OLT | Talar Dome Cartilage + Subchondral Bone | Size-Driven Treatment
- Most OLTs are post-traumatic - typically after an inversion ankle sprain or fracture; a minority are atraumatic (idiopathic/vascular)
- The posteromedial talar dome is the commonest site - medial lesions tend to be deeper and cup-shaped; lateral lesions are shallower, wafer-shaped and more clearly trauma-related
- MRI is the key investigation - it shows cartilage, subchondral bone oedema, fragment stability and cysts; CT best shows bony detail and cysts; plain films miss many lesions
- Asymptomatic / incidental lesions are managed non-operatively - not every talar dome lesion needs surgery
- Lesion size and stability drive treatment - small stable lesions do well with bone marrow stimulation (microfracture); large or cystic lesions favour osteochondral grafting (OAT) or cartilage restoration
- Always look for and correct malalignment - uncorrected varus/valgus overload causes graft failure and recurrent symptoms
- “OLT is usually post-traumatic - ask about a previous ankle sprain or fracture
- “Posteromedial dome is the commonest location; MRI is the best single test
- “Small stable lesions to microfracture; large/cystic lesions to OAT or cartilage restoration
- “Lesion size around 10-15mm is the rough switch-point from BMS to grafting
- “Correct any varus/valgus malalignment or the graft/repair will fail
Most OLTs are post-traumatic. Persistent deep ankle pain, catching or swelling weeks to months after an "ankle sprain" that will not settle should prompt MRI. The injury is frequently missed on the initial plain radiographs.
Lesion size and stability decide treatment. Small, stable lesions do well with bone marrow stimulation (microfracture). Large, deep or cystic lesions (roughly over 10-15mm) do better with osteochondral autograft transfer (OAT) or cartilage restoration. Quote the size threshold in viva.
MRI characterises cartilage, subchondral oedema, fragment stability and cysts. CT is superior for bony detail and measuring cystic defects. Plain radiographs underestimate or miss lesions - do not rely on them alone.
Uncorrected hindfoot/ankle malalignment overloads the lesion. A varus or valgus ankle must be corrected (e.g. supramalleolar or calcaneal osteotomy) or any repair/graft will fail. This is a classic "what else would you do?" viva point.
- Typical lesion
- Any size, no symptoms
- First-line treatment
- Non-operative + observe
- Notes
- Not every lesion needs surgery
- Typical lesion
- Under ~10-15mm, no large cyst
- First-line treatment
- Arthroscopic debridement + bone marrow stimulation (microfracture)
- Notes
- Good short-term results; cheap, one-step
- Typical lesion
- Over ~10-15mm, deep/cystic, or failed BMS
- First-line treatment
- Osteochondral autograft (OAT/mosaicplasty) or cartilage restoration (ACI/MACI)
- Notes
- Replaces the osteochondral unit
- Typical lesion
- Intact cartilage cap, subchondral cyst
- First-line treatment
- Retrograde drilling or fragment fixation (e.g. bone peg)
- Notes
- Preserves native cartilage
- Typical lesion
- Any size + varus/valgus
- First-line treatment
- Add corrective osteotomy
- Notes
- Failure to realign causes recurrence
There are TWO classifications you must keep separate. Berndt-Harty is the original radiographic staging (I-IV) and consistently underestimates the true lesion. Hepple is the MRI-based staging (1-5) that reflects modern practice. In a viva, lead with size and stability - the size of the lesion and whether the fragment/cartilage is stable matter more for the actual treatment decision than the stage number.
TALUSOLT Key Features
Hook:TALUS: Trauma, Anteromedial pain, Location posteromedial, Unstable?, Scan with MRI!
SLABWhy Repairs Fail
Hook:SLAB: Size too big, Lateral/cystic, Alignment uncorrected, BMI/patient factors!
Overview and Epidemiology
An osteochondral lesion of the talus (OLT) is a defect involving the articular cartilage and the underlying subchondral bone of the talar dome. The terms osteochondral lesion, osteochondral defect, osteochondritis dissecans and transchondral fracture overlap and are often used interchangeably; "osteochondral lesion of the talus" is the preferred modern umbrella term because it does not assume a single cause.
