LUCL Insufficiency | Elbow Dislocation Spectrum | Horii Circle Injury
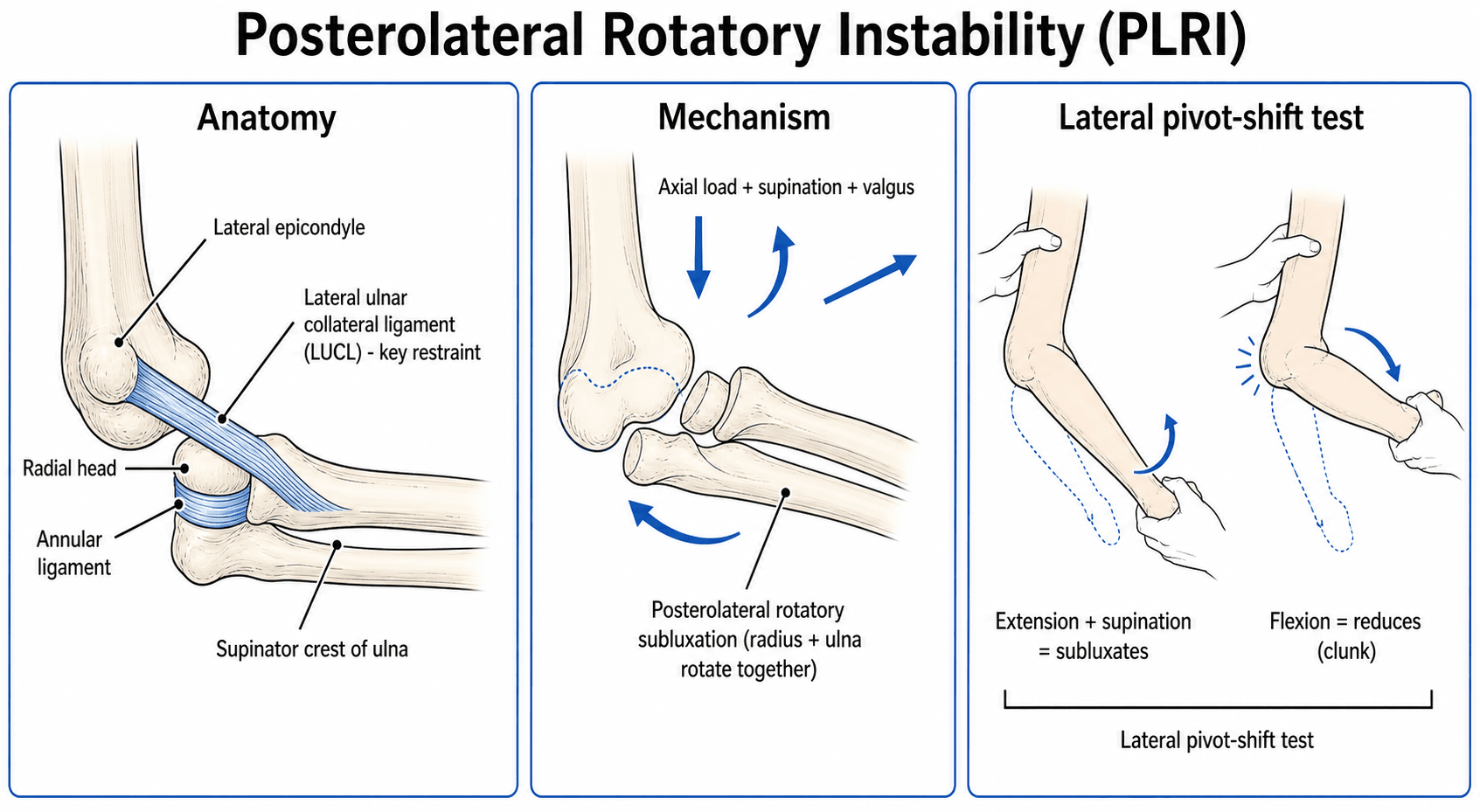
- LUCL originates from lateral epicondyle, inserts on supinator crest of ulna
- PLRI follows simple elbow dislocation or repetitive varus stress
- Pivot-shift test: patient supine, arm overhead, forearm supinated, valgus + axial load produces subluxation
- Horii circle describes sequential soft-tissue disruption from lateral to medial
- Reconstruction uses tendon graft (palmaris, gracilis, or triceps) through bone tunnels or anchors
- “PLRI often missed after simple dislocation - always test lateral stability
- “Chair push-up test and lateral pivot apprehension sign are highly sensitive
- “MRI in supination shows LUCL discontinuity and posterolateral capsule injury
- “Reconstruction indicated when instability persists beyond 3-6 months
Stage 1: LUCL tear. Stage 2: + posterolateral capsule. Stage 3: + radial collateral ligament. Stage 4: + anterior and posterior capsule. Stage 5: + medial collateral ligament (complete dislocation).
