Adolescent Overhead Athlete | Capitellar OCD | Stable vs Unstable Lesions
- OCD of the capitellum affects the lateral side of the distal humerus in adolescent throwers and gymnasts
- Panner disease (age under 10, entire capitellum) is self-limiting and always treated conservatively
- MRI is essential for staging: stable lesions have intact overlying cartilage, unstable lesions show fluid behind the fragment
- Stable lesions: rest from throwing/gymnastics for 3-6 months. Unstable lesions: arthroscopic evaluation and treatment
- Return to sport averages 6-12 months depending on lesion stability and treatment
- “Capitellum OCD = lateral elbow pain in an adolescent thrower or gymnast
- “Panner disease is NOT the same as OCD: younger age, whole capitulum, excellent prognosis
- “Gymnast's elbow = capitellar OCD from weight-bearing on upper extremity
- “Tender over radiocapitellar joint, pain with active supination/pronation
OCD capitellum: Age 11-16, focal capitellar defect, lateral elbow pain in thrower/gymnast. May progress to loose bodies and surgery. Panner disease: Age under 10, entire capitulum involved, self-limiting, rest only.
Stable: Intact articular cartilage, no displacement. Treated conservatively with rest. Unstable: Disrupted cartilage, loose or displaced fragment. Arthroscopic management required. MRI distinguishes the two.
The capitellum is the lateral articular surface of the distal humerus articulating with the radial head. It is almost entirely covered by articular cartilage with limited blood supply from end-arterioles, making it vulnerable to repetitive microtrauma and ischaemia.
Lateral elbow pain in an adolescent overhead athlete that worsens with activity. Tender over the radiocapitellar joint. Painful clicking or locking suggests unstable lesion with loose body. Loss of extension is common.
- Diagnosis
- Panner disease - whole capitellum flattened
- Treatment
- Rest from sport, no surgery ever needed
- Key Pearl
- Excellent prognosis, self-limiting
- Diagnosis
- OCD - focal capitellar lesion on MRI, stable
- Treatment
- Activity modification 3-6 months
- Key Pearl
- Intact cartilage on MRI = trial of rest
- Diagnosis
- OCD - unstable lesion, loose body on MRI
- Treatment
- Arthroscopic fixation or excision + drilling
- Key Pearl
- Fluid behind fragment on MRI = unstable
THROWOCD Capitellum Risk Factors
Hook:THROW: the capitellum takes the load in adolescent overhead athletes!
FOCUSOCD vs Panner Disease
Hook:FOCUS: Focal, Older, Cartilage disrupted, Unstable possible, Surgery sometimes = OCD not Panner!
Overview and Epidemiology
Osteochondritis dissecans of the capitellum is one of the most important causes of lateral elbow pain in the adolescent athlete. It is distinct from Panner disease (younger age, entire capitulum, self-limiting). The key clinical decision is determining whether the lesion is stable (treated with rest) or unstable (requiring surgery). MRI is the gold standard for this distinction. Delayed diagnosis in unstable lesions risks loose body formation, progressive arthritis, and career-ending elbow dysfunction in young athletes.
