Cartilage Lesions | MACI | OAT | Restoration
- Medial femoral condyle is most common location
- ICRS grading classifies cartilage damage
- Microfracture for small (less than 2cm²) contained lesions
- MACI/ACI for larger lesions (greater than 2-4cm²)
- OAT (mosaicplasty) for small-moderate lesions
- “Address alignment, meniscal, and ligament issues concurrently
- “Microfracture produces fibrocartilage (Type I collagen)
- “ACI/MACI produces hyaline-like cartilage (Type II)
- “OAT transfers hyaline cartilage with bone from non-weight-bearing area
Small lesions (less than 2cm²). Marrow stimulation. Creates fibrocartilage (Type I collagen). Good short-term but deteriorates at 5+ years. Contained lesion ideal.
Larger lesions (greater than 2-4cm²). Two-stage: harvest chondrocytes, culture, implant. MACI uses membrane. Produces hyaline-like cartilage. Better long-term than microfracture for large lesions.
Osteochondral autograft transfer (mosaicplasty). Small-moderate lesions. Plugs from non-weight-bearing area (trochlea, notch). True hyaline cartilage. Limited by donor site.
Osteochondral allograft. Large lesions (greater than 4cm²). Fresh allograft. Good for young patients with large defects. Disease transmission risk, availability issues.
Overview and Classification
Osteochondral defects of the knee involve damage to the articular cartilage and potentially underlying subchondral bone. Goals of treatment are pain relief, improved function, and prevention of osteoarthritis.
ICRS Classification
Grade I: Superficial softening, fibrillation Grade II: Partial thickness lesion (less than 50% depth) Grade III: Deep lesion (greater than 50% depth) or down to subchondral bone Grade IV: Full thickness with exposed subchondral bone
Grade III and IV are generally treated.
Location
Medial femoral condyle (MFC): Most common weight-bearing location for symptomatic lesions. Patellofemoral (patella/trochlea) lesions are next most frequent and behave differently — they tolerate microfracture poorly and ACI/MACI has historically had less reliable results here.
Differential Diagnosis of a Focal Knee Lesion
A focal cartilage/subchondral signal change on MRI is not always a treatable osteochondral defect. Distinguish the following before committing to a restoration procedure.
- Typical Patient / Clue
- Young, post-traumatic or insidious; mechanical pain
- Key Imaging Feature
- Sharp-bordered cartilage defect ± exposed bone, ICRS III-IV
- Distinguishing Point
- Discrete, well-shouldered lesion in otherwise healthy joint - the restoration candidate
- Typical Patient / Clue
- Adolescent/young adult; classic lateral aspect of medial femoral condyle
- Key Imaging Feature
- Subchondral fragment with crescentic lucent interface
- Distinguishing Point
- Bone-side process; stability (T2 rim, cysts) drives treatment, not size alone
- Typical Patient / Clue
- Older patient (over 55), acute medial pain, often female
- Key Imaging Feature
- Subchondral insufficiency fracture line, oedema on weight-bearing MFC
- Distinguishing Point
- Not a graft candidate; often related to insufficiency fracture/meniscal root tear
- Typical Patient / Clue
- Older, diffuse/bipolar wear
- Key Imaging Feature
- Joint-space narrowing, osteophytes, bipolar cartilage loss
- Distinguishing Point
- Diffuse not focal - cartilage restoration contraindicated; consider osteotomy/arthroplasty
- Typical Patient / Clue
- Acute trauma
- Key Imaging Feature
- Reticular subchondral oedema, intact cartilage
- Distinguishing Point
- Self-limiting; treat the injury, not the signal
- Typical Patient / Clue
- Middle-aged, popping injury or insidious
- Key Imaging Feature
- Root signal, meniscal extrusion, secondary MFC oedema
- Distinguishing Point
- Drives rapid chondral overload; repair the root rather than chase the cartilage
Pathophysiology
Articular (hyaline) cartilage is avascular, aneural and alymphatic, and adult chondrocytes have very limited mitotic capacity. Consequently a full-thickness chondral injury that does not reach the subchondral vascular bed mounts essentially no intrinsic repair and persists as a defect.
- Partial-thickness (chondral) injury — no access to marrow, no clot, no healing response; the defect remains and the rim degenerates over time.