Technique: Patient supine, shoulder flexed 90 degrees, forearm fully supinated. Apply valgus and axial load while flexing from extension. Positive = radial head subluxes posterolaterally at 40-60 degrees flexion, reduces with further flexion.
Sign: Patient experiences apprehension or reproduction of instability when the forearm is supinated and a valgus force is applied in slight flexion. Highly sensitive for symptomatic PLRI.
Technique: Patient pushes up from a chair with hands on armrests, forearms supinated. Positive test = reproduction of posterolateral pain or instability sensation. Sensitivity over 90 percent in confirmed PLRI.
- Diagnosis
- Positive pivot-shift + apprehension
- Treatment
- LUCL reconstruction with graft
- Key Pearl
- Wait 3-6 months before surgery
- Diagnosis
- Chair push-up and table-top tests positive
- Treatment
- Graft reconstruction (palmaris/gracilis)
- Key Pearl
- Address any bony deficiency first
- Diagnosis
- Stress views under anesthesia
- Treatment
- Non-operative if stable post-reduction
- Key Pearl
- Reassess stability at 2-3 weeks
LATERALHorii Circle of Injury
Hook:Horii circle starts LATERAL and marches medially until the elbow dislocates!
SUPINATEPivot-Shift Test Steps
Hook:SUPINATE the forearm and feel the radial head jump back into place!
GRAFTPLRI Reconstruction Principles
Hook:GRAFT the LUCL isometrically and test stability before closure!
Overview and Epidemiology
Posterolateral rotatory instability is the most common pattern of recurrent elbow instability after simple dislocation. The lateral ulnar collateral ligament (LUCL) is the primary restraint. Missed or undertreated PLRI leads to chronic pain, mechanical symptoms, and secondary osteoarthritis. Early recognition of the Horii circle injury pattern and appropriate ligament reconstruction restore stability in over 85 percent of patients.
- Simple elbow dislocation: Most common precursor (valgus-hyperextension)
- Repetitive varus stress: Overhead athletes, gymnasts
- Iatrogenic: Excessive release during lateral epicondylitis surgery
- Trauma: Direct varus blow or fall onto outstretched hand
- Mechanical instability: Clicking, clunking with supinated activities
- Pain: Posterolateral elbow, worse with loading in supination
- Secondary OA: Chronic subluxation accelerates radiocapitellar wear
- Functional loss: Difficulty with pushing, throwing, weight-bearing
Pathophysiology
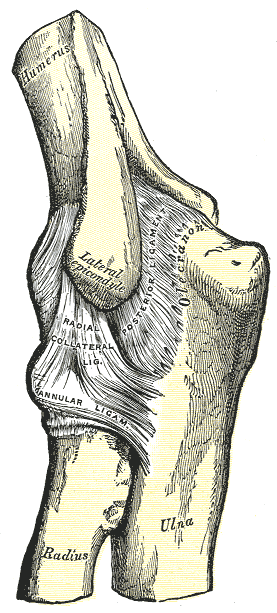
The lateral ulnar collateral ligament originates from the lateral epicondyle just distal and slightly anterior to the common extensor origin. It courses distally and inserts on the supinator crest of the proximal ulna. The LUCL is the primary static restraint to posterolateral rotatory instability. Secondary restraints include the radial collateral ligament, posterolateral capsule, and when deficient, the medial collateral ligament complex. The radial head acts as a secondary stabilizer; its excision dramatically increases PLRI risk.