- Age: 11-16 years (peak 12-14), open physis
- Sex: Male predominant (baseball, gymnastics)
- Dominant arm: Over 80 percent involve dominant arm
- Sport: Baseball pitchers, gymnasts, racquet sports, cricket bowlers
- Bilateral: Reported in gymnasts due to symmetrical loading
- Activity restriction: Months away from sport
- Career risk: Can end overhead athletic careers if untreated
- Long-term arthritis: Radiocapitellar joint degeneration in chronic cases
- Surgery: 30-50 percent of symptomatic OCD lesions require surgical intervention
- Return to sport: 6-12 months average; not all return to prior level
Pathophysiology
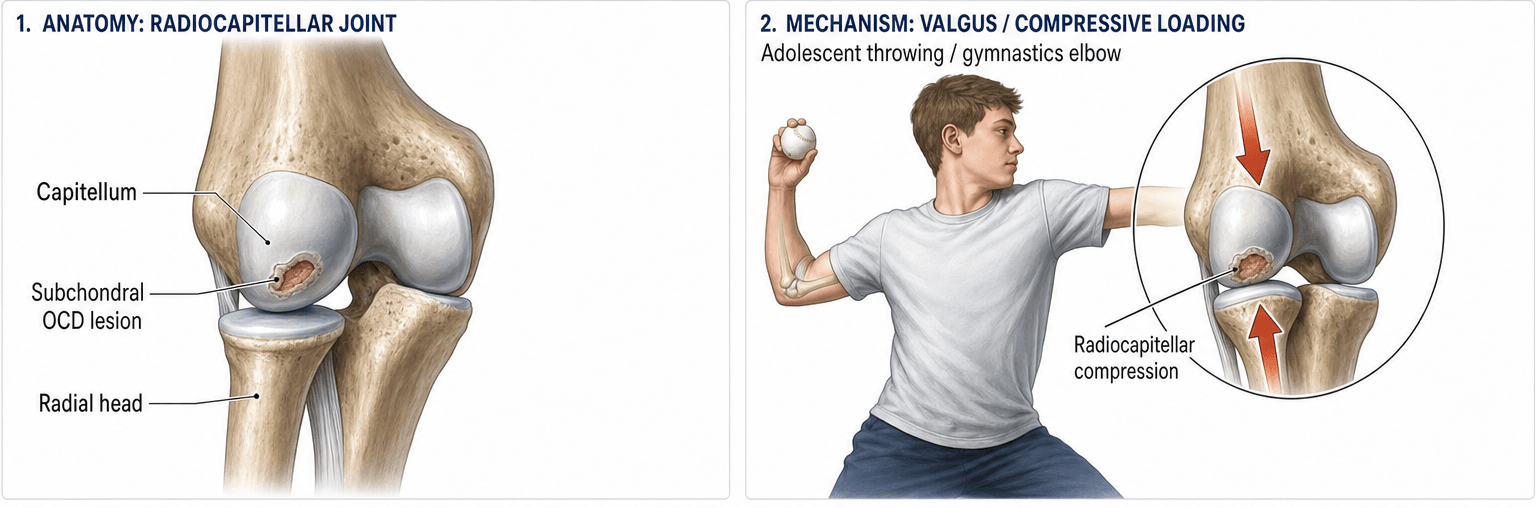
The capitellum is almost entirely covered by articular cartilage and receives its blood supply from limited end-arterioles that enter posteriorly. In the skeletally immature, the capitellar secondary ossification centre is still developing and the vascular supply is tenuous. Repetitive compressive loading (valgus stress in throwing, axial loading in gymnastics) across the radiocapitellar joint causes microtrauma to subchondral bone and compromised blood flow, leading to ischaemic necrosis of a focal segment. If loading continues, the overlying articular cartilage may separate, creating an unstable fragment or loose body.
- Mechanism
- Late cocking / early acceleration phase
- Load Type
- Valgus compression at radiocapitellar joint
- Typical Age
- 12-16 years
- Mechanism
- Weight-bearing on upper extremity (vault, bars, floor)
- Load Type
- Axial compression across radiocapitellar joint
- Typical Age
- 10-14 years
- Mechanism
- Repetitive forehand stroke, gripping
- Load Type
- Valgus and rotational compression
- Typical Age
- 11-15 years
- Mechanism
- Delivery stride, valgus stress
- Load Type
- Valgus compression, similar to baseball
- Typical Age
- 12-16 years
