediatric lesions are stable on arthroscopy, so imaging alone should not mandate surgery.
Bioabsorbable implants avoid removal and MRI artefact but give less compression and can cause synovitis/sterile effusion. Headless metal screws give strong compression but may need removal. No clear winner.
For unsalvageable lesions, the best restoration (microfracture vs OAT/mosaicplasty vs ACI/MACI vs osteochondral allograft) is debated and size-dependent. Microfracture produces less durable fibrocartilage and is falling out of favour for larger defects.
MCQ Practice Points
Q: What is the classic location of OCD knee? A: Lateral aspect of the Medial Femoral Condyle (75%). Often cited as the lateral wall of the intercondylar notch.
Q: What is the most significant prognostic factor? A: Status of the physis. Open physis (juvenile) has significantly better prognosis than closed physis (adult).
Q: What MRI finding confirms instability? A: High T2 signal (fluid) behind the fragment. This is the 'rim sign', indicating fluid interposition and instability.
Q: What is the Wilson sign? A: Pain with internal rotation at 30 degrees flexion, relieved by external rotation. (Tibial spine impinges on MFC lesion).
Q: Mechanism of retrograde drilling? A: Stimulates vascular access to the necrotic subchondral bone without breaching the overlying articular cartilage.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 13-year-old male football player presents with vague knee pain. X-ray shows a classic OCD lesion on the lateral MFC. Physes are wide open. MRI shows no fluid behind the fragment. How do you manage him?”
“A 25-year-old man presents with locking and catching. MRI shows a focal defect on the MFC with fluid behind a large osseous fragment. The cartilage hinge is intact on one side.”
“The 13-year-old from the first scenario returns at 6 months. Despite strict compliance, he still has pain. MRI shows the lesion size is unchanged, but no fluid signal. What is your next step?”
Key Concepts
- Lateral aspect of Medial Femoral Condyle (75%)
- Juvenile (open physis) = Good prognosis
- Adult (closed physis) = Poor prognosis
- MRI Fluid behind fragment = Unstable
Classification
- Juvenile Stable: Greater than 50% heal with rest
- Juvenile Unstable: Fixation/Drilling
- Adult: Almost always surgical
- Stage III/IV: Unstable/Loose body
Treatment
- Conservative: Activity mod 3-6mo (Juv Stable)
- Drilling: Retrograde (Stable, failed conservative)
- Fixation: Screw/Pin (Unstable, salvageable)
- Excision: Loose body (Unsalvageable)
Imaging
- X-ray: Tunnel view best for MFC
- MRI: T2 Rim sign (Fluid) = Unstable
- MRI: Assess cartilage integrity
- Serial MRI: Follow healing
Clinical
- Vague activity-related pain
- Wilson Sign: Pain IR 30°, relieved ER
- Mechanical symptoms = Instability
- Antalgic gait (external rotation)
Evidence Base
Healing Potential of Stable Juvenile OCD
- Two-thirds (66%) of stable juvenile lesions heal at 6 months
- Larger normalised lesion size predicts failure to heal
- Swelling/mechanical symptoms at presentation predict failure
- Standardised 6-month nonoperative trial is justified
Internal Fixation of Unstable Juvenile OCD
- 84.6% healing rate with internal fixation
- Even detached fragments healed when fixed
- Mean union time 6 months
- Supports preservation over excision for salvageable fragments
Fragment Excision vs Restoration: Long-term OA
- Excision: 70% OA at 30 years vs 51% with preservation
- Excision independently predicts OA (HR 2.3)
- Older age at diagnosis is the strongest OA risk factor (HR 4.9)
- Fragment preservation/grafting protects the joint long-term
MR Instability Criteria: Juvenile vs Adult
- Classic MR instability criteria are reliable in ADULTS (100% sensitive/specific)
- Same criteria are non-specific in JUVENILES (11% specificity)
- A T2 rim in a child often reflects vascular granulation, not instability
- Interpret a high-signal rim cautiously in skeletally immature knees
Extra-articular Drilling for Stable Juvenile OCD
- 12 of 13 knees healed with full return to activity
- Retrograde drilling protects the articular surface
- Mean time to healing/return ~8.5 months
- Effective salvage when nonoperative care fails in stable lesions
Transarticular Drilling for Stable Juvenile OCD
- 15 of 19 lesions healed completely after transarticular drilling
- All patients returned to previous sporting level
- Osteochondral-type lesions less likely to heal radiographically
- Lesion morphology on CT predicts healing
AAOS Clinical Practice Guideline: Knee OCD
- Few strong recommendations - evidence base is weak
- Supports MRI characterisation of size and stability
- Nonoperative trial reasonable for stable immature lesions
- Surgery for unstable/failed lesions