- Function
- Primary restraint to external rotation of ulna
- When Deficient
- Allows posterolateral subluxation
- Clinical Relevance
- Target of reconstruction
- Function
- Resists varus and posterolateral rotation
- When Deficient
- Increases instability magnitude
- Clinical Relevance
- Often reconstructed together
- Function
- Secondary check-rein to rotation
- When Deficient
- Permits greater subluxation arc
- Clinical Relevance
- Repaired or imbricated during surgery
- Function
- Final restraint in complete dislocation
- When Deficient
- Complete dislocation occurs
- Clinical Relevance
- Rarely addressed in isolated PLRI
Stage 1: LUCL tear only - pivot-shift positive Stage 2: + posterolateral capsule - increased external rotation Stage 3: + radial collateral ligament - gross subluxation Stage 4: + anterior/posterior capsule - perched dislocation Stage 5: + MCL - complete dislocation (ulnohumeral joint)
Acute dislocation: Swelling and hemarthrosis provide temporary stability Healing potential: LUCL may heal in extension but not in supination Missed diagnosis: Patients often told "simple dislocation" and discharged Late presentation: 6-24 months later with mechanical symptoms
Classification and Types
Classification by Soft-Tissue Injury Stage
- Structures Torn
- LUCL only
- Clinical Test
- Pivot-shift positive, apprehension
- Treatment
- Non-operative trial or repair
- Structures Torn
- LUCL + posterolateral capsule
- Clinical Test
- Gross pivot-shift, clunk
- Treatment
- Reconstruction indicated
- Structures Torn
- + radial collateral ligament
- Clinical Test
- Subluxation at rest, visible prominence
- Treatment
- Graft reconstruction mandatory
- Structures Torn
- Complete dislocation, MCL involved
- Clinical Test
- Recurrent dislocation episodes
- Treatment
- Staged or combined medial-lateral reconstruction
The Horii circle concept explains why some elbows remain unstable after "simple" dislocation reduction.
The Terrible Triad of the Elbow
When an elbow dislocation is accompanied by both a radial head fracture AND a coronoid fracture, it is termed the terrible triad - so named because of its historically poor results from persistent instability and stiffness. It sits at the complex end of the same posterolateral injury spectrum as PLRI.
- The three lesions: posterolateral dislocation + radial head fracture + coronoid (usually tip) fracture, with the lateral collateral ligament avulsed off the lateral epicondyle.
- Why it is unstable: the elbow loses both its bony buttress (the coronoid anteriorly and the radial head as a posterolateral/valgus secondary stabiliser) and its primary lateral ligament restraint simultaneously.
- Structure
- Coronoid
- Principle
- Fix (suture or screw) if large; even a tip fragment via the anterior capsule helps restore the anterior buttress
- Structure
- Radial head
- Principle
- Repair if reconstructable, otherwise REPLACE - never simply excise (it is a key secondary stabiliser)
- Structure
- Lateral collateral ligament
- Principle
- Repair the avulsed LCL/LUCL back to the isometric point on the lateral epicondyle
- Structure
- Medial side / hinged fixator
- Principle
- If still unstable after the above, repair the MCL and/or apply a hinged external fixator
Q: Why must the radial head be repaired or replaced - not excised - in a terrible triad? A: With a coronoid fracture and a torn lateral collateral ligament, the radial head is the critical remaining secondary stabiliser against posterolateral and valgus subluxation. Excising it removes the last buttress and produces recurrent instability, so a reconstructable head is fixed and an unreconstructable head is replaced with a metallic prosthesis, never simply removed.