Limited blood supply: End-arterioles with no collateral circulation to subchondral bone
Cartilage coverage: Nearly entire capitellum is articular surface, limiting vessel access
Repetitive compression: Radiocapitellar joint bears significant compressive load during throwing
Open physis: Skeletally immature bone is less resistant to microtrauma
Ossification: The capitellar ossification centre is still maturing during peak sporting years
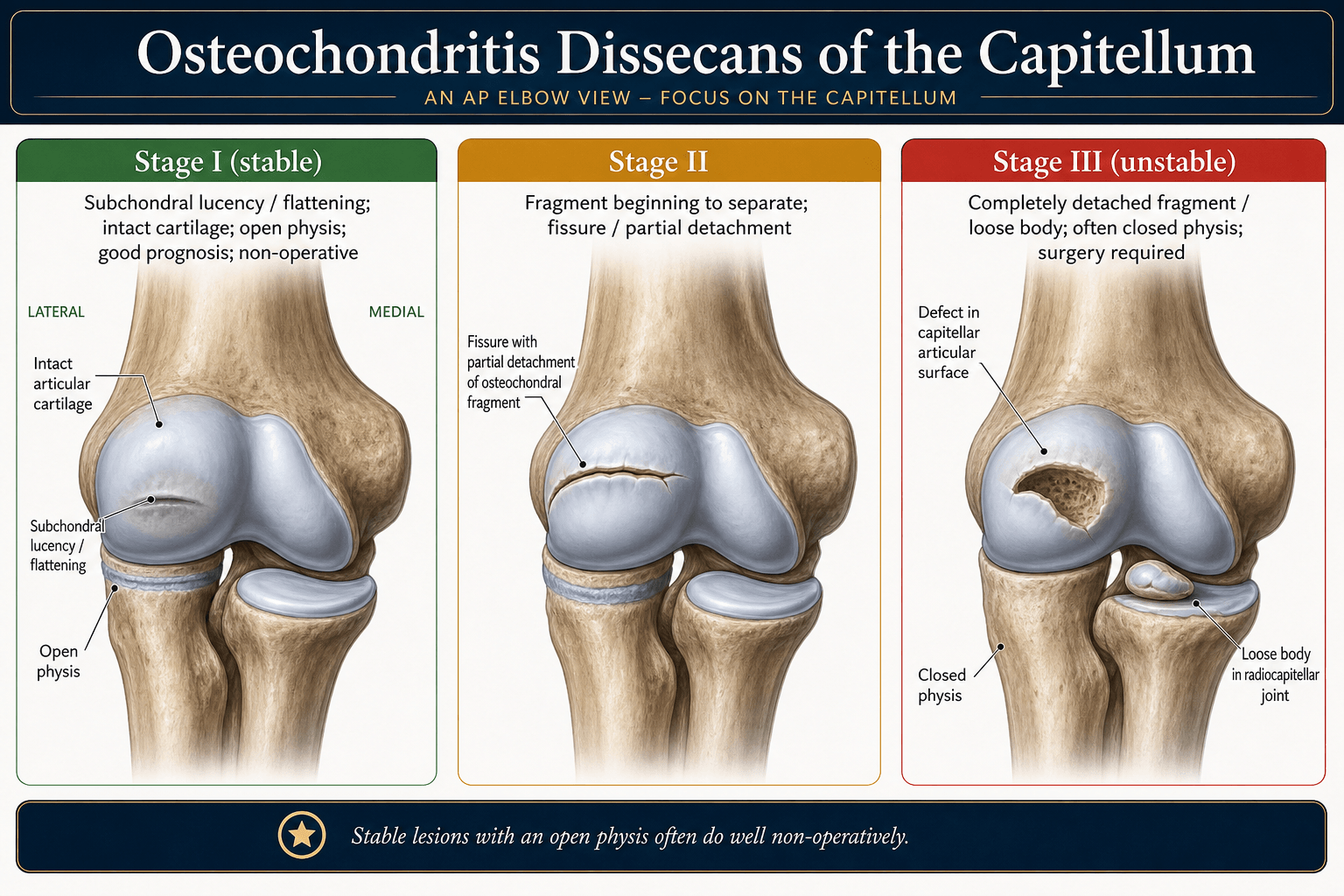
Early: Subchondral bone oedema and ischaemia (reversible with rest)
Progressive: Fragmentation of subchondral bone with intact cartilage (stable OCD)
Advanced: Cartilage breach, fragment separation (unstable OCD)
End-stage: Loose body formation, articular surface defect, early radiocapitellar arthritis
Key point: Early diagnosis and activity modification can arrest progression
Classification and Types
OCD Capitellum Classification
- Radiograph
- Radiolucent area in capitellum, flattening
- MRI Findings
- T2 hyperintensity subchondral bone, intact cartilage
- Management
- Rest, activity modification 3-6 months
- Radiograph
- Sclerosis, possible fragmentation
- MRI Findings
- Cartilage thinning/irregularity, no fluid behind fragment
- Management
- Prolonged rest, consider drilling if refractory
- Radiograph
- Visible fragment, possible loose body
- MRI Findings
- Fluid signal between fragment and bone, disrupted cartilage
- Management
- Arthroscopic evaluation, fixation or excision
- Radiograph
- Loose body in joint, defect in capitellum
- MRI Findings
- Displaced fragment, loose body, full-thickness cartilage loss
- Management
- Arthroscopic loose body removal + defect treatment
The distinction between stable and unstable is the key clinical decision point: stable lesions can heal with rest, unstable lesions generally require surgery.