- Full-thickness osteochondral injury — breaches the subchondral plate, allowing a marrow clot with mesenchymal stem cells to fill the defect. This heals with mechanically inferior fibrocartilage (Type I collagen) rather than true hyaline cartilage (Type II) — the biological basis of microfracture and its long-term deterioration.
Once cartilage is lost, increased peak contact stress accelerates degeneration of adjacent cartilage, and abnormal load transfer to subchondral bone produces marrow oedema and cysts — the substrate for progression toward focal then generalised osteoarthritis. Anything that raises focal contact stress (malalignment, meniscal deficiency, instability) magnifies this cascade, which is why concurrent pathology must be corrected.
ANAWhy Focal Cartilage Defects Do Not Heal
Hook:ANA = cartilage is Avascular, has No mitosis, Aneural - so it cannot self-repair.
Clinical Presentation
- Symptoms: activity-related, often localised joint-line or anterior pain; effusion after activity; mechanical symptoms (catching, locking, giving way) suggest an unstable fragment or loose body.
- History: young/active patient, prior trauma, twisting injury, or insidious onset; ask about prior knee surgery (especially meniscectomy or ACL reconstruction) and any previous cartilage procedure.
- Examination: focal condylar or patellofemoral tenderness, effusion, possible crepitus; always assess limb alignment (varus/valgus, gait thrust), meniscal signs and ligament stability — these determine whether any cartilage procedure can succeed.
- Red flags against restoration: diffuse/bipolar pain, older age with established OA, inflammatory features.
