Great Toe | Lesser Toes | Usually Conservative
- Phalangeal fractures foot = most common foot fractures - great toe (hallux) most important, lesser toes usually conservative
- Great toe requires better alignment - Hallux is critical for push-off, displacement greater than 2mm or intra-articular step-off requires ORIF
- Lesser toes usually conservative - Buddy taping and early weight bearing usually sufficient, ORIF rarely needed
- Intra-articular fractures - Displacement greater than 2mm or step-off requires ORIF to prevent arthritis
- Usually conservative treatment - Most heal with buddy taping and protected weight bearing
- “Great toe most important - requires better alignment
- “Lesser toes usually conservative - buddy taping
- “Intra-articular displacement requires ORIF
- “Usually conservative treatment
Great toe (hallux) most important - Critical for push-off and gait. Displacement greater than 2mm or intra-articular step-off requires ORIF. Lesser toes usually conservative with buddy taping.
Most phalangeal fractures heal with conservative treatment - Buddy taping and protected weight bearing. ORIF rarely needed - only for great toe displacement, intra-articular step-off, or open fractures.
Intra-articular fractures require ORIF if displaced - Step-off greater than 2mm causes arthritis. Great toe IP joint most critical. Screw or K-wire fixation.
Lesser toes (2nd-5th) usually conservative - Buddy taping and early weight bearing usually sufficient. ORIF rarely needed - only for severe displacement or open fractures.
- Displacement
- Less than 2mm, extra-articular
- Treatment
- Conservative (buddy taping)
- Outcome
- 85-90% good results
- Displacement
- Greater than 2mm or intra-articular
- Treatment
- ORIF
- Outcome
- 80-85% good results
- Displacement
- Any displacement
- Treatment
- Conservative (buddy taping)
- Outcome
- 85-90% good results
BUDDYLesser Toes
Hook:BUDDY: Buddy taping, Usually sufficient, Displacement tolerated, Displacement less critical, Yes conservative!
Overview and Epidemiology
Phalangeal fractures of the foot are the most common foot fractures. Great toe (hallux) fractures require better alignment due to their importance in push-off, while lesser toe fractures are usually treated conservatively.
Definition
Phalangeal fracture foot: Fracture of the phalanges of the foot, which:
- Location: Great toe (hallux) or lesser toes (2nd-5th)
- Pattern: Proximal, middle, or distal phalanx
- Treatment: Usually conservative, ORIF for great toe displacement
- Outcome: Good with proper treatment
Great toe (hallux):
- Most important: Critical for push-off and gait
- Requires better alignment: Displacement greater than 2mm or intra-articular step-off requires ORIF
- IP joint: Most critical joint
Lesser toes (2nd-5th):
- Usually conservative: Buddy taping and protected weight bearing
- Tolerates displacement: Less critical than great toe
- ORIF rarely needed: Only for severe displacement or open fractures
Epidemiology
- Incidence: Among the most common foot fractures and a frequent emergency-department / fracture-clinic presentation
- Toe distribution: In a 339-patient cohort the first toe (38%) and fifth toe (30%) were most commonly fractured
- Mechanism: Stubbing or crush accounts for about 76% of cases; barefoot/open-footwear injuries predominate
- Displacement: Over 95% are displaced less than 2mm and amenable to conservative care
- Age: All ages; median patient age around 40-45 years, no strong sex predominance
- Associated injuries: Nailbed laceration (making distal fractures effectively open), open crush wounds, adjacent metatarsal injury
Great toe (hallux) most important - Critical for push-off and gait. Displacement greater than 2mm or intra-articular step-off requires ORIF. Lesser toes usually conservative with buddy taping.