Definition
Osteochondral lesion of the talus (OLT): an injury or defect of the talar dome that affects both:
- The articular cartilage (the smooth bearing surface), and
- The subchondral bone beneath it (which can develop oedema, cysts or a detached fragment).
Epidemiology and aetiology
- Most lesions are post-traumatic. According to PubMed, OLTs typically occur after a traumatic injury - classically an inversion ankle sprain or an ankle fracture - and are best diagnosed on MRI (Anastasio 2023).
- A minority are atraumatic (idiopathic), where repetitive microtrauma with local vascular impairment is thought to play a role.
- Common in young, active patients - the same population that sustains ankle sprains and sports injuries.
- Frequently missed early - because plain radiographs often look normal, an OLT is a classic cause of an "ankle sprain that will not settle."
- Associated with chronic ankle instability - recurrent inversion injuries expose the talar dome to repeated shear.
An OLT is the classic explanation for persistent deep ankle pain after a "simple sprain." If pain, catching or swelling continue beyond the expected recovery of a sprain, image with MRI. Do not keep re-labelling it as a soft-tissue injury.
Pathophysiology, Anatomy and Blood Supply
Talar dome and cartilage
The talus is largely covered by articular cartilage and has no muscular attachments, so it relies on a precarious blood supply that enters around its neck. The talar dome articulates with the tibial plafond and the medial and lateral malleoli to form the ankle (tibiotalar) joint.
The cartilage of the talar dome is relatively thin, and like all hyaline cartilage it has poor intrinsic healing capacity because it is avascular. Once the cartilage and subchondral plate are breached, repair depends on cells reaching the defect - which is the rationale behind bone marrow stimulation.
Why location matters
- Medial lesions
- More common (posteromedial)
- Lateral lesions
- Less common (anterolateral)
- Medial lesions
- Deeper, cup-shaped
- Lateral lesions
- Shallower, wafer-shaped
- Medial lesions
- Often present, sometimes atraumatic
- Lateral lesions
- Almost always clearly traumatic
- Medial lesions
- Inversion + plantarflexion (posteromedial)
- Lateral lesions
- Inversion + dorsiflexion (anterolateral)
Pathophysiology
- Initial injury - shear or compression across the talar dome (during a sprain or fracture) damages cartilage and the subchondral plate.