Investigations
- Weight-bearing radiographs (AP, lateral, skyline, and a Rosenberg/45° flexion PA view) — assess joint space, exclude established OA, look for OCD or loose bodies.
- Long-leg standing alignment films — mandatory before any restoration procedure to quantify mechanical axis; uncorrected malalignment is a leading cause of failure.
- MRI — the key modality: maps cartilage lesion location, size and depth (ICRS grade), subchondral bone status (oedema, cysts), and concurrent meniscal/ligament pathology. Cartilage-sensitive sequences and quantitative mapping (e.g. T2/dGEMRIC) assess repair tissue on follow-up.
- Diagnostic arthroscopy — defines the true ICRS grade, lesion size, containment and shoulder quality, and is often the staging step (chondrocyte harvest) for ACI/MACI.
Lesion size measured intra-operatively at arthroscopy is frequently larger than the MRI estimate — never finalise a size-based treatment plan from imaging alone, and consent the patient for the next technique up.


Treatment Options
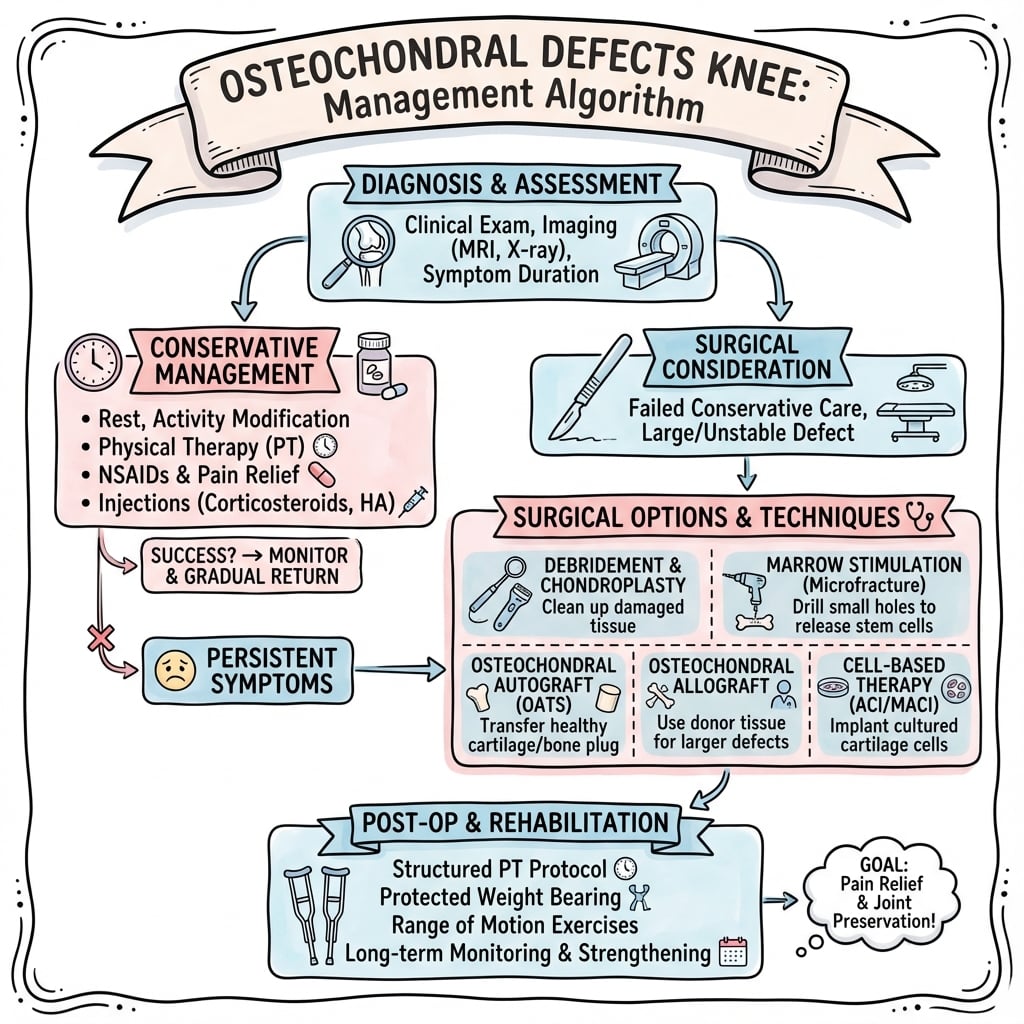
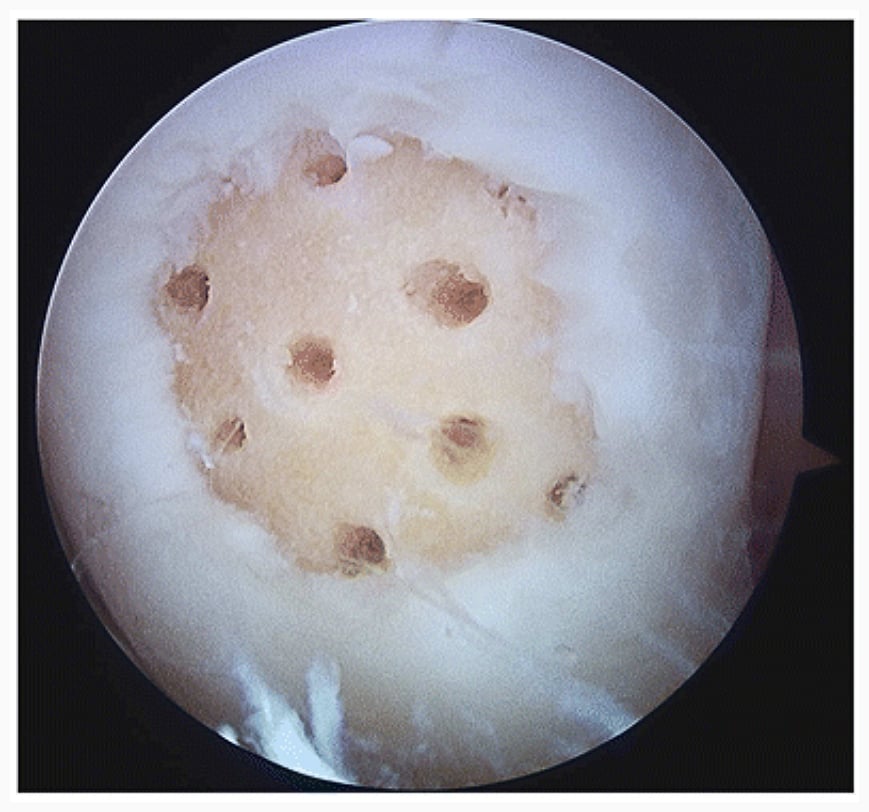
Mechanism: Create holes in subchondral bone. Marrow elements (MSCs, blood) fill defect. Forms fibrocartilage.
Indications: Small lesions (less than 2cm², ideally less than 1.5cm²). Contained with healthy shoulder. First-line for small lesions.
Technique: Debride edges to stable margins. Create microfracture holes 3-4mm apart, 3-4mm deep.
Outcomes: Good short-term (2-5 years). Deteriorates over time. Fibrocartilage (Type I collagen) less durable than hyaline (Type II).