The single most useful prognostic question is whether a lesion will heal non-operatively, and Takahara defined the practical predictors. A lesion is likely stable and healable with rest when all three are present: an open capitellar physis, good elbow motion (a flexion contracture under about 20 degrees), and a localised radiolucency or flattening with intact overlying cartilage. It is unstable and unlikely to heal (favouring surgery) when there is a closed or closing physis, a flexion contracture of 20 degrees or more, or radiographic fragmentation, a clear separation line, or a loose body. The physeal status is the dominant factor - the open physis still has the biological capacity to revascularise and heal, whereas a lesion in the older adolescent with a closed physis behaves like an adult osteochondral defect. So pair the MRI stability read with the physis and the ROM before committing a patient to months of rest.
STAGEMRI Staging of Capitellar OCD
Hook:STAGE your MRI read: from Signal change to Extra fragment = stable to unstable!
Clinical Assessment
- Age and sport: Adolescent overhead athlete or gymnast
- Pain location: Lateral elbow, insidious onset, worse with activity
- Mechanical symptoms: Clicking, locking, catching suggests unstable lesion
- Duration: Often present for weeks to months before seeking attention
- Throwing pattern: Year-round play, high pitch counts, no off-season
- Tenderness: Over the radiocapitellar joint (lateral elbow)
- Range of motion: Loss of extension is most common finding, possible flexion contracture
- Provocative tests: Pain with active forearm rotation (supination/pronation) against resistance
- Clicking: Palpable or audible click with motion suggests loose body
- Effusion: Mild lateral elbow swelling may be present
- Neurovascular: Typically normal; rule out radial nerve entrapment
With the elbow in extension, apply an axial load through the forearm while pronating and supinating. Pain localized to the lateral elbow is a positive test and suggests radiocapitellar joint pathology (OCD or Panner). This test compresses the radial head against the capitellum, reproducing the mechanical pain.
- Age Group
- 11-16 years
- Key Feature
- Lateral pain, insidious, overhead athlete
- Discriminating Finding
- Focal capitellar lucency on X-ray; MRI confirms staging
- Age Group
- Under 10 years
- Key Feature
- Lateral pain, acute or subacute onset
- Discriminating Finding
- Whole capitulum involved on X-ray, no loose bodies
- Age Group
- Adults (rare under 16)
- Key Feature
- Pain over lateral epicondyle, gripping
- Discriminating Finding
- No radiocapitellar tenderness, MRI normal capitellum
- Age Group
- 9-14 years
- Key Feature
- Medial elbow pain, thrower
- Discriminating Finding
- Medial epicondyle tenderness and widening on X-ray
- Age Group
- Any age (fall on outstretched hand)
- Key Feature
- Acute lateral pain, fat pad sign
- Discriminating Finding
- Acute presentation, history of trauma, fracture on imaging
- Age Group
- Young adults
- Key Feature
- Snapping over lateral elbow with motion
- Discriminating Finding
- MRI shows plica, no capitellar lesion
Any adolescent overhead athlete or gymnast with lateral elbow pain and loss of extension needs AP and lateral elbow radiographs, and if suspicious, an MRI to assess the capitellum. Do not dismiss lateral elbow pain in a young thrower as "growing pains" or "muscle strain." Early-stage OCD is reversible with rest; late-stage OCD may end an athletic career.