Clinical Assessment
- Index event: Simple elbow dislocation or varus injury
- Timing: When instability symptoms began after injury
- Activities: Pain or clunk with pushing, throwing, supinated loading
- Prior treatment: Immobilisation duration, therapy, injections
- Inspect: Swelling, radial head prominence, carrying angle
- Palpate: Lateral epicondyle tenderness, radial head click
- ROM: Note flexion arc, any extension loss from prior injury
- Stability tests: Pivot-shift, lateral pivot apprehension, chair push-up, table-top
Technique: Patient supine, shoulder flexed to 90 degrees, elbow extended, forearm fully supinated. Examiner applies valgus force and axial compression while slowly flexing the elbow. At approximately 40-60 degrees of flexion the radial head subluxes posterolaterally (felt as a clunk or visible prominence). Further flexion to 90-100 degrees reduces the joint with a second clunk. Key point: The test is performed under anesthesia if apprehension prevents relaxation. Sensitivity approaches 100 percent when performed correctly.
- Technique
- Supine, arm overhead, supinated forearm, valgus + axial load during flexion
- Positive Finding
- Radial head subluxes at 40-60 degrees, reduces in further flexion
- Sensitivity
- Gold standard - near 100 percent when relaxed
- Technique
- Supinated forearm, valgus stress in 20-30 degrees flexion
- Positive Finding
- Patient apprehension or reproduction of instability
- Sensitivity
- Greater than 90 percent in symptomatic PLRI
- Technique
- Push up from chair with forearms supinated
- Positive Finding
- Pain or instability sensation posterolaterally
- Sensitivity
- Greater than 90 percent sensitivity
- Technique
- Patient leans on table with elbow extended, forearm supinated
- Positive Finding
- Pain or giving-way sensation
- Sensitivity
- Useful office screening test
Lateral epicondylitis produces point tenderness at the epicondyle but negative pivot-shift and no mechanical instability. Radial tunnel syndrome causes forearm pain without instability signs. PLRI is confirmed only when the pivot-shift or apprehension tests are positive. Always perform stability testing before diagnosing "tennis elbow" in a post-dislocation patient.
Investigations
Imaging Protocol
Views: AP, lateral, oblique of elbow Look for: Radial head subluxation, coronoid fracture, radial head fracture, heterotopic ossification Clinical correlation: Many PLRI cases have normal radiographs; diagnosis is clinical
Indication: When clinical tests equivocal or under anesthesia Technique: Supinated forearm with valgus load, compare to contralateral side Positive finding: Greater than 3 mm radial head posterior translation or ulnohumeral gapping
Indication: Pre-operative planning, confirm LUCL tear, assess cartilage Best sequence: T2-weighted coronal and axial in supination Findings: LUCL discontinuity or attenuation, posterolateral capsule injury, radial head chondral damage
MRI is most useful when performed with the forearm in supination and elbow in slight flexion. The LUCL is best seen on coronal images just distal to the lateral epicondyle. A "bright" or discontinuous LUCL on T2 is diagnostic, but a normal MRI does not exclude symptomatic PLRI if clinical tests are positive.

Management Algorithm
Acute or Minimally Symptomatic PLRI
Goal: Allow soft-tissue healing and assess whether instability resolves with protected motion
Treatment Protocol
Immobilisation: Posterior splint or hinged brace at 90 degrees flexion, neutral rotation Avoid: Forced supination or varus stress Early motion: Gentle flexion-extension in pronation only
Hinged brace: Allow gradual extension, maintain pronation during loading Strengthening: Isometric exercises, avoid supinated resistance Reassess: Pivot-shift test at 6 weeks
Progressive loading: Begin supinated activities if stable Physiotherapy: Proprioception, dynamic stabiliser strengthening Return to sport: 3-4 months if asymptomatic and stable
Non-operative treatment succeeds in approximately 30-40 percent of acute post-dislocation PLRI when the injury is limited to stage 1-2 and the patient avoids supinated loading during healing. Failure is common when the Horii circle extends beyond stage 2 or when early aggressive supination exercises are prescribed.
Complications
Complications arise from untreated/recurrent instability and from reconstruction itself.