Key Considerations
Address Concurrent Pathology
Alignment: Varus/valgus malalignment must be corrected (HTO, DFO). Uncorrected alignment leads to failure.
Meniscus: Meniscal deficiency increases contact stress. Consider MAT if previous meniscectomy.
Ligaments: ACL deficiency causes abnormal kinematics. Reconstruct if unstable.
Patient Selection
- Young (typically under 40-50)
- Active, motivated
- Single compartment disease
- Focal lesion (not diffuse OA)
- Normal or correctable alignment
- Stable knee
Lesion Containment and Shoulder Quality
The microfracture indications, the investigations section and the management algorithm all use "contained" lesion and healthy "shoulder" as selection criteria - the algorithm's decision node is literally "lesion size and containment" - but the concepts are never defined, and they decide which technique can work.
- Containment. A contained lesion is surrounded on all sides by an intact peripheral rim (wall) of healthy cartilage. That wall is what holds a marrow clot (microfracture/AMIC) or an ACI/MACI graft inside the defect - it is essential for those techniques to succeed.
- Uncontained lesions have a deficient rim - typically at the very edge of a condyle, at a bipolar ("kissing") lesion, or where the shoulder has broken down. A clot or cell graft cannot be retained, so marrow stimulation and cell therapy do poorly here; these lesions favour structural replacement that does not need a containing wall - OAT or osteochondral allograft, which bring their own bone and cartilage.
- Shoulder quality. The "shoulder" is the transition between the defect and the surrounding cartilage. A good shoulder is healthy, full-thickness cartilage firmly anchored to subchondral bone, so the surgeon can debride the lesion to stable vertical walls and create a well-contained defect. A poor shoulder (soft, fibrillated, delaminating or undermined cartilage) makes the "contained" appearance illusory - the walls will not hold a repair, which predicts failure of marrow stimulation and again favours OAT/OCA.
- Practical point: assess containment and shoulder quality at arthroscopy, together with size, before committing to a technique - a small lesion with a poor shoulder is not a good microfracture candidate.
Q: What do "contained" and "shoulder quality" mean and why do they matter? A: A contained lesion has an intact healthy cartilage rim on all sides that can hold a marrow clot or a cell graft in place - a prerequisite for microfracture, AMIC and ACI/MACI. An uncontained lesion (rim deficient - condylar edge, bipolar, or a broken-down shoulder) cannot retain a clot/graft, so it favours structural options that bring their own wall (OAT, osteochondral allograft). The "shoulder" is the surrounding cartilage-to-defect transition; only a healthy, well-anchored shoulder lets you debride to stable vertical walls, so a poor shoulder predicts marrow-stimulation failure regardless of lesion size.
AMIC and Scaffold-Augmented Marrow Stimulation
The Controversies section flags "augmented marrow stimulation (scaffold-assisted / AMIC)" as the response to microfracture's declining reputation, but never explains what it is.
- AMIC = autologous matrix-induced chondrogenesis. It combines standard marrow stimulation (microfracture or drilling) with a collagen type I/III membrane (or scaffold) laid over the defect and sealed, usually with fibrin glue. The membrane protects and stabilises the marrow clot - which is otherwise prone to washout and uneven fill - and provides a three-dimensional scaffold that organises the marrow-derived mesenchymal cells as they differentiate.
- Why it exists. It targets microfracture's two weaknesses (an unstable clot with variable fill, and mechanically inferior fibrocartilage) while staying a single-stage, cell-culture-free, lower-cost procedure - unlike the two-stage, regulated and expensive ACI/MACI. It is therefore attractive where cell therapy is unavailable or unaffordable.
- Where it sits. Usually offered for medium (roughly 2 to 4 cm2) contained lesions where microfracture alone is unreliable but a two-stage cell therapy is not warranted or accessible; some surgeons extend it to larger contained defects.
- Evidence. Medium-term series report better and more durable defect fill than microfracture alone, but there is little high-level randomised evidence against MACI/ACI, so its precise place in the algorithm remains an area of active study - exactly the "augmented marrow stimulation" the controversies section refers to.
Q: What is AMIC and where does it fit between microfracture and MACI? A: Autologous matrix-induced chondrogenesis = marrow stimulation plus a collagen I/III membrane sealed over the defect to protect the clot and scaffold the marrow cells. It is single-stage and cell-culture-free (cheaper/simpler than two-stage ACI/MACI) and addresses microfracture's clot washout and poor fill. It is used mainly for medium contained lesions (about 2 to 4 cm2); medium-term data show better fill than microfracture, but high-level comparison with MACI is still lacking.
