Neuralgic Amyotrophy | Severe Pain THEN Patchy Palsy | The Great Mimic
- Pain BEFORE palsy: severe neuropathic shoulder/arm pain for days to weeks, then weakness emerges as pain settles
- Patchy, multifocal: affects individual nerves or fascicles (long thoracic, suprascapular, AIN, PIN), not a single root or trunk
- Immune-mediated: often triggered by infection, vaccination, surgery, or strenuous exercise
- Hourglass fascicular constrictions: the structural lesion sits WITHIN the parent nerve, proximal to the branch point
- Recovery is slow and often incomplete: two-thirds have residual pain or weakness at 3 years
- “Disproportionate early pain that wakes the patient is the giveaway
- “Scapular winging plus a dropped shoulder = long thoracic plus suprascapular involvement
- “It is the classic cause of 'spontaneous' AIN or PIN palsy
- “No randomised evidence for any drug - steroids are used early on weak evidence
Severe pain precedes weakness. A spontaneous upper-limb palsy with a preceding bout of disproportionate neuropathic pain is neuralgic amyotrophy until proven otherwise.
Weakness does not respect a single nerve or root. A patchy pattern (for example winging PLUS deltoid weakness) points away from a compressive lesion and towards neuralgic amyotrophy.
It imitates rotator cuff tear, cervical radiculopathy, and isolated AIN/PIN palsy. Always ask about the painful onset to avoid an unnecessary cuff repair or discectomy.
Do not promise full recovery. Around two-thirds have lasting pain, weakness, or fatigability at three years; counsel realistically.
Overview and Epidemiology
Neuralgic amyotrophy is the great mimic of the upper limb. Recognising the painful-onset, patchy palsy prevents misdiagnosis as a rotator cuff tear, cervical radiculopathy, or a simple compressive nerve entrapment - and prevents unnecessary surgery.
Parsonage-Turner syndrome (neuralgic amyotrophy, idiopathic brachial plexus neuritis) is an immune-mediated disorder of the brachial plexus and its branches. It is defined by attacks of severe neuropathic upper-limb pain followed by patchy, multifocal weakness and atrophy.
- Incidence: about 1 per 1,000 per year in primary care - far commoner than older textbooks state
- Age: idiopathic form peaks around 40 years; hereditary form earlier (late 20s)
- Sex: slight male predominance in idiopathic disease
- Recurrence: roughly a quarter of idiopathic patients have further attacks over years
Long under-recognised; awareness is the main barrier to diagnosis.
- Frequently misdiagnosed: mistaken for cuff pathology or radiculopathy
- Classic cause of spontaneous AIN and PIN palsy
- Slow recovery: months to years, often incomplete
- Functional burden: residual pain, weakness, and fatigability are common
Early recognition allows pain control, rehabilitation, and realistic counselling.
According to PubMed, a prospective primary-care cohort found a one-year incidence of classic neuralgic amyotrophy of 1 per 1,000, suggesting the disorder is 30-50 times more common than previously thought (DOI).
Pathophysiology and Mechanisms
In neuralgic amyotrophy the structural lesion is an intraneural hourglass-like fascicular constriction located WITHIN the parent nerve, proximal to the branch point - not external compression at the usual entrapment sites. This is why a "spontaneous AIN palsy" is really a proximal median-nerve fascicular problem.
- Predisposition: a susceptible peripheral nervous system (clear in hereditary disease with SEPT9 mutations)
- Trigger: an immune-activating event - infection, vaccination, surgery, the peripartum period, or strenuous exercise
- Immune attack: focal inflammatory injury to specific nerves or fascicles within the brachial plexus
- Fascicular constriction: swelling, then incomplete and complete hourglass constriction, and finally fascicular entwinement - a continuum seen on high-resolution ultrasound
- Inflammatory cell infiltration
- Demyelination
- Reduction in the number of nerve fibres
- Predilection for the upper and middle trunk - the long thoracic and suprascapular nerves are most often hit
- Distal mononeuropathies (AIN, PIN, superficial radial) occur, but the lesion still sits proximally in the parent nerve
- Phrenic nerve involvement can cause diaphragmatic palsy and breathlessness
Classification Systems
Idiopathic versus Hereditary Neuralgic Amyotrophy
- Idiopathic (INA)
- Around 40 years
- Hereditary (HNA)
- Younger, late 20s
- Idiopathic (INA)
- Usually single or few
- Hereditary (HNA)
- Recurrent, more frequent
- Idiopathic (INA)
- Sporadic
- Hereditary (HNA)
- SEPT9 mutation, autosomal dominant
- Idiopathic (INA)
- Less common (~17%)
- Hereditary (HNA)
- More common (~56%)
- Idiopathic (INA)
- Better on average
- Hereditary (HNA)
- Poorer, more severe paresis
The hereditary form is roughly ten times less common than the idiopathic form.