Investigations
Imaging Protocol
Views: AP, lateral, and oblique of the elbow. A 45-degree flexion lateral view improves capitellar visualization.
Look for: Radiolucent area in the capitellum, flattening, sclerosis, fragmentation, loose bodies.
Early OCD: May be subtle or normal on X-rays. Sclerosis and lucency develop over time.
Indication: All suspected capitellar OCD. The gold standard for staging.
Stable findings: Subchondral T2 hyperintensity, intact overlying cartilage, no fluid behind fragment.
Unstable findings: Fluid signal between fragment and underlying bone (high-signal T2 rim), disrupted cartilage, displaced fragment, loose body.
Key sign: High-signal T2 rim around the fragment = unstable lesion requiring surgical evaluation.
Indication: Pre-operative planning for surgical fixation. Better delineates bony architecture and fragment size.
Useful for: Assessing fragment size, location, and bone quality before fixation or OATS.
Not routine: Reserved for surgical planning rather than initial staging.
MRI is the gold standard for staging capitellar OCD. The critical finding is whether there is fluid signal between the fragment and the underlying bone on T2 sequences. If the cartilage is intact and there is no fluid behind the fragment, the lesion is likely stable and may heal with rest. If fluid tracks behind the fragment or cartilage is disrupted, the lesion is unstable and surgery is generally indicated. Plain radiographs alone may underestimate lesion severity.
Beyond the generic stable/unstable staging, two named systems are worth quoting. The Minami radiographic classification grades the plain film: Grade I - a translucent cystic shadow in the middle or lateral capitellum (early, stable); Grade II - a clear split line or zone of demarcation between the fragment and the adjacent subchondral bone; Grade III - a loose body with a defect in the capitellum. The arthroscopic ICRS-OCD classification grades what is seen and probed at surgery: ICRS-OCD I - intact but softened (stable) cartilage over the lesion; II - partial cartilage discontinuity, fragment stable on probing; III - complete discontinuity, a "dead in situ" but undisplaced fragment; IV - a displaced fragment or empty crater (loose body). The exam logic mirrors the MRI: a higher Minami or ICRS grade means a less stable, less healable lesion that moves you from rest toward fixation or cartilage restoration.
Management Algorithm
Stable OCD Lesions (Intact Cartilage, No Displacement)
Goal: Allow healing of the osteochondral lesion by eliminating repetitive stress on the capitellum
Conservative Treatment Protocol
Activity cessation: Stop all throwing, gymnastics, and weight-bearing through the upper extremity
Relative rest: Allow gentle daily activities, no sport
Immobilisation: Short-arm splint or sling for comfort for 2-4 weeks if acutely painful
Physical therapy: ROM exercises for elbow, wrist, and shoulder to maintain flexibility
Progressive loading: Begin gentle strengthening, avoid compressive loading across radiocapitellar joint
Repeat MRI at 3 months: Assess healing; look for resolution of bone oedema
No throwing or gymnastics: Continue activity restriction
Monitoring: Clinical review for resolution of tenderness and return of full ROM
Criteria for return: Full painless ROM, no tenderness, MRI evidence of healing
Gradual return: Begin with light tossing or low-impact gymnastics, progress over 6-8 weeks
Pitch count limits: Strict adherence to age-appropriate pitch count guidelines
Re-imaging if symptoms recur: Recurrence of pain mandates repeat MRI
Indications for surgery: Failure of 3-6 months of conservative treatment with persistent pain, no MRI evidence of healing
Options: Arthroscopic drilling (retroarticular or transarticular) to stimulate healing
Post-operative: Similar rehabilitation timeline, 6-9 months return to sport
The most important intervention is complete cessation of the offending activity. Partial rest (reducing but not stopping throwing) often fails. The athlete and family must understand that 3-6 months away from sport is necessary. Compliance is the strongest predictor of success in stable lesions.
