Paronychia (Acute & Chronic)
- Antibiotics for an established abscess. "No pus, no knife — but once there is pus, drain it." Antibiotics are an adjunct, never a substitute for drainage.
- Incising a herpetic whitlow. Grouped vesicles + recurrent + pain-out-of-proportion = HSV — do NOT incise (risks superinfection/spread; it is self-limiting, give aciclovir).
- Cutting the eponychium / germinal matrix. Over-zealous incision near the proximal fold causes permanent nail deformity — lift the fold/incise parallel to the nail and spare the matrix.
- Treating chronic paronychia as an abscess. Chronic (over 6 weeks, multiple wet-hand digits) is an inflammatory dermatitis, not pus — repeated incision is wrong; treat the barrier (dry, gloves, emollient, topical steroid).
- Missing the tumour. A chronic, atypical, non-resolving single-digit "paronychia" can be SCC or amelanotic melanoma — biopsy it.
- Missing run-around/subungual pus. Pus tracked under the nail base or to the opposite fold will recur unless the eponychial fold is elevated ± the nail is (partly) removed.
Overview & epidemiology
Paronychia is the most common hand infection. It is two distinct entities: acute bacterial paronychia (rapid, usually a single digit, after a breach of the cuticle seal — hangnail, nail-biting, manicure, ingrowing nail) and chronic paronychia (over 6 weeks, typically several digits of a "wet hand"). Acute disease most often affects otherwise healthy people with a recent nail-fold breach; chronic disease clusters in "wet-hand" occupations (cleaners, bartenders, dishwashers, food handlers, swimmers) and is more common in diabetes, immunosuppression and with systemic retinoid use. The peak for chronic paronychia is middle-aged women in wet work. Recognising which entity you are facing — and the felon and herpetic-whitlow look-alikes — drives the entire management.
Acute paronychia — infection of the nail fold; pus collects superficial to the nail plate, under the eponychium or lateral fold → drain it (antibiotics alone fail once pus is present). Felon — closed-space abscess of the pulp (volar fingertip) with its fibrous septa; tense, throbbing, globally swollen pad → different incision (volar/high-lateral) to avoid skin necrosis and osteomyelitis. Herpetic whitlow — viral (HSV): grouped vesicles on an erythematous base, intense pain, recurrent → do NOT incise (self-limiting; aciclovir; incision risks superinfection/spread).
The felon is the closed-space abscess of the volar fingertip pulp the topic keeps telling you to separate from paronychia — different space, different incision:
- Anatomy: the pulp is divided by ~15 to 20 fibrous septa running from the periosteum of the distal phalanx to the skin, creating tight fat-filled compartments; infection (usually S. aureus, often after a splinter/penetrating injury) raises pressure within these closed spaces.
- Presentation: a rapidly worsening, throbbing, tense, exquisitely tender, globally swollen distal pulp (distal to the DIP crease) — the rest of the finger is spared (contrast paronychia, confined to the nail fold).
- Complications of the closed-space pressure: skin/pulp necrosis, distal phalanx osteomyelitis, septic DIP arthritis, spread to the flexor sheath, and tip ischaemia.
- Drainage: a high lateral (mid-axial) incision over the point of maximal tenderness (the non-contact border — ulnar in the fingers, radial in thumb/index), or a longitudinal volar incision, breaking the septa to decompress; avoid crossing the DIP flexion crease (contracture) and avoid the "fish-mouth"/through-and-through incision (causes an unstable, anaesthetic, painful pad and tip necrosis). Antibiotics are adjunctive; X-ray if osteomyelitis is suspected.