Clinical Assessment
- Pain: sudden, severe, neuropathic shoulder/arm pain, often waking the patient
- Sequence: pain for days to weeks, THEN weakness as pain eases
- Triggers: ask about recent infection, vaccine, surgery, pregnancy, exertion
- Sensory symptoms: present in most (around three-quarters) but milder than the pain
- Family history: recurrent attacks suggest hereditary form
The painful prodrome is the single most useful historical clue.
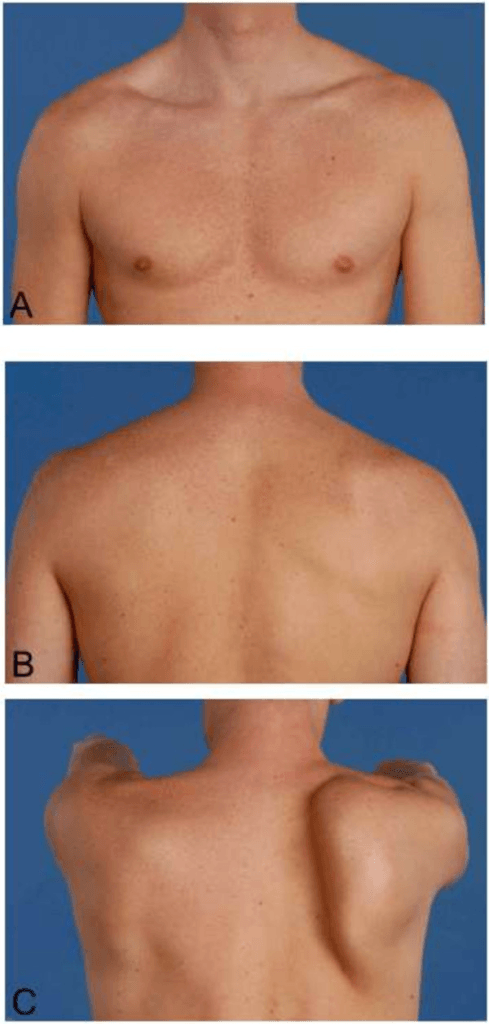
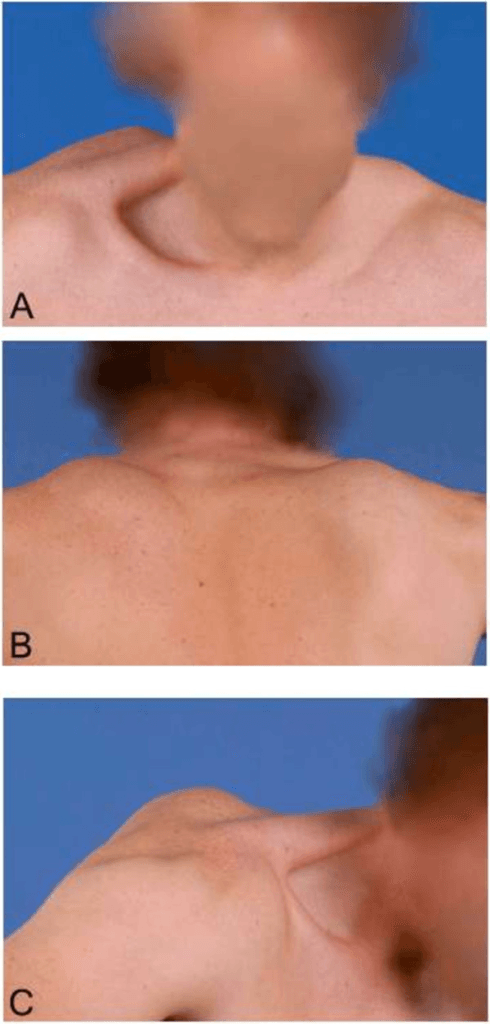
- Inspection: scapular winging, periscapular and deltoid wasting
- Targeted motor testing: serratus anterior, supraspinatus/infraspinatus, FPL/FDP (AIN), finger extensors (PIN)
- Patchy weakness: not confined to one nerve or root
- Sensory exam: variable, often patchy sensory loss
- Reflexes: usually preserved unless a major nerve is affected
Examine the whole upper limb - the deficit is rarely where the pain is worst.