Complications
- Incidence
- 30-50 percent of untreated unstable lesions
- Risk Factors
- Delayed diagnosis, continued sporting activity
- Management
- Arthroscopic removal + defect treatment
- Incidence
- Long-term risk, higher with larger defects
- Risk Factors
- Unstable lesion, multiple loose bodies, inadequate treatment
- Management
- Activity modification, symptomatic management
- Incidence
- 10-20 percent post-operative
- Risk Factors
- Prolonged immobilization, arthrofibrosis
- Management
- Early ROM exercises, physiotherapy
- Incidence
- 20-30 percent of initially stable lesions
- Risk Factors
- Poor compliance, continued activity, larger lesions
- Management
- Progress to surgical intervention
- Incidence
- 5-15 percent
- Risk Factors
- Poor bone stock, technical error, early loading
- Management
- Revision surgery or microfracture
The most effective strategy for capitellar OCD is prevention. Adolescent baseball pitchers should adhere to age-appropriate pitch count limits, take at least 3-4 months off from overhead throwing per year, and avoid pitching for multiple teams simultaneously. Gymnasts should have scheduled rest periods and avoid year-round training without breaks. Any lateral elbow pain in a young athlete warrants evaluation before resuming sport.
Outcomes and Prognosis
- Expected Outcome
- Good healing in 70-85 percent with full rest
- Return to Sport
- 6-9 months with full compliance
- Long-term
- Good if lesion heals, low arthritis risk
- Expected Outcome
- Healing in 70-80 percent
- Return to Sport
- 6-12 months
- Long-term
- Good outcomes, comparable to conservative success
- Expected Outcome
- Union in 70-90 percent with good bone stock
- Return to Sport
- 6-9 months after union confirmed
- Long-term
- Good if union achieved, risk of late arthritis
- Expected Outcome
- Symptom improvement in 60-80 percent
- Return to Sport
- 6-12 months
- Long-term
- Fibrocartilage less durable than hyaline
- Expected Outcome
- Good pain relief in 75-90 percent
- Return to Sport
- 9-18 months
- Long-term
- Hyaline cartilage restoration, best long-term for large defects
- Expected Outcome
- Near 100 percent resolution
- Return to Sport
- 3-6 months
- Long-term
- Excellent, near-normal elbow function
Best prognosis: Younger age, stable lesion (intact cartilage), early diagnosis, complete activity cessation, high compliance
Poor prognosis: Older adolescent (near physeal closure), unstable lesion, large defect, multiple loose bodies, poor compliance with rest
Key threshold: The stability of the lesion on MRI is the most important prognostic factor. Stable lesions have a high rate of healing with rest alone, while unstable lesions almost always require surgical intervention.
Guidelines, Registries & Global Practice
- Highest incidence: Japan, United States, and countries with strong baseball cultures (Dominican Republic, Venezuela, South Korea)
- Gymnastics-associated: Worldwide, particularly in Eastern Europe, China, and the US where competitive gymnastics is prevalent
- Male predominance: Approximately 3:1, reflecting baseball participation patterns
- Dominant arm: Over 80 percent involve the dominant extremity, except in gymnasts where bilateral involvement is more common
- North America / Japan: Higher index of suspicion due to baseball prevalence; early MRI common
- Europe: More commonly seen in gymnasts and racquet sport athletes; similar treatment principles
- Resource-limited settings: Diagnosis may be delayed due to limited MRI access; radiograph-based management with longer empiric rest periods
- Universal principle: Activity cessation is the cornerstone of stable lesion management regardless of resource setting
- Diagnosis Emphasis
- MRI for all suspected cases; plain films insufficient for staging
- Stable Lesion
- Minimum 3 months rest from sport; repeat MRI to confirm healing
- Unstable Lesion
- Arthroscopic evaluation; fixation if salvageable, OATS for large defects
- Diagnosis Emphasis
- Early MRI standard; high suspicion in baseball players
- Stable Lesion
- Conservative first; drilling for refractory cases
- Unstable Lesion
- Fragment fixation preferred; OATS for large defects
- Diagnosis Emphasis
- Clinical assessment and MRI; differentiate from Panner
- Stable Lesion
- Activity modification with physiotherapy; surgical if 6 months fails
- Unstable Lesion
- Arthroscopic management; microfracture or OATS
- Diagnosis Emphasis
- Radiographic and MRI staging; classify stable vs unstable
- Stable Lesion
- Conservative protocol with defined milestones
- Unstable Lesion
- Fixation principles per fragment size; cartilage restoration as needed
The most widely endorsed prevention strategy across societies is adherence to age-appropriate pitch count limits and mandatory rest periods in youth baseball. USA Baseball and the AOSSM have published pitch count guidelines by age group. Similar principles apply to gymnastics training volumes. The common message: year-round single-sport participation without rest periods is the strongest modifiable risk factor for capitellar OCD.