- Subchondral response - oedema develops; the fragment may stay in place (stable) or partially separate.
- Cyst formation - synovial fluid is driven into the subchondral bone through the cartilage breach, forming subchondral cysts over time.
- Progression - a stable lesion may remain quiet, while an unstable or cystic lesion causes mechanical symptoms and, if untreated, can lead to ankle osteoarthritis.
The talus has no muscle attachments and a tenuous blood supply, and its cartilage cannot heal itself. This biology explains both why lesions persist and why treatments aim either to recruit marrow cells (microfracture) or to physically replace the osteochondral unit (OAT/grafting).
Classification Systems
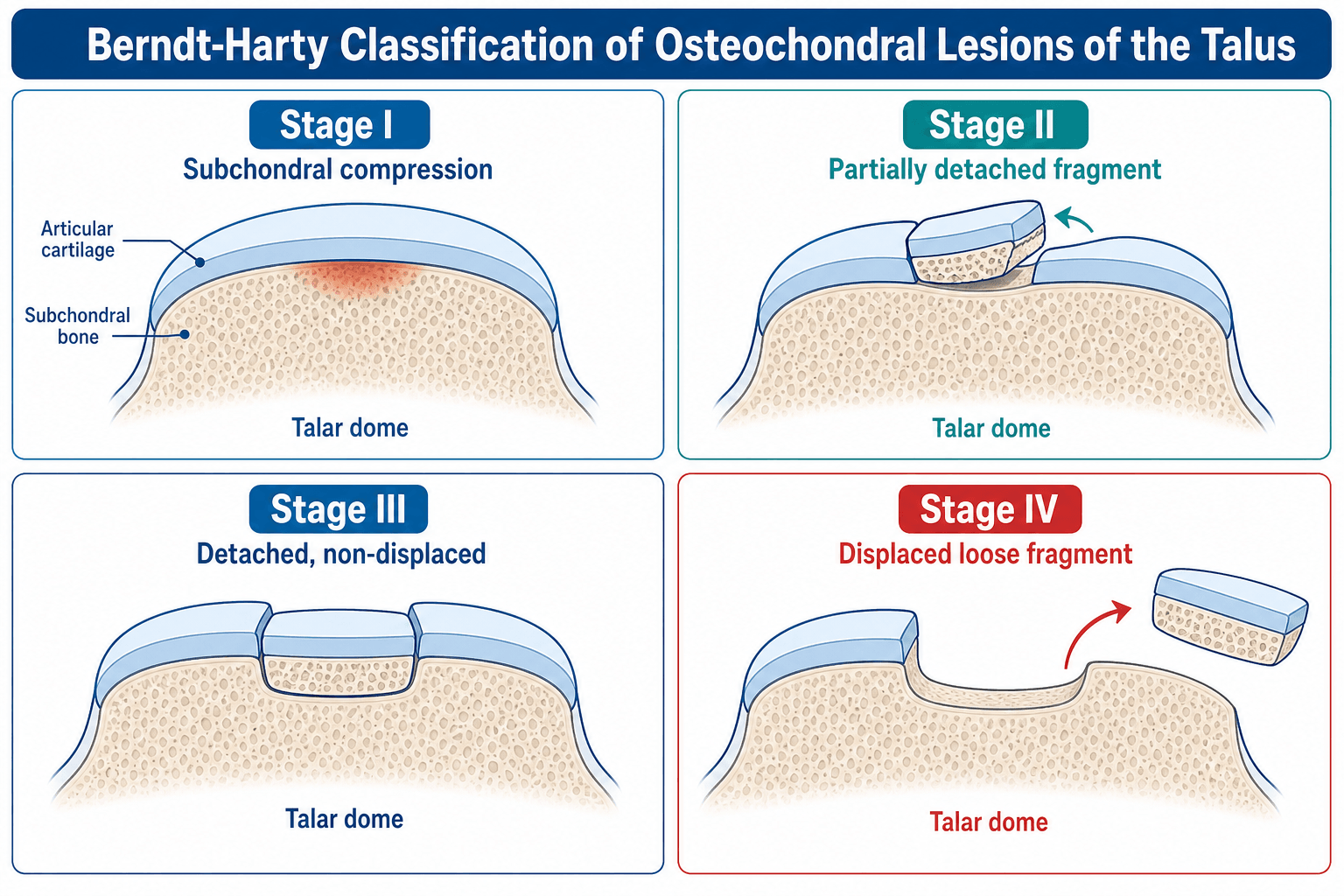
Berndt-Harty - the original radiographic staging
The historic plain-film staging describes progressive separation of an osteochondral fragment:
- Stage I - small area of subchondral compression
- Stage II - partially detached osteochondral fragment
- Stage III - completely detached fragment, but not displaced (remains in its crater)
- Stage IV - detached and displaced fragment
Limitation: plain radiographs frequently miss or underestimate the lesion, so the Berndt-Harty stage often understates the true cartilage and subchondral damage seen on MRI or at arthroscopy.
Clinical Presentation and Assessment
History
- Deep, poorly localised ankle pain - typically worse with weight-bearing and activity.
- Antecedent trauma - a previous ankle sprain or fracture in most cases. Ask specifically about a sprain that never fully recovered.
- Mechanical symptoms - catching, locking, clicking or a sense of giving way, suggesting an unstable fragment or loose body.
- Recurrent swelling after activity.
- Chronic ankle instability - recurrent inversion injuries point to both the cause and a target for treatment.
Examination
- Tenderness over the anteromedial or anterolateral talar dome, palpated with the ankle plantar/dorsiflexed to bring the dome forward.
- Effusion / swelling of the ankle.
- Range of motion - often preserved; pain at extremes.
- Ligament assessment - test for lateral ligament laxity (anterior drawer, talar tilt) because instability frequently coexists and may need addressing.
- Alignment - assess hindfoot and ankle alignment (varus/valgus) on standing, as malalignment changes management.
A complete OLT assessment includes ligamentous stability and hindfoot alignment, not just dome tenderness. Coexisting instability or malalignment must be treated to protect any cartilage procedure.