- Shared feature
- Shoulder/arm pain plus weakness
- Key difference
- Radiculopathy follows a dermatome/myotome; pain is neck-related and worse with neck movement
- Shared feature
- Painful weak shoulder
- Key difference
- Cuff tear has no patchy distal palsy and no severe neuropathic prodrome
- Shared feature
- Isolated distal motor palsy
- Key difference
- Neuralgic amyotrophy has a painful onset and proximal fascicular lesion
- Shared feature
- Sudden severe shoulder pain
- Key difference
- No motor palsy; calcium on radiograph
Bilateral or rapidly ascending weakness, prominent sensory level, or bowel/bladder change should prompt consideration of Guillain-Barre syndrome, myelopathy, or a structural plexus lesion (tumour). Patchy painful upper-limb palsy with normal cord signs favours neuralgic amyotrophy.
The Three Phases of Pain in Neuralgic Amyotrophy
The evidence base notes that the pain "runs in three consecutive phases" — worth developing, because the character of the pain changes over time and mis-reading it drives the wrong treatment.
- Phase 1 — initial severe neuropathic pain. A sudden, intense, continuous neuropathic pain (often waking the patient), typically lasting around four weeks. It is out of proportion to any mechanical finding and is the diagnostic prodrome; weakness emerges as it settles.
- Phase 2 — musculoskeletal / mechanical pain. As the acute pain fades and weakness (especially periscapular) develops, a second, more musculoskeletal pain appears from altered scapular biomechanics, muscle imbalance and overuse of compensating muscles. This pain responds to scapular rehabilitation rather than to neuropathic drugs.
- Phase 3 — chronic intermittent pain. A longer-term pattern of intermittent neuropathic and exertional pain with fatigability, part of the residual burden affecting the majority at three years.
- Why it matters. The phase directs treatment: neuropathic analgesia (and possible early steroids) for phase 1; scapular/postural rehabilitation and pacing for phases 2-3. Persistent phase-1-type neuropathic pain alongside a structural constriction on imaging is what raises the question of surgery.
Q: How does the pain of neuralgic amyotrophy evolve, and how does that change management? A: Three phases — an initial severe neuropathic prodrome (~4 weeks), then a musculoskeletal pain from altered scapular mechanics as weakness sets in, then chronic intermittent/exertional pain. Treat phase 1 with neuropathic analgesia (and possibly early steroids), and phases 2-3 with scapular rehabilitation and pacing — giving neuropathic drugs for the mechanical pain, or physio for the acute neuropathic pain, misfires.
Investigations
Investigation Protocol
History plus examination carry the diagnosis: a painful onset followed by patchy upper-limb weakness with a typical nerve distribution. Investigations support and localise rather than confirm.
EMG/NCS after about 2-3 weeks shows patchy denervation in the affected muscles with relatively preserved sensory studies in pure-motor branches. Helps map the multifocal pattern and excludes radiculopathy.
HRUS of the clinically affected nerves can show nerve swelling, incomplete or complete constriction, and fascicular entwinement - a continuum that helps predict recovery versus need for surgery.