Record in every case of suspected capitellar OCD:
- Patient age, sport, training volume, and dominant arm
- MRI staging with explicit comment on cartilage integrity and fragment stability
- Treatment plan with expected duration of activity restriction
- Follow-up imaging schedule
- Counselling regarding compliance and consequences of premature return
Missed or delayed diagnosis of unstable capitellar OCD leading to loose body formation and arthritis is a source of medicolegal concern globally. Early MRI and appropriate staging are essential.
Controversies & Areas of Uncertainty
When 3-6 months of rest fails for a stable lesion, the role of drilling (retroarticular vs transarticular) versus continued conservative management is debated. No high-quality randomised trials guide this decision. Most experts recommend drilling before fragment excision.
Microfracture is simpler and less morbid but produces fibrocartilage. OATS restores hyaline cartilage but requires a graft harvest (knee or rib) with donor-site morbidity. Choice depends on defect size, patient demand, and surgeon experience. No head-to-head RCTs exist.
There is no universally agreed set of objective criteria for return to sport after OCD treatment. Most surgeons use a combination of pain-free ROM, imaging evidence of healing/union, and functional sport-specific testing, but protocols vary widely.
Cell-based therapies (autologous chondrocyte implantation, stem cell injections) are being explored for capitellar OCD but remain experimental without strong evidence supporting their use over established surgical techniques.
MCQ Practice Points
Q: A 12-year-old baseball pitcher has lateral elbow pain. Radiographs show a radiolucent lesion in the capitellum. What is the next most appropriate investigation? A: MRI of the elbow. MRI is the gold standard for staging capitellar OCD. It determines whether the lesion is stable (intact cartilage, no fluid behind fragment) or unstable (disrupted cartilage, fluid behind fragment), which directly guides management.
Q: A 7-year-old presents with lateral elbow pain. Radiographs show flattening and fragmentation of the entire capitulum. No loose bodies are seen. What is the diagnosis? A: Panner disease. Age under 10, involvement of the entire capitulum, and absence of loose bodies are characteristic. Panner disease is an osteochondrosis (analogous to Perthes disease of the hip) and is self-limiting with rest. No surgery is indicated.
Q: What is the most important conservative measure for stable capitellar OCD? A: Complete cessation of the offending activity (throwing, gymnastics, weight-bearing). Partial rest (reducing but not stopping activity) often fails. A minimum of 3 months of complete activity restriction is required, with repeat MRI to assess healing before gradual return.
Q: What MRI finding indicates that a capitellar OCD lesion is unstable and likely requires surgery? A: Fluid signal (high T2 intensity) between the fragment and the underlying bone, indicating disruption of the articular cartilage and fragment mobility. This is the most reliable MRI sign of instability. Other signs include displaced fragments and loose bodies.
Q: Why is the capitellum vulnerable to OCD in young athletes? A: The capitellum has limited end-arterial blood supply and is almost entirely covered by articular cartilage, restricting vessel access. In skeletally immature athletes, the ossification centre is still developing. Repetitive compressive loading at the radiocapitellar joint (valgus stress in throwing, axial loading in gymnastics) causes microtrauma and ischaemia in the vulnerable subchondral bone.