Pathophysiology & anatomy
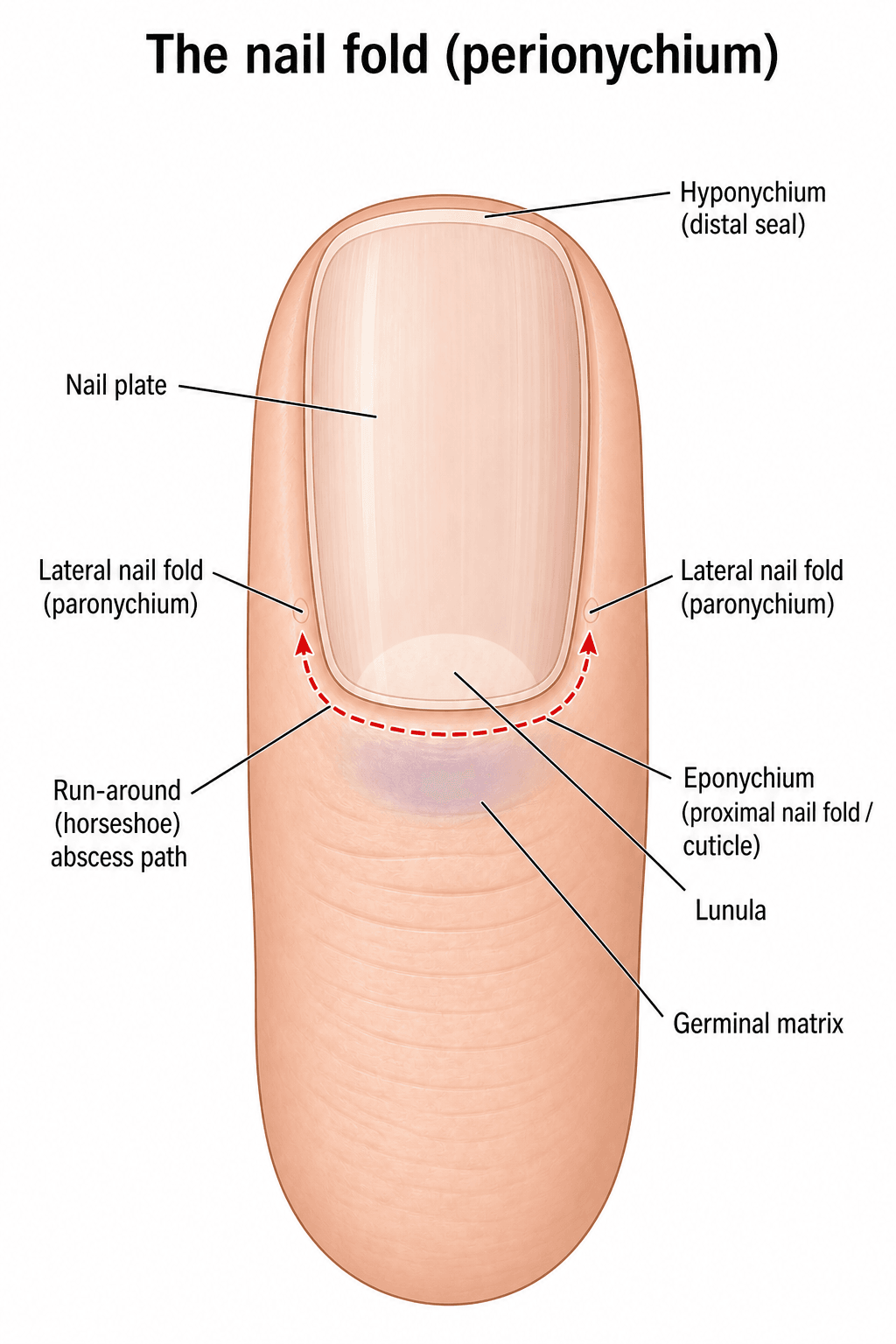
The perionychium is the soft tissue surrounding the nail: the eponychium (proximal nail fold, the cuticle), the paronychium (lateral nail folds) and the hyponychium (the seal under the distal free edge). The eponychial fold continues as a thin layer over the germinal matrix — this continuity is why pus in one lateral fold can spread proximally under the eponychium and across to the other fold (the "run-around" abscess). The seal between cuticle and nail plate is the principal barrier; once it is breached (hangnail, nail-biting, aggressive manicure, splinter, ingrowing nail), bacteria enter the potential space of the nail fold.