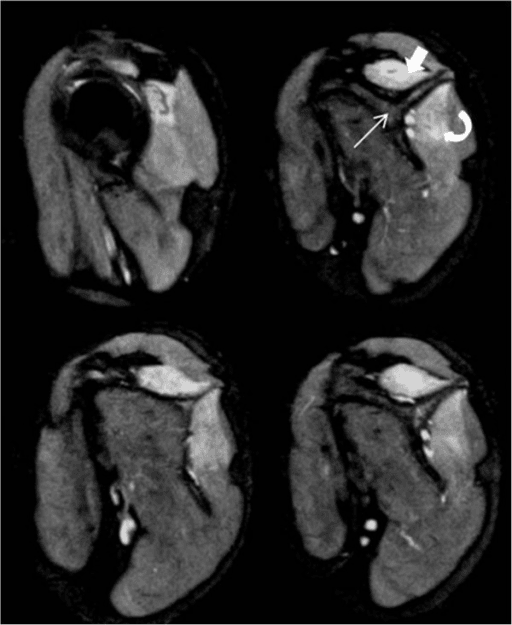
MRI shows muscle denervation oedema (bright T2 signal) and MR neurography can localise the fascicular lesion. Useful when the affected nerve is hard to pin down or to exclude a structural plexus lesion.
Bloods and triggers:
- No specific blood test confirms the diagnosis
- Consider testing for an antecedent trigger where relevant - hepatitis E serology is worthwhile, as acute hepatitis E virus infection has a recognised association with neuralgic amyotrophy
According to PubMed, a Swiss multicentre case-control study found a moderate association between concomitant acute hepatitis E virus infection and neuralgic amyotrophy, but not with Guillain-Barre syndrome or Bell's palsy (DOI).
Management Algorithm
Acute Phase (Pain Dominant)
Acute Management
Aggressive multimodal analgesia. Neuropathic agents (for example gabapentinoids, amitriptyline) plus simple analgesia; opioids may be needed short term. The early pain is severe and a major source of distress.
Oral corticosteroids in the first month may shorten the painful phase and accelerate recovery in some patients, based on weak (non-randomised) evidence. Discuss the uncertainty and risks before starting.
Avoid overuse of the painful limb, protect from traction injury, and explain the natural history. Reassurance about the typical sequence (pain settles, then weakness emerges) reduces anxiety.
There is no proven disease-modifying drug; treatment is largely supportive.
Complications and Sequelae
- Frequency
- Common (up to two-thirds at 3 years)
- Management
- Rehabilitation, tendon transfer if fixed
- Frequency
- Common
- Management
- Neuropathic analgesia, pacing
- Frequency
- Frequent
- Management
- Energy conservation, graded activity
- Frequency
- Frequent with long thoracic involvement
- Management
- Scapular rehab, transfer if persistent
- Frequency
- ~25% idiopathic, higher hereditary
- Management
- Counsel, treat each attack acutely
- Frequency
- Uncommon
- Management
- Monitor; plication in selected cases
According to PubMed, a study of the clinical spectrum in 246 patients found that overall recovery is less favourable than usually assumed, with persisting pain and paresis in approximately two-thirds of patients followed for three years or more (DOI).
Extra-Plexal Involvement: Phrenic Nerve and Diaphragmatic Palsy
The pathophysiology and complications flag phrenic nerve involvement as an extra-plexal feature — here is how it presents and is managed, because it is easily missed as "just deconditioning".
- Why it happens. Neuralgic amyotrophy is patchy and can strike nerves outside the plexus; the phrenic nerve is the classic extra-plexal target (the recurrent laryngeal is another, causing hoarseness). Extra-plexal involvement is commoner in the hereditary form.
- Presentation. Dyspnoea, especially orthopnoea (breathlessness lying flat), reduced exercise tolerance and disturbed sleep — often overshadowed by the shoulder pain and weakness, so it is under-recognised.
- Diagnosis. A raised hemidiaphragm on chest radiograph; paradoxical diaphragm movement on the sniff test (fluoroscopy or ultrasound); and lung-function tests showing a fall in vital capacity from erect to supine (a supine drop of about 20% or more suggests diaphragm weakness).
- Management. Most recover spontaneously over months to a couple of years, in line with the general natural history; supportive measures (non-invasive ventilation for symptomatic or nocturnal hypoventilation) bridge severe cases, and diaphragmatic plication is reserved for persistent, symptomatic unilateral palsy that fails to recover.