Q: What is the typical timeline for return to sport after surgical fixation of an unstable capitellar OCD lesion? A: 6-9 months after confirmation of fragment union on imaging. Rehabilitation involves 6 weeks of protected motion, followed by progressive strengthening and gradual return to throwing or gymnastics over months. Return to the same competitive level is not guaranteed.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 13-year-old right-handed baseball pitcher presents with 6 weeks of right lateral elbow pain, worsened by throwing. He has lost 10 degrees of extension and is tender over the radiocapitellar joint. AP and lateral radiographs show a radiolucent area in the capitellum with surrounding sclerosis. MRI shows subchondral T2 hyperintensity with intact overlying cartilage and no fluid behind the fragment. What is the diagnosis and management?”
“A 15-year-old competitive gymnast presents with a 4-month history of progressive lateral right elbow pain, intermittent clicking, and one episode of the elbow locking in 70 degrees of flexion. She has 15 degrees of flexion contracture and radiocapitellar tenderness. Radiographs show a capitellar defect with a possible loose body in the olecranon fossa. MRI demonstrates a full-thickness cartilage defect with a displaced fragment and fluid signal around the lesion. How would you manage this?”
Key Diagnosis
- Adolescent overhead athlete (11-16) with lateral elbow pain and loss of extension
- Panner disease: under 10, whole capitulum, self-limiting, never operate
- OCD: focal lesion, may become unstable, may need surgery
- MRI is gold standard for staging: fluid behind fragment = unstable
OCD vs Panner
- Age: OCD 11-16, Panner under 10
- Lesion: OCD focal, Panner whole capitulum
- Loose bodies: OCD yes, Panner never
- Treatment: OCD stable=rest, unstable=surgery; Panner always conservative
Management Algorithm
- Stable (intact cartilage): complete rest 3-6 months, repeat MRI
- Stable refractory: arthroscopic drilling
- Unstable with salvageable fragment: arthroscopic fixation
- Unstable with non-viable fragment: excision + microfracture or OATS
Surgical Options
- Fixation: bioabsorbable pins or headless compression screws for large viable fragments
- Microfracture: for small defects, produces fibrocartilage
- OATS: for larger defects, restores hyaline cartilage, best for high-demand athletes
- All procedures: arthroscopic or mini-open, 6-12 months return to sport
Exam Traps
- Don't confuse Panner disease with OCD: different age, treatment, prognosis
- Don't treat unstable lesions conservatively: surgery is indicated
- Don't rely on radiographs alone: MRI is essential for staging
- Don't allow premature return to sport: risks progression and re-injury
Evidence Base and Key Trials
Nonoperative treatment for osteochondritis dissecans of the capitellum
- Non-operative treatment was effective for stable lesions in the majority of immature athletes
- Unstable lesions had significantly worse outcomes with conservative treatment alone
- Early diagnosis and activity modification were key predictors of successful nonoperative management
- Return to sport was higher in the stable lesion group compared to unstable
Autologous osteochondral mosaicplasty for osteochondritis dissecans of the elbow in teenage athletes
- Autologous osteochondral mosaicplasty using plugs from the lateral femoral condyle for capitellar OCD
- Good to excellent results in the majority of teenage athletes at mid-term follow-up
- Hyaline cartilage restoration demonstrated on post-operative MRI assessment
- Most athletes returned to competitive sport, with improved elbow function scores
The arthroscopic classification and treatment of osteochondritis dissecans of the capitellum
- Arthroscopic classification system for capitellar OCD guiding treatment decisions
- Drilling of stable lesions refractory to conservative management showed good healing
- High rate of lesion healing and return to sport in the majority of patients
- Recommended as an intermediate step between failed conservative care and fragment excision
Classification, treatment, and outcome of osteochondritis dissecans of the humeral capitellum
- Classification system based on fragment stability guiding treatment for capitellar OCD
- Fragment fixation achieved union in the majority of cases with adequate bone stock
- Better outcomes when fragment is large enough for stable internal fixation
- Clinical outcomes declined with longer follow-up in patients with residual defects
Treatment Strategies and Outcomes for Osteochondritis Dissecans of the Capitellum
- Systematic review of surgical treatments for capitellar OCD including drilling, fixation, excision, and OATS
- OATS demonstrated the highest rate of return to sport among surgical options
- Fragment fixation had good union rates but variable return to sport
- Excision alone had lower return to sport rates compared with restoration procedures