A breach of the cuticle seal allows skin flora into the nail fold. Staphylococcus aureus is the most common organism; MRSA is increasingly frequent and should be assumed in non-responders and high-prevalence settings. Mixed flora (streptococci, and in nail-biters/oral contact anaerobes and Eikenella corrodens) also occur. Infection begins as a cellulitis of the fold and, if untreated, localises into an abscess that points at the fold margin or under the eponychium. Untreated pus can track under the nail (subungual abscess) or around the base (run-around / horseshoe abscess), and rarely into the pulp or to the distal phalanx.

Clinical presentation
- Rapid onset (hours to days), usually one digit
- Throbbing pain, erythema, swelling of a single nail fold
- A visible collection of pus at the fold margin or under the cuticle
- Often a precipitant: hangnail, nail-biting, manicure, minor trauma, ingrowing nail
- Fluctuance and a "shiny", tense fold indicate a drainable abscess
- Insidious, more than 6 weeks, often several digits (dominant hand)
- Loss of the cuticle, boggy/retracted nail fold, intermittent discharge
- Nail dystrophy — transverse ridging, discolouration, surface irregularity
- Episodic acute flares superimposed on chronic change
- "Wet-hand" occupation, diabetes, immunosuppression, or systemic retinoid use
Assess how much pus and where (lateral fold, eponychium, subungual, run-around), and whether infection has spread to the pulp (felon) or there is lymphangitis/systemic upset. Always look for vesicles (herpetic whitlow) before reaching for a blade. In a chronic, non-healing, or atypical single-digit "paronychia" that resists treatment, think of the mimics: squamous cell carcinoma, amelanotic melanoma, pyogenic granuloma, chronic osteomyelitis, gout/tophi, sarcoid, and unusual organisms (mycobacteria, Candida in the immunosuppressed). Biopsy a chronic lesion that does not settle.

Investigations
Paronychia is a clinical diagnosis. Investigations are selective:
- Swab pus for Gram stain and culture/sensitivity at drainage — guides antibiotics and detects MRSA.
- Imaging is not routine; consider a radiograph if there is a suspected foreign body, retained splinter, or chronicity/possible osteomyelitis of the distal phalanx.
- Bloods only if systemically unwell or in the immunocompromised/diabetic.
Management
No pus, no knife — but once there is pus, drain it. Early acute paronychia (cellulitis only) may settle with warm soaks and oral antibiotics. An established abscess requires drainage; antibiotics are an adjunct, not a substitute. Chronic paronychia is treated as a dermatitis — moisture avoidance and topical anti-inflammatories — not by repeated incisions.
Warm soaks, elevation, and a short course of an anti-staphylococcal oral antibiotic (e.g. flucloxacillin; cover MRSA — e.g. co-trimoxazole/doxycycline/clindamycin per local sensitivities — where prevalent or in non-responders). Many early cases resolve without surgery.
Drainage. Under digital (ring) block: lift the affected nail fold off the nail plate with a blunt instrument/scalpel held parallel to the nail to release pus; a small incision may be needed at the point of maximal fluctuance. Avoid cutting into or scarring the eponychium/germinal matrix. Send pus for culture; leave open or lightly pack; dressing and soaks afterwards.
If pus is under the nail base or has run around to the opposite fold, elevate the eponychial fold and perform partial (proximal) or complete nail-plate removal to deroof and drain the collection. Inadequate drainage is the usual reason for recurrence.
Reserve/continue oral antibiotics for surrounding cellulitis, lymphangitis, systemic features, or the immunocompromised/diabetic; tailor to culture. Antibiotics do not replace adequate drainage.

Match the technique to where the pus sits (all under a digital/ring block, all sparing the germinal matrix):
- Simple elevation: pus at a lateral fold → slide a blunt elevator (Freer) or a blade held parallel to the nail under the affected fold to release pus, or a small incision at maximal fluctuance directed away from the eponychium.
- Eponychial flap (single or double incision): pus under the eponychium / proximal fold → one or two short longitudinal incisions at the corner(s) of the eponychial fold, reflecting it proximally to expose and drain the proximal nail — never incise transversely across the matrix.
- Partial (proximal-third) nail removal for subungual pus localised proximally; complete nail removal for extensive subungual pus — to deroof the collection.