Investigations
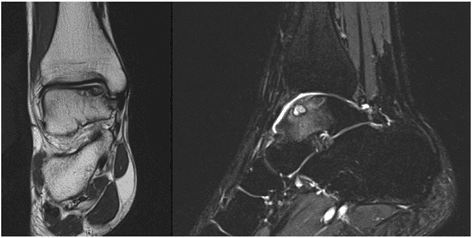
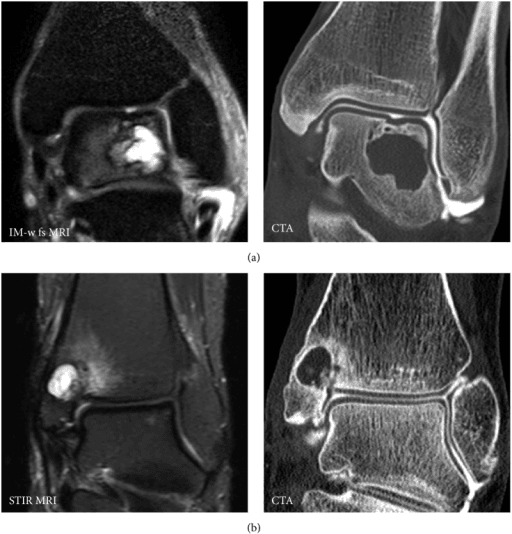
MRI - the best single test
MRI is the investigation of choice because it shows the cartilage, the subchondral bone, oedema, fragment stability and cysts in one study, and is the recommended way to diagnose an OLT.
Key MRI features:
- Bone marrow oedema beneath the lesion (a marker of an active, often symptomatic lesion).
- Cartilage integrity - intact cap versus fissured or detached cartilage.
- Fragment stability - a high-signal (fluid) line completely encircling a fragment suggests instability.
- Subchondral cysts (Hepple stage 5), which usually push treatment toward grafting.
Management Algorithm
Stepwise management
Osteochondral Lesion of the Talus Management
Incidental or asymptomatic lesions are best treated non-operatively - reassurance, activity modification and monitoring. Not every talar dome lesion needs surgery.
Relative rest, activity modification, a period of protected weight-bearing, physiotherapy and analgesia. A trial of conservative care is reasonable for many stable symptomatic lesions before surgery.
Arthroscopic debridement and microfracture / drilling. Reliable short-term improvement for small lesions; cheap and one-step.
Osteochondral autograft transfer (OAT/mosaicplasty), or autologous chondrocyte implantation (ACI/MACI), or osteochondral allograft for very large defects.
Correct varus/valgus with a supramalleolar or hindfoot osteotomy so the repaired surface is not overloaded.
DRAFTTreatment Ladder
Hook:DRAFT: Debride+drill, Retrograde drilling, Autograft, Fix fragment, Transplant + Tidy alignment!
Surgical Technique
Arthroscopic bone marrow stimulation
- Ankle arthroscopy (anteromedial and anterolateral portals; +/- distraction).
- Debride unstable cartilage back to a stable, vertical rim.
- Curette the calcified cartilage layer off the base of the lesion.
- Microfracture / drill the subchondral plate to create channels that release marrow elements, which form a fibrocartilage repair (note: fibrocartilage, not true hyaline cartilage).
- Protected weight-bearing postoperatively with early range-of-motion.
Best suited to small, stable lesions; results are good in the short term but may deteriorate over time, particularly for larger lesions.
Biologic and Scaffold Augmentation of Bone Marrow Stimulation
Standard microfracture heals a defect with mechanically inferior fibrocartilage rather than true hyaline cartilage, and its results deteriorate over time and with larger lesions. This has driven interest in augmenting bone marrow stimulation rather than abandoning it - a strategy this topic's own complication data points to (the Hollander meta-analysis found matrix-assisted bone marrow stimulation carried the lowest complication rate of any technique, about 3 percent).
The augmentation options
- Platelet-rich plasma (PRP) - concentrated autologous platelets deliver growth factors to the microfractured base. In a Level I randomised trial of talar lesions, a single postoperative PRP injection added to arthroscopic microfracture gave significantly better pain and function than hyaluronic acid or saline (Görmeli 2015).
- Concentrated bone marrow aspirate (cBMAC) - supplements the marrow released by the microfracture channels with additional mesenchymal stromal cells and growth factors.