- Recurrent posterolateral rotatory subluxation/dislocation with mechanical symptoms (clicking, clunking, apprehension on push-up or pushing up from a chair)
- Progression to frank recurrent elbow dislocation when the lateral ulnar collateral ligament (LUCL) is incompetent
- Post-traumatic osteoarthritis from repeated radiocapitellar/ulnohumeral subluxation
- Chronic pain and loss of function; a missed diagnosis after a 'simple' elbow dislocation is the classic cause
- Residual or recurrent instability from non-anatomic (non-isometric) graft placement on the lateral epicondyle / capitellar centre
- Stiffness / flexion contracture - the commonest functional complication after elbow ligament surgery
- Posterior interosseous nerve (PIN) injury during the Kocher (anconeus-ECU) approach or distal ulnar tunnel drilling
- Tunnel malposition, graft elongation/failure, inter-tunnel fracture and heterotopic ossification
- Wound problems / infection (standard surgical risks)
The commonest 'complication' of PLRI is the missed diagnosis: a patient labelled with a 'simple elbow dislocation' or 'tennis elbow' who actually has LUCL insufficiency. Persistent lateral elbow pain, clicking or apprehension after an elbow dislocation should prompt a lateral pivot-shift assessment (often under anaesthesia) rather than reassurance.
The Medial Counterpart: Varus Posteromedial Rotatory Instability
PLRI is the posterolateral pattern; its frequently-missed mirror image is varus posteromedial rotatory instability (PMRI), driven by a fracture of the anteromedial facet of the coronoid (often with a lateral collateral ligament injury).
- Mechanism: a varus, posteromedial rotatory force shears off the anteromedial coronoid facet, which is normally unsupported by the underlying metaphysis and acts as a key anterior-medial buttress.
- The trap: these fractures look small on a plain AP film and the elbow can appear reduced, so they are easily dismissed - yet untreated they cause rapid varus collapse and early arthritis.
- Classification: the O'Driscoll classification of coronoid fractures distinguishes tip, anteromedial facet (subtypes 1-3) and basal fractures; the anteromedial facet type is the one that produces PMRI.
- Management: a displaced anteromedial facet fracture needs buttress plate fixation through a medial (over-the-top) approach plus repair of the lateral collateral ligament - not the radial-head-focused approach used for the terrible triad.
Q: An elbow looks reduced after a varus injury but CT shows a small anteromedial coronoid facet fracture. Why does it matter? A: It is the hallmark of varus posteromedial rotatory instability. The anteromedial facet is an unbuttressed corner of the coronoid, so even a small fragment leads to varus subluxation, rapid cartilage wear and arthritis if left unfixed. It needs buttress plating via a medial approach with lateral collateral ligament repair, not simple observation.
Guidelines, Registries & Global Practice
- PLRI occurs worldwide after simple elbow dislocation (incidence 5-10 percent of dislocations develop chronic instability)
- Overhead athletes and gymnasts have higher rates due to repetitive varus stress
- Iatrogenic PLRI remains a recognised complication of lateral epicondylitis release in all regions
- Missed diagnosis is the most common reason for late presentation globally
- High-resource: MRI + arthroscopic assessment, anatomic graft reconstruction with anchors
- Limited-resource: Clinical diagnosis with stress fluoroscopy, palmaris graft through bone tunnels
- Universal principle: Outcome depends on isometric tunnel placement and postoperative compliance more than implant cost
- Surgery: Concentrated in upper-limb specialist centres; generalists refer chronic cases
- Diagnosis emphasis
- Pivot-shift under anesthesia, MRI in supination
- Non-operative care
- Protected motion 6-12 weeks, reassess stability
- Surgery / reconstruction
- Anatomic LUCL reconstruction with autograft
- Diagnosis emphasis
- Clinical tests + stress views, MRI for planning
- Non-operative care
- Hinged bracing, avoid supinated loading
- Surgery / reconstruction
- Graft reconstruction when symptoms persist greater than 6 months
- Diagnosis emphasis
- Recognise Horii circle pattern on MRI
- Non-operative care
- Early protected pronated motion
- Surgery / reconstruction
- Isometric graft placement critical; document technique
- Diagnosis emphasis
- Apprehension and chair push-up as screening
- Non-operative care
- Physiotherapy-led, 3-month trial minimum
- Surgery / reconstruction
- Triceps or gracilis graft when palmaris absent
There is no dedicated elbow instability registry comparable to joint arthroplasty registries. Evidence is derived from prospective cohorts and anatomic studies rather than randomised trials. The consistent message across all guidelines is: diagnose with pivot-shift testing, allow 3-6 months for potential healing, then reconstruct isometrically with autograft when symptoms persist. Documentation of the Horii stage and tunnel positions improves audit and outcome analysis.