Complications
Procedure failure / persistent symptoms is the dominant concern — graft delamination, incomplete fill or progression to OA, ultimately leading to revision restoration or arthroplasty.
- Microfracture: subchondral bone overgrowth, intralesional osteophyte, subchondral cysts, and fibrocartilage breakdown with symptom recurrence at 2-5 years.
- OAT / mosaicplasty: donor-site morbidity, plug subsidence/proud plugs, surface incongruity, dead space between plugs ("valleys"), limited graft availability for large lesions.
- ACI / MACI: graft hypertrophy or delamination, periosteal patch overgrowth (older ACI), prolonged rehabilitation, two procedures and cost; possible incomplete integration.
- OCA: graft non-incorporation/collapse, immunologic and (rare) disease-transmission risk, dependence on chondrocyte viability that falls with storage time.
- General: infection, arthrofibrosis/stiffness, VTE, and accelerated degeneration if concurrent malalignment, meniscal deficiency or instability is left uncorrected.
GRAFTCauses of Cartilage Procedure Failure
Hook:A cartilage repair fails for GRAFT reasons - the biggest avoidable ones are missed Realignment and Absent meniscus.
Guidelines, Registries & Global Practice
Global Epidemiology
- Full-thickness chondral lesions are found in roughly 5-11% of knee arthroscopies, and some degree of cartilage damage in up to 60% — most are incidental, only a minority are symptomatic, focal and treatable.
- Symptomatic defects cluster in active patients in their 20s-40s; the medial femoral condyle is the most common symptomatic site, followed by the patellofemoral joint.
- Traumatic and sport-related chondral injury predominates in younger patients, while degenerative/diffuse lesions in older patients are not restoration candidates.
Side-by-Side Guidance
- Position on cartilage repair of the knee
- Emphasises matching technique to lesion size and addressing concurrent malalignment, meniscal and ligament pathology; acknowledges limited high-level comparative evidence between techniques
- Position on cartilage repair of the knee
- ACI/MACI supported for selected symptomatic defects in patients without significant OA who have not had prior cartilage repair, in specialist centres; microfracture positioned for small lesions
- Position on cartilage repair of the knee
- Stresses staged correction of alignment and meniscal deficiency before/with cartilage restoration; subchondral bone preservation
- Position on cartilage repair of the knee
- Provide the ICRS grading framework and decision algorithms driven by lesion size, depth, containment and patient demand
Registry & Outcome Notes
- Dedicated cartilage-repair registries are less mature than arthroplasty registries, but national joint registries (NJR, AJRR, AOANJRR, Swedish/Norwegian) capture the key downstream endpoint: conversion of a prior cartilage procedure to arthroplasty, informing real-world failure and survivorship.
- Long-term RCT data (Knutsen 2016) is more sobering than early single-arm series — both microfracture and first-generation ACI show substantial failure and radiographic OA at 14-15 years.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: full menu available — microfracture/AMIC, OAT, two-stage MACI/ACI and fresh OCA, with combined osteotomy/MAT where indicated. Cell-therapy products (e.g. MACI) require regulatory approval and tissue-bank/lab infrastructure that is not universal.
- Limited-resource settings: marrow stimulation (microfracture/drilling) and OAT/mosaicplasty dominate because they are single-stage, low-cost and require no cell culture or allograft banking. Cultured-chondrocyte and fresh-allograft options are often unavailable, making patient selection and concurrent biomechanical correction even more important.
Exam Relevance (global)
- A core topic across FRCS (Tr & Orth), FRACS, EBOT/FEBOT, ABOS and DNB/MS curricula.
- Vivas test the ICRS/Outerbridge grading, the size-based treatment algorithm, and — most importantly — the principle that alignment, meniscal and ligament status must be assessed and corrected for any cartilage procedure to succeed.
Controversies & Areas of Uncertainty
- Does cartilage restoration prevent osteoarthritis? The honest answer is uncertain. The Knutsen 14-15 year RCT showed early radiographic OA in roughly half of survivors regardless of whether they had ACI or microfracture, and no difference in total knee replacement. Restoration improves symptoms but its disease-modifying claim is unproven — counsel patients accordingly.