Q: A patient with neuralgic amyotrophy becomes breathless lying flat — what is the concern and how do you confirm it? A: Phrenic-nerve involvement with diaphragmatic palsy — the classic extra-plexal target (commoner in hereditary NA). Confirm with a raised hemidiaphragm on CXR, a positive sniff test (paradoxical elevation), and a supine drop in vital capacity (about 20% or more). Most recover spontaneously; reserve plication for persistent symptomatic palsy.
Clinical Relevance for the Orthopaedic Surgeon
The orthopaedic trap is operating on the wrong problem: a "frozen shoulder" or "cuff tear" that is actually neuralgic amyotrophy, or a "compressive AIN/PIN palsy" decompressed at the forearm when the lesion is a proximal fascicular constriction. The painful prodrome and patchy pattern are what save the patient an unnecessary operation.
Neuralgic amyotrophy can occur after any surgery or anaesthetic, sometimes in a limb remote from the operation. New patchy painful weakness post-operatively is not always a positioning or block injury - keep neuralgic amyotrophy in the differential.
Most spontaneous AIN and PIN palsies are now understood as forms of neuralgic amyotrophy with proximal fascicular constrictions. This reframes both diagnosis (image proximally) and surgery (operate proximally if at all).
When serratus anterior winging follows a painful episode, neuralgic amyotrophy is the leading cause. Most recover; reserve nerve or tendon transfer for persistent, disabling winging after prolonged failure to recover.
Set expectations early: pain settles first, strength returns slowly over months to years, and recovery may be incomplete. Honest counselling protects both patient and surgeon.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Annual incidence around 1 per 1,000 in a prospective primary-care setting - far higher than older hospital-based estimates
- Long under-recognised; awareness is the main determinant of diagnosis rate worldwide
- Idiopathic form peaks around age 40; hereditary form (SEPT9) is roughly ten times less common with earlier, recurrent attacks
- Recognised triggers (infection including hepatitis E, vaccination, surgery, peripartum period, exertion) are identified in roughly half of cases
Side-by-Side Practice (no condition-specific registry exists for neuralgic amyotrophy):
- Diagnostic emphasis
- Clinical pain-then-palsy pattern
- Acute treatment
- Supportive; early oral steroids on weak evidence
- Imaging
- EMG to map multifocal denervation
- Diagnostic emphasis
- Recognise spontaneous AIN/PIN palsy as neuralgic amyotrophy
- Acute treatment
- Observe first; analgesia
- Imaging
- HRUS / MR neurography to localise constriction
- Diagnostic emphasis
- Functional and patchy deficit mapping
- Acute treatment
- Scapular and energy-conservation rehab
- Imaging
- Clinical and serial EMG follow-up
- Diagnostic emphasis
- Localise fascicular constriction
- Acute treatment
- As above
- Imaging
- HRUS continuum (swelling to entwinement) guides surgery
There is broad agreement that the diagnosis is clinical, that most cases are observed first with supportive care, and that imaging (HRUS / MR neurography) is increasingly used to localise a proximal fascicular constriction and select the minority who may benefit from surgery.
- Well-resourced settings: HRUS and MR neurography localise intraneural constrictions; interfascicular microneurolysis and nerve reconstruction available for non-recovering focal lesions
- Limited-resource settings: diagnosis is clinical (painful onset, patchy palsy, typical nerve distribution), often without electrodiagnostics or advanced imaging; management defaults to analgesia, rehabilitation, and observation, with tendon transfer as the principal salvage for established deficits
- Record the painful prodrome and the patchy, multifocal distribution that define the diagnosis
- Counsel on slow, often incomplete recovery and the possibility of recurrence
- For surgery on a fascicular constriction, consent should cover incomplete recovery and the need for possible nerve grafting or later tendon transfer
- Document trigger screening, including hepatitis E serology where liver enzymes are deranged
Memory Aids
PAINFULRecognising Neuralgic Amyotrophy
Hook:PAINFUL - the pain is the clue that turns a confusing patchy palsy into the diagnosis.
SPIVECommon Triggers
Hook:SPIVE - ask about all five triggers in the history; one is found in roughly half of cases.