- Scaffold-augmented / matrix-assisted bone marrow stimulation (AMIC - autologous matrix-induced chondrogenesis) - a collagen or hyaluronan membrane is laid over the microfractured base to stabilise the marrow clot and support a more organised repair, extending the technique to slightly larger lesions where bare microfracture would fail.
- Hyaluronic acid - a viscosupplement adjunct; in the same randomised trial it outperformed saline but was inferior to PRP.
The general cartilage-repair biology and the science of PRP and scaffolds belong to the dedicated cartilage topics; what matters for the talus specifically is that these adjuncts are used to stretch the size ceiling of a one-step marrow-stimulation procedure and to make the fibrocartilage repair more durable before committing the patient to grafting.
PRP as an adjunct to microfracture (randomised trial)
- PRP as an adjunct to microfracture beat hyaluronic acid and saline
- Both PRP and hyaluronic acid improved outcomes over control
- Authors recommend PRP as the primary adjunct after talar microfracture
If asked "how might you improve a microfracture result," name biologic and scaffold augmentation - PRP or concentrated bone marrow aspirate, and matrix-assisted bone marrow stimulation / AMIC (a membrane over the microfractured base). These aim to make the fibrocartilage repair more durable and to stretch the size ceiling of a one-step procedure; matrix-assisted BMS also had the lowest complication rate in the largest meta-analysis.
Complications
Complications of OLT and its treatment
- Persistent or recurrent pain - the commonest reason for revision; often due to an undersized procedure, a large/cystic lesion, or uncorrected malalignment.
- Nerve injury - the most frequently reported complication after OLT surgery (e.g. injury to cutaneous nerves around portals or approaches).
- Failure / need for revision surgery - higher with larger lesions and with biologics added to bone marrow stimulation in some series.
- Donor-site morbidity - knee pain after harvesting OAT plugs.
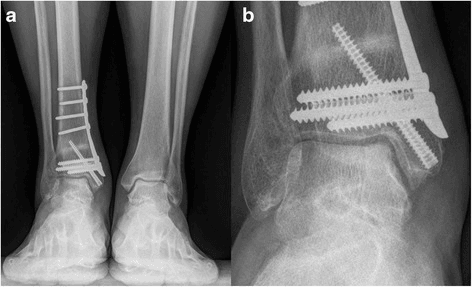
- Malleolar osteotomy problems - nonunion, malunion or hardware irritation when an osteotomy is used for access.
- Subchondral cyst formation / progression - especially if the lesion is incompletely treated.
- Ankle osteoarthritis - the long-term consequence of an untreated or failed lesion.
Across surgical techniques for OLT, the overall complication rate is roughly 1 in 20 patients, and nerve injury is the most commonly observed complication; metal implants carry a notably higher complication rate than other techniques (Hollander/Dahmen meta-analysis of 6,962 lesions).
Postoperative Care and Rehabilitation
Principles
- Protected weight-bearing - a period of non- or partial weight-bearing protects the repair while it matures; the duration depends on the procedure (longer for grafting/osteotomy than for simple debridement).
- Early range of motion - controlled ankle motion encourages cartilage health and prevents stiffness.
- Progressive loading - gradually advance to full weight-bearing as pain and healing allow.
- Physiotherapy - regain strength, proprioception and balance; address any ankle instability that contributed to the lesion.
- Graded return to sport - typically several months; return is guided by symptoms, strength and imaging when needed.
Whatever the procedure, the postoperative theme is the same: offload while it heals, then progressively reload and rehabilitate, and fix the underlying instability or malalignment so the lesion does not recur.
Outcomes and Prognosis
What to quote
- Bone marrow stimulation gives good short-term results for small, stable lesions, but outcomes are strongly size-dependent - smaller lesions (around under 10mm) do significantly better than larger ones (Guo 2010).
- Osteochondral autograft (OAT) produces good long-term clinical and MRI outcomes, with significant improvements in pain and function maintained at long follow-up; results are worse when OAT is used as a salvage after previous failed surgery (Imhoff 2011).
- Patient and lesion factors affect outcome - higher age, BMI and larger lesion size are associated with poorer results and higher failure rates (Anastasio 2023; Dekker 2017).
- Surgery is generally safe - no life-threatening complications are reported, and the overall complication rate is around 5% (Hollander/Dahmen 2023).