- "Swiss roll" technique for a severe run-around (horseshoe) abscess → incise both eponychial corners, reflect and roll the fold back over a suture/dressing, leaving it open to drain and unrolling it later — drains the whole horseshoe while preserving the nail and matrix. The cardinal error throughout is damaging the germinal matrix (deep or transverse cuts) → permanent nail dystrophy.
Complications
- Run-around (horseshoe) abscess from inadequate or late drainage
- Spread to the pulp (felon), flexor sheath, or distal phalanx (osteomyelitis)
- Nail dystrophy and permanent matrix damage in chronic disease
- Recurrence (often from persistent moisture exposure or missed subungual pus)
- Germinal matrix injury from an overzealous incision near the eponychium → permanent nail deformity
- Inadequate drainage → persistence/recurrence
- Missed mimic (SCC, melanoma) treated repeatedly as "infection" — the dangerous error
- Antibiotic overuse without drainage
Mnemonics & memory aids
PUSAcute paronychia
Hook:Acute paronychia in three letters: find the PUS, free the PUS, and Swab the PUS.
WETChronic paronychia
Hook:Chronic paronychia lives on WET hands — dry them, calm the inflammation, and don't miss a tumour.
Fold • Pulp • VesiclesThe painful fingertip — 3 look-alikes
Hook:Fold, Pulp, Vesicles — where the problem sits tells you whether (and how) to cut: fold = drain, pulp = felon incision, vesicles = leave alone.
Evidence Base
Fingertip Infections
- The fingertip is the most common site of hand infection; mismanagement carries serious consequences.
- Reviews the perionychial and pulp anatomy and the pathophysiology and treatment of acute and chronic paronychia and felon — including surgical-versus-medical decision-making, antibiotic choice, incision technique and aftercare.
- Emphasises recognising the infectious, rheumatologic and oncologic conditions that mimic common fingertip infections.
Bacterial and viral infections of the nail unit: Tips for diagnosis and management
- The nail unit is the most commonly affected area in hand infections, usually triggered by mechanical or chemical trauma (artificial nails/polish can harbour organisms).
- Abscesses should always be drained, but herpetic whitlow may mimic an abscess and instead requires NON-operative treatment to prevent sequelae.
- A more conservative approach is advised for less severe bacterial infection and for subacute/chronic nail infection.
Topical steroids versus systemic antifungals in the treatment of chronic paronychia: an open, randomized double-blind and double dummy study
- RCT in 45 adults with chronic paronychia comparing a topical corticosteroid (methylprednisolone aceponate) with systemic antifungals (itraconazole or terbinafine).
- The topical steroid was MORE effective: 41/48 nails improved or cured versus 30/57 (terbinafine) and 29/64 (itraconazole).
- Candida presence was not linked to disease activity and its eradication rarely produced cure - supporting chronic paronychia as a hand dermatitis, not an onychomycosis.
Acute and Chronic Paronychia
- Acute paronychia follows a breach of the nail barrier; treat with warm soaks ± topical antibiotic/steroid, and DRAIN any abscess (oral antibiotics usually unnecessary if drainage is adequate, unless immunocompromised/severe).
- Chronic paronychia (symptoms over 6 weeks) is an irritant dermatitis from acids/alkalis/chemicals in wet-work occupations; treat by stopping the irritant and using topical steroids or calcineurin inhibitors.
- Patient education to restore and protect the nail barrier is central to preventing recurrence.
The anatomy-based management of fingertip infection and the importance of recognising mimics come from Barger et al. 2020 (DOI); the drain-the-abscess-but-not-the-whitlow principle and conservative approach to chronic disease from Iorizzo & Pasch 2022 (DOI); the randomised evidence that a topical steroid outperforms systemic antifungals in chronic paronychia from Tosti et al. 2002 (DOI); and the acute-vs-chronic management synthesis from Leggit 2017 (Am Fam Physician 2017;96(1):44-51, PMID 28671378). The S. aureus/MRSA microbiology, the run-around/felon anatomy, and the chronic-paronychia-as-dermatitis model are standard hand-infection teaching.