Record in every post-dislocation elbow:
- Pivot-shift test result (positive/negative, under anesthesia if required)
- Chair push-up and apprehension signs
- MRI findings of LUCL and cartilage status
- Time from injury and response to non-operative care A missed PLRI diagnosis leading to chronic instability and secondary arthritis is an avoidable source of morbidity worldwide. Always perform and document lateral stability testing after elbow dislocation reduction.
Controversies & Areas of Uncertainty
Most surgeons wait 3-6 months after dislocation before offering reconstruction. Earlier surgery risks operating on injuries that would have healed. Later surgery risks secondary cartilage damage. No high-quality data defines the exact threshold.
Palmaris longus, gracilis, and triceps all report good outcomes. Suture anchors versus interference screws versus bone tunnels have no comparative trials. Surgeon experience and graft availability drive choice rather than evidence.
Arthroscopy can confirm chondral damage and perform capsular plication, but ligament reconstruction remains an open procedure. Whether arthroscopic plication adds value in early-stage PLRI is debated.
Most protocols allow return at 6-9 months, but objective criteria (isokinetic strength, pivot-shift elimination, patient-reported stability) vary widely between centres. No consensus exists on the safest timeline.
MCQ Practice Points
Q: What is the primary restraint to posterolateral rotatory instability of the elbow? A: The lateral ulnar collateral ligament (LUCL). It originates from the lateral epicondyle and inserts on the supinator crest of the ulna. Sectioning studies confirm it is the essential lesion; all other lateral structures are secondary.
Q: Describe the pivot-shift test for PLRI and what constitutes a positive result. A: Patient supine, shoulder flexed 90 degrees, forearm fully supinated. Apply valgus and axial load while flexing the elbow from extension. Positive test: radial head subluxes posterolaterally at 40-60 degrees flexion with a palpable clunk, then reduces with further flexion. The test is pathognomonic for LUCL insufficiency.
Q: What is the Horii circle and why is it clinically relevant to PLRI? A: The Horii circle describes the sequential soft-tissue disruption from lateral to medial during elbow dislocation. Stage 1 = LUCL, Stage 2 = + posterolateral capsule, Stage 3 = + radial collateral, Stage 4 = + anterior/posterior capsule, Stage 5 = + MCL (complete dislocation). PLRI represents an incomplete stage; recognising the stage guides reconstruction magnitude.
Q: What are the indications and graft options for LUCL reconstruction? A: Indications: symptomatic PLRI greater than 3-6 months, positive pivot-shift, failed non-operative care. Graft options: palmaris longus (preferred), gracilis, or ipsilateral triceps tendon strip. The graft is passed through isometric humeral and ulnar bone tunnels and tensioned at 30-40 degrees flexion.
Q: Which clinical test has the highest sensitivity for symptomatic PLRI in the office setting? A: The chair push-up test (greater than 90 percent sensitivity). The patient pushes up from a chair with forearms supinated; reproduction of posterolateral pain or instability is positive. The lateral pivot apprehension sign is equally useful and often easier to elicit.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old rugby player sustained a simple elbow dislocation 4 months ago that was reduced in the emergency department. He has since had recurrent mechanical clicking and a feeling of instability when pushing up from a chair or throwing. Examination demonstrates a positive pivot-shift test and lateral pivot apprehension sign. X-rays are normal. How would you manage this patient?”