Outcomes are best when the lesion is small, the alignment is corrected, and it is a primary (not salvage) procedure. Large lesions, malalignment and prior failed surgery all predict poorer results.
Critical Lesion Size: Area, Diameter and the Microfracture Threshold
The topic repeatedly says "size drives treatment" and quotes both a diameter (roughly 10-15mm) and an area (over 125mm2, Dekker) - but these are two different measurements, and it is worth knowing where the numbers come from and why the area is the more discriminating figure.
The classic critical size
- Choi 2009 studied 120 ankles after arthroscopic bone marrow stimulation and found a sharp threshold at a defect area of about 150mm2: only around 10 percent of lesions smaller than 150mm2 failed, versus roughly 80 percent of lesions of 150mm2 or larger. Patient age, symptom duration, trauma and lesion location did not predict outcome - size did.
- Ramponi 2016 systematically reviewed 25 studies (1,868 ankles) and refined the guidance: bone marrow stimulation is best reserved for lesions with an area under about 107mm2 and/or a diameter under about 10mm, tightening the older "150mm2 or 15mm" figure.
- Dekker 2017 (already cited) similarly found cartilage-graft failure rose sharply once lesion area exceeded 125mm2.
Why area, not just a single diameter
A lesion is rarely a perfect circle, and a single "widest diameter" can badly under- or over-state the true defect. Measuring the area (and, ideally, the volume - including depth and any cyst) on MRI or CT captures how much bearing surface is actually lost, which is why the area thresholds correlate with outcome more reliably than a lone diameter. In practice: measure the lesion on cross-sectional imaging, and if it is around 1 cm2 or larger (or deep/cystic), lean toward grafting rather than microfracture.
The defensible viva answer is that lesion area predicts microfracture success: the classic critical size is about 150mm2 (Choi), tightened by systematic review to roughly 107mm2 in area or 10mm in diameter (Ramponi). Above this, expect bone marrow stimulation to fail and plan for osteochondral grafting or cartilage restoration.
Critical defect size for poor outcome after marrow stimulation
- Defect area around 150mm2 is a critical threshold for poor outcome
- Failure jumped from about 10 percent to about 80 percent above the threshold
- Size predicted outcome; age, duration, trauma and location did not
Guidelines, Registries & Global Practice
Global epidemiology. Osteochondral lesions of the talus are most common in young, active patients and are usually post-traumatic, classically following an inversion ankle sprain or an ankle fracture. They are a leading cause of persistent ankle pain after a sprain worldwide. There is no implant registry for OLT - the evidence is pooled case series, systematic reviews and consensus statements, so practice is consensus-driven globally.
Side-by-side guidance
- Diagnosis emphasis
- MRI for diagnosis and staging; CT for bony detail
- First-line surgery
- Bone marrow stimulation for small lesions
- Distinctive point
- Size and stability drive the algorithm
- Diagnosis emphasis
- CT for bony mapping of cysts and acute fragments
- First-line surgery
- Fix acute displaced fragments; BMS for small chronic lesions
- Distinctive point
- Emphasis on the osteochondral unit and alignment
- Diagnosis emphasis
- MRI as primary; high suspicion after sprains
- First-line surgery
- Microfracture small lesions; OAT for large/cystic
- Distinctive point
- Strong focus on lesion-size thresholds
- Diagnosis emphasis
- MRI + CT; assess instability and alignment
- First-line surgery
- BMS, then OAT/ACI for large lesions
- Distinctive point
- Routinely add corrective osteotomy for malalignment
High- vs limited-resource practice
Routine MRI (and often CT) to stage the lesion, ankle arthroscopy for bone marrow stimulation, and access to OAT, ACI/MACI and osteochondral allograft for large lesions, with corrective osteotomy when needed.
Diagnosis may rely on clinical suspicion plus whatever cross-sectional imaging is available; the priority is not to miss the lesion. Arthroscopic or open debridement with microfracture is a low-cost, durable first-line option, with referral for grafting when feasible.
OLT is a high-yield foot and ankle viva topic. Know that it is usually post-traumatic, commonest on the posteromedial dome, best diagnosed on MRI, and that treatment is driven by lesion size and stability: microfracture for small stable lesions and OAT or cartilage restoration for large/cystic ones. Always mention correcting malalignment and assessing instability, distinguish Berndt-Harty (X-ray) from Hepple (MRI), and remember nerve injury is the commonest surgical complication.