- First-line for the 2-4 cm² "grey-zone" lesion. Microfracture, OAT and MACI all have advocates here. Microfracture is cheapest and single-stage but produces fibrocartilage; OAT gives true hyaline bone-cartilage but is donor-limited; MACI gives hyaline-like tissue but is two-stage and costly. No single technique is definitively superior across this whole range.
- Microfracture's declining reputation. Concerns about subchondral bone overgrowth, intralesional osteophytes and subchondral cysts after marrow stimulation have narrowed its indications toward truly small (under 2 cm²) contained lesions, and have driven interest in "augmented" marrow stimulation (scaffold-assisted / AMIC).
- Patellofemoral lesions remain the hardest subgroup. Historically poorer ACI results (Brittberg 1994) have improved with modern matrix techniques and concurrent patellofemoral realignment/unloading, but the evidence base is thinner than for the femoral condyle.
- OCA graft viability and access. Fresh osteochondral allograft depends on chondrocyte viability that falls with storage time, and availability/regulation of fresh allograft varies enormously between countries — a major practical determinant of which option a surgeon can actually offer.
- Biologics (PRP, BMAC, stem-cell injections). Widely marketed as cartilage "regenerators" but lacking high-level evidence for true cartilage restoration; current role is adjunctive symptom management at best.
MCQ Practice Points
Q: What lesion size thresholds guide treatment selection for osteochondral defects?
A: Less than 2 cm²: Microfracture or drilling preferred. 2-4 cm²: OATS (osteochondral autograft) or ACI (autologous chondrocyte implantation). Greater than 4 cm²: ACI or osteochondral allograft (fresh). Microfracture produces fibrocartilage (Type I collagen), while ACI/OATS produce hyaline-like cartilage (Type II collagen).
Q: What is the ICRS classification for cartilage lesions?
A: Grade 0: Normal. Grade 1: Superficial lesions (soft, fissures). Grade 2: Less than 50% depth. Grade 3: Greater than 50% depth, not reaching subchondral bone. Grade 4: Full thickness with exposed subchondral bone. Guides treatment: Grade 3-4 lesions with symptoms are candidates for cartilage restoration procedures.
Q: What are the advantages and disadvantages of OATS versus ACI?
A: OATS advantages: Single-stage, immediate hyaline cartilage, structural bone support. OATS disadvantages: Donor site morbidity, limited graft availability, plug mismatch. ACI advantages: Larger lesions, no donor morbidity. ACI disadvantages: Two-stage, requires periosteal flap or collagen membrane, expensive.
Q: What MRI findings indicate an unstable osteochondritis dissecans lesion?
A: Unstable OCD signs: High T2 signal rim surrounding fragment (fluid interface), cystic changes in subchondral bone, breach of articular cartilage, loose body formation. Unstable lesions require surgical fixation or fragment removal. Stable lesions may be treated nonoperatively in skeletally immature patients.
Q: What is the preferred harvest site for OATS in the knee?
A: Lateral femoral trochlea (superolateral, above sulcus terminalis) and intercondylar notch. These areas are non-weight-bearing. Harvest plugs perpendicular to surface. Maximum 2-3 plugs to avoid significant donor morbidity. Plug diameter typically 6-10mm. Match recipient site curvature.
At a Glance
Osteochondral defects involve damage to articular cartilage and underlying subchondral bone, with the medial femoral condyle (MFC) being the most common weight-bearing location. Treatment selection is size-dependent: microfracture for small lesions (less than 2cm²) produces fibrocartilage (Type I collagen), while MACI/ACI for larger lesions (greater than 2-4cm²) produces hyaline-like cartilage (Type II). OAT (mosaicplasty) transfers true hyaline cartilage with bone from non-weight-bearing areas. Critical principle: always address concomitant alignment, meniscal, and ligamentous pathology for successful outcomes.
SIZETreatment Selection by Size
Hook:SIZE determines treatment: Small = microfracture/OAT, Large = MACI/OCA!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old has a 3cm² full-thickness cartilage defect on the medial femoral condyle. Knee is stable with normal alignment. What are your treatment options?”