“A 45-year-old manual labourer presents with 18-month history of posterolateral elbow pain and instability after a fall onto an outstretched hand. He has a positive pivot-shift under anesthesia and MRI shows LUCL tear, radial head chondral loss, and early capitellar wear. He cannot return to heavy work. How would you manage?”
Key Anatomy
- LUCL originates lateral epicondyle, inserts supinator crest of ulna
- Primary restraint to posterolateral rotation and varus
- Secondary restraints: radial collateral ligament, posterolateral capsule
- Radial head is important secondary stabilizer when LUCL deficient
Diagnosis
- Pivot-shift test: gold standard (subluxation at 40-60 degrees flexion)
- Lateral pivot apprehension and chair push-up tests highly sensitive
- MRI in supination best visualises LUCL discontinuity
- Always test stability after simple elbow dislocation
Horii Circle Stages
- Stage 1: LUCL tear only - pivot-shift positive
- Stage 2: + posterolateral capsule - increased external rotation
- Stage 3: + radial collateral - gross subluxation
- Stage 4-5: complete dislocation with MCL involvement
Treatment Algorithm
- Acute post-dislocation: protected motion 3-6 months, reassess
- Symptomatic greater than 3-6 months: LUCL reconstruction
- Graft options: palmaris longus, gracilis, triceps tendon
- Tension graft at 30-40 degrees flexion, forearm pronated
Complications
- Recurrent instability: 5-15 percent if non-isometric tunnels
- Stiffness: 10-20 percent, worse with prolonged immobilisation
- Radial nerve or PIN injury: rare but reported with Kocher approach
- Secondary OA: common if chronic subluxation untreated
Evidence Base
The pivot-shift test for posterolateral rotatory instability of the elbow
- Original description of recurrent PLRI in five patients (aged 5 to 40), a condition the authors regarded as previously undescribed and difficult to diagnose
- Defined the posterolateral rotatory-instability test (supination, valgus moment and axial compression with the elbow flexed from extension), producing a sudden visible/palpable reduction of the radiohumeral joint beyond about 40 degrees of flexion
- Attributed the instability to laxity of the ulnar part of the lateral collateral ligament with an intact annular ligament; operative repair eliminated the instability in all five
Lateral ulnar collateral ligament reconstruction for posterolateral rotatory instability
- Eleven consecutive patients with PLRI managed operatively: radial collateral-ligament complex advanced/imbricated in 3, lateral ulnar collateral ligament reconstructed with palmaris longus in 7 (2 augmented with a prosthetic ligament) and with triceps fascia in 1
- Stability achieved in 10 of 11 patients, with an excellent functional result in 7
- The single failure occurred in a palmaris-longus reconstruction augmented with a prosthetic ligament
Ligamentous repair and reconstruction for posterolateral rotatory instability of the elbow
- Intermediate results of 12 direct repairs and 33 tendon-autograft reconstructions (44 of 45 elbows followed at a mean of 6 years, range 2 to 15)
- Surgery restored stability in all but five patients (two stabilised after a second procedure); mean Mayo Elbow Performance Score 85, with 19 excellent, 13 good, 7 fair and 5 poor and 86 percent subjectively satisfied
- Better outcomes with a post-traumatic aetiology, subjective instability at presentation and augmented tendon-graft reconstruction; reconstruction outperformed repair and did not deteriorate with time
Tardy posterolateral rotatory instability of the elbow due to cubitus varus
- Twenty-four patients (25 limbs) with cubitus varus (mean 15 degrees) developed tardy PLRI roughly two to three decades after a childhood distal-humeral fracture or congenital deformity, presenting with lateral elbow pain and recurrent instability
- Medial displacement of the mechanical axis, olecranon and triceps line of pull imposes a repetitive external-rotation torque on the ulna that stretches the lateral collateral ligament complex
- Good or excellent results in 19 of 22 operated limbs (combinations of LCL reconstruction and corrective osteotomy), establishing cubitus varus as a cause rather than a purely cosmetic deformity