MCQ Practice Points
Q: What is the commonest location of an osteochondral lesion of the talus? A: The posteromedial talar dome. Medial lesions tend to be deeper and cup-shaped; lateral (anterolateral) lesions are shallower, wafer-shaped and more clearly traumatic.
Q: What is the best single investigation for an OLT? A: MRI - it shows cartilage, subchondral bone oedema, fragment stability and cysts. CT is best for bony detail and cyst size; plain radiographs frequently miss the lesion.
Q: How does lesion size guide treatment? A: Small, stable lesions (roughly under 10-15mm) do well with bone marrow stimulation (microfracture); larger or cystic lesions favour osteochondral autograft (OAT) or cartilage restoration. Size is a strong predictor of outcome.
Q: What is the most commonly reported complication after OLT surgery? A: Nerve injury. The overall complication rate is around 5%, and metal implants carry the highest rate (about 15%).
Q: How do Berndt-Harty and Hepple classifications differ? A: Berndt-Harty is the original radiographic staging (I-IV) and underestimates the lesion; Hepple is the MRI-based staging (1-5, where stage 5 is a subchondral cyst). Modern decisions also rely heavily on lesion size and stability.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old recreational footballer presents with deep medial ankle pain and intermittent swelling 5 months after an inversion ankle sprain. Plain radiographs were reported as normal at the time. On examination there is tenderness over the medial talar dome and a small effusion. How would you investigate and manage this?”
“A 32-year-old presents with ongoing pain 18 months after arthroscopic microfracture for a medial talar OLT. Repeat MRI shows a 14mm posteromedial lesion with a subchondral cyst (Hepple stage 5). The hindfoot is in slight varus. What are the options and what would you do?”
“A 14-year-old gymnast has activity-related ankle pain. MRI shows a posteromedial talar dome lesion with an intact cartilage cap and a small underlying subchondral cyst, with no fluid line around the fragment (stable, in situ). How does management differ in this age group?”
Key Concepts
- Defect of cartilage + subchondral bone of the talar dome
- Usually post-traumatic (inversion sprain or fracture)
- Commonest location: posteromedial talar dome
- MRI is the best single investigation
Classification
- Berndt-Harty (X-ray): I compression to IV displaced - underestimates lesion
- Hepple (MRI): 1 cartilage injury to 5 subchondral cyst
- Modern decisions: lesion size + stability
- Rough switch-point ~10-15mm: BMS below, grafting above
Treatment
- Asymptomatic / incidental: observe
- Small stable symptomatic: debridement + microfracture (BMS)
- Large or cystic / failed BMS: OAT (mosaicplasty) or ACI/MACI; allograft for very large
- Stable in-situ lesion / juvenile: retrograde drilling or fragment fixation (bone peg)
- Always correct varus/valgus malalignment
Surgical Technique
- Microfracture: debride to stable rim, curette calcified layer, perforate subchondral plate (yields fibrocartilage)
- OAT: posteromedial access often needs medial malleolar osteotomy; press-fit hyaline plug flush
- Retrograde drilling: stimulate healing without breaching intact cartilage cap
- Fixation: reduce and fix a viable fragment to preserve native cartilage
Complications
- Nerve injury (commonest surgical complication)
- Persistent/recurrent pain and need for revision
- Donor-site knee morbidity (OAT)
- Malleolar osteotomy nonunion/malunion; subchondral cysts; ankle OA
Evidence Base
Comprehensive review: aetiology, classification, treatment and outcomes
- Most OLTs are post-traumatic; MRI is the diagnostic test of choice
- Asymptomatic / incidental lesions are managed conservatively
- Outcomes depend on age, BMI and lesion characteristics
Lesion size predicts success of arthroscopic treatment
- 81% good/excellent results after arthroscopic debridement + microfracture
- Lesions under 10mm did significantly better than larger lesions
- Medial vs lateral location did not significantly change outcome
Long-term outcomes of osteochondral autograft (OATS)
- Significant, durable improvement in pain and function at ~7 years
- Good graft integration on MRI predicts better clinical scores
- OATS as a salvage procedure does worse than as a primary procedure