“You are seeing a 32-year-old recreational footballer in your clinic 3 years after he underwent arthroscopic microfracture for a 1.8cm² ICRS grade IV cartilage defect on the medial femoral condyle. At the time, microfracture was appropriate given the lesion size (under 2cm²) and he was a suitable candidate - young, active, stable knee with normal alignment. He did well initially, returning to football at 9 months post-operatively with significant improvement in his knee pain. However, over the past 6-8 months, his medial knee pain has gradually returned and is now limiting his ability to play football. He has tried physiotherapy, activity modification, and NSAIDs with minimal benefit. On examination, he has medial joint line tenderness, a small effusion, and pain with deep knee flexion. Range of motion is full (0-135°). His knee is stable to ligamentous examination and there is no malalignment on standing alignment. You order an MRI which shows deterioration of the previously treated cartilage lesion - the microfractured area now has poor fill with irregular surface and underlying bone marrow edema. The lesion measures approximately 2.2cm² (slightly larger than original). There is no evidence of other cartilage damage, meniscal pathology, or ligamentous injury. The patient is frustrated and asks what can be done - he wants to continue playing football. How do you counsel him and what is your management plan?”
“You are seeing a 35-year-old woman in your knee reconstruction clinic who was referred by a colleague. She has severe medial knee pain following a skiing injury 4 years ago where she sustained an ACL rupture which was reconstructed at the time. However, her pain has progressively worsened despite a stable ACL reconstruction. She has tried conservative management including physiotherapy, weight loss (BMI now 28, down from 32), activity modification, and multiple courses of injections with minimal sustained benefit. She is now unable to walk more than 500 meters without severe pain and has had to stop her active lifestyle completely. On examination, she has marked medial joint line tenderness, moderate effusion, full range of motion (0-130°), stable ACL reconstruction (negative Lachman and pivot shift), but varus thrust during gait. Standing alignment films show 6° of mechanical varus with the mechanical axis passing well medial to the knee center, loading the medial compartment. MRI shows a large ICRS grade IV cartilage defect on the medial femoral condyle measuring 5cm² with significant bone marrow edema. Additionally, the MRI shows that she had a previous total medial meniscectomy (you review the notes - at the time of her ACL reconstruction 4 years ago, the medial meniscus was found to be complex and degenerative with extensive tearing, and the surgeon performed a total meniscectomy). There is no evidence of significant arthritis in other compartments - the lateral compartment is pristine. The patient is desperate for help and wants to avoid knee replacement as long as possible. A previous surgeon told her nothing could be done and she would need a knee replacement within 5 years. How do you counsel her and what is your surgical plan if you proceed?”
Treatment by Size
- Small (less than 2cm²): Microfracture, OAT
- Medium (2-4cm²): OAT, MACI
- Large (greater than 4cm²): MACI, OCA
Cartilage Quality
- Microfracture: Fibrocartilage (Type I)
- MACI/ACI: Hyaline-like (Type II)
- OAT/OCA: True hyaline with bone
Address Concurrent
- Malalignment (HTO/DFO)
- Meniscal deficiency (MAT)
- ACL instability (ACLR)
MACI
- Two-stage procedure
- Larger lesions (greater than 2cm²)
- Better than microfracture long-term
- Hyaline-like cartilage
Evidence Base
- 23 patients, full-thickness defects 1.6-6.5 cm², cultured autologous chondrocytes under periosteal flap
- 14 of 16 femoral condylar transplants good-to-excellent at 2 years
- Patellar lesions did far worse (only 2 of 7 good/excellent)
- Biopsy: hyaline-like cartilage in 11 of 15 femoral grafts vs 1 of 7 patellar
- 144 patients, symptomatic Outerbridge III-IV defects 3 cm² or larger (mean lesion 4.8 cm²)
- MACI vs microfracture; co-primary endpoint KOOS pain + function at 2 years
- MACI significantly better for both pain and function (P=.001)
- Fewer treatment failures with MACI (12.5%) than microfracture (31.9%)
- 5-year follow-up of the SUMMIT cohort (128 of 144 patients)
- MACI superiority in KOOS pain + function maintained at 5 years (P=.022)
- MRI defect fill improved in both groups with no significant difference
- No unexpected safety signals
- 80 patients, single femoral condyle defect, 14-15 year follow-up
- No significant difference between first-generation ACI and microfracture on any clinical score
- Failures: 17 (ACI) vs 13 (microfracture); more TKRs in the ACI group (6 vs 3)
- Radiographic OA (Kellgren-Lawrence 2 or greater) in roughly half of survivors in each group