SLAPMost Commonly Affected Nerves
Hook:SLAP - the four nerves to examine carefully in any suspected neuralgic amyotrophy.
MCQ Practice Points
Q: What is the characteristic temporal sequence of Parsonage-Turner syndrome? A: Severe neuropathic pain first, then patchy weakness as the pain subsides over days to weeks. This pain-before-palsy sequence is the key diagnostic clue.
Q: Which nerves are most commonly involved? A: The long thoracic and suprascapular nerves (upper/middle trunk distribution), involved in the majority of cases; distal branches such as the AIN and PIN are also classically affected.
Q: What is the structural lesion in spontaneous distal mononeuropathies due to neuralgic amyotrophy? A: An hourglass-like fascicular constriction within the parent nerve, proximal to the branch point - not external entrapment at the usual distal site.
Q: What is the level of evidence for corticosteroids in neuralgic amyotrophy? A: Weak. A Cochrane review found no randomised trials; one open-label series suggested early oral prednisone may shorten initial pain and speed recovery in some patients.
Q: What proportion of patients have residual deficit at three years? A: About two-thirds have persisting pain or weakness at three years or more - recovery is slower and less complete than older teaching suggested.
Q: Which viral infection has a recognised association with neuralgic amyotrophy? A: Acute hepatitis E virus infection, particularly when accompanied by raised liver enzymes at onset.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 38-year-old man develops sudden severe right shoulder pain that wakes him at night and lasts about two weeks. As the pain settles he notices his shoulder blade sticks out and he struggles to lift his arm overhead. He had a flu vaccine three weeks ago. What is your diagnosis and approach?”
“A 30-year-old woman presents with a weak OK sign and no sensory loss, preceded by a few days of forearm and arm pain. She has no history of trauma or mass. Imaging of the forearm is normal. How do you reconcile this with classic anterior interosseous syndrome, and what does it change?”
“A patient with confirmed neuralgic amyotrophy affecting the posterior interosseous nerve has had no clinical or electrical recovery at six months. High-resolution ultrasound shows a complete hourglass constriction of the affected fascicles. What are the options and how do you decide?”
Core Concept
- Immune-mediated neuralgic amyotrophy of the brachial plexus
- Pain FIRST, then patchy multifocal weakness and atrophy
- Lesion = hourglass fascicular constriction within the parent nerve
- Incidence about 1 per 1,000/year - common, not rare
Triggers
- Infection (including hepatitis E)
- Vaccination
- Surgery / anaesthesia
- Pregnancy/postpartum and strenuous exercise
Most Affected Nerves
- Long thoracic - scapular winging
- Suprascapular - weak external rotation
- Anterior interosseous - weak OK sign
- Posterior interosseous - finger drop
Diagnosis
- Clinical: painful onset plus patchy palsy
- EMG/NCS: multifocal denervation, maps pattern
- HRUS / MR neurography: localise constriction
- MRI: muscle denervation oedema (bright T2)
Management
- Aggressive neuropathic pain control
- Early oral corticosteroids (weak evidence)
- Scapular and energy-conservation rehabilitation
- Surgery only for non-recovering focal constriction
Prognosis
- Recovery slow: months to years
- Residual deficit in about two-thirds at 3 years
- Recurrence in ~25% idiopathic, higher hereditary
- Counsel realistically - do not promise full recovery
Evidence Base
- 246 patients (199 idiopathic, 47 hereditary); pain runs in three phases with an initial severe phase lasting about 4 weeks
- Sensory involvement in 78.4%; upper/middle trunk distribution (long thoracic and/or suprascapular) most common (71.1%)
- Hereditary form: earlier onset, more attacks, more extra-plexal nerves, worse outcome than idiopathic
- Persisting pain and paresis in about two-thirds of patients followed for 3+ years
- Prospective primary-care registration of new neck/shoulder/arm complaints in 14,118 people over one year
- 14 confirmed classic neuralgic amyotrophy cases, giving a one-year incidence of 1 per 1,000
- Suggests the disorder is 30-50 times more common than previously believed
- Under-recognition, not rarity, explains the historical low estimates