Anatomy and Pathophysiology
Phalangeal Anatomy
Great toe (hallux):
- Proximal phalanx: Largest, articulates with 1st metatarsal
- Distal phalanx: Smaller, tuft fractures common
- IP joint: Interphalangeal joint, critical for push-off
- Function: Critical for gait and push-off
Lesser toes (2nd-5th):
- Proximal phalanx: Articulates with metatarsal
- Middle phalanx: 2nd-4th toes (3rd toe may have only 2 phalanges)
- Distal phalanx: Tuft fractures common
- Function: Less critical than great toe
Deforming forces:
- Great toe: Flexor and extensor tendons
- Lesser toes: Similar but less significant
- Intrinsic muscles: Minimal deforming force
Pathophysiology
Injury mechanism:
- Crush injury: Most common (stubbing, dropping object)
- Direct trauma: To toe
- Axial loading: During push-off
Why great toe requires better alignment:
- Push-off function: Critical for gait
- IP joint: Most important joint
- Arthritis risk: Malunion causes arthritis
Why lesser toes usually conservative:
- Less critical function: Tolerates displacement
- Compensatory motion: Adjacent toes compensate
- Good healing: Most heal with conservative treatment
Classification Systems
Location-Based Classification
Great toe (hallux):
- Proximal phalanx
- Distal phalanx
- IP joint
- Treatment: Conservative or ORIF
Lesser toes (2nd-5th):
- Proximal phalanx
- Middle phalanx (2nd-4th)
- Distal phalanx
- Treatment: Usually conservative
Location guides treatment approach.
Clinical Assessment

History
Symptoms:
- Toe pain: Pain in affected toe
- Swelling: Localised to toe
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: Crush injury, stubbing, direct trauma
Risk factors:
- Crush injuries
- Stubbing toes
- Direct trauma
Physical Examination
Inspection:
- Swelling in toe
- Ecchymosis (may be delayed)
- Deformity (angulation, rotation)
Palpation:
- Tenderness over fracture site
- Crepitus (if unstable)
- Deformity (if displaced)
Range of Motion:
- Toe ROM limited and painful
- IP joint ROM (great toe)
Special tests:
- Alignment check: Check for angulation and rotation
- IP joint stability: Test great toe IP joint
- Weight bearing: Pain with weight bearing
Check alignment carefully - Great toe requires better alignment (displacement greater than 2mm or intra-articular step-off requires ORIF). Lesser toes usually tolerate displacement. Check for angulation and rotation. Always lift the nail / inspect the nailbed on a distal phalanx fracture - a subungual haematoma over a fracture signals an open injury.
Differential Diagnosis
- Distinguishing features
- Acute stub/crush, focal bony tenderness, cortical break on film
- Key investigation
- AP/oblique radiograph
- Pitfall
- Miss nailbed = miss open fracture
- Distinguishing features
- Diffuse tenderness, no cortical break, no point bony pain
- Key investigation
- Radiograph normal
- Pitfall
- Over-imaging; treat symptomatically
- Distinguishing features
- Two phalanges in little toe (about 26% of people), no acute pain
- Key investigation
- Compare contralateral foot
- Pitfall
- Variant misread as fracture
- Distinguishing features
- Atraumatic overuse pain in athlete, plantar base tenderness
- Key investigation
- Oblique radiograph, MRI if early
- Pitfall
- Normal AP film falsely reassures
- Distinguishing features
- Hot, red, exquisitely tender joint, no trauma, raised urate
- Key investigation
- Joint aspirate, serum urate
- Pitfall
- Mistaking flare for fracture
- Distinguishing features
- Plantar hallux pain on push-off, not on the phalanx
- Key investigation
- Sesamoid/axial view, MRI
- Pitfall
- Bipartite sesamoid mimics fracture
Malrotation vs Angulation: What Actually Needs Reducing
The controversies note that malrotation and scissoring - not sagittal angulation - are the real reasons to reduce a toe; here is how to assess it.
- Rotation is the villain. Lesser toes tolerate considerable sagittal and coronal angulation, but malrotation makes the toe scissor or override its neighbour, producing painful footwear conflict, callosities and pressure sores — so rotation, not the angle, is the key operative indication in the lesser toes.
- How to detect rotation. Compare the plane of the nail with the adjacent uninjured toes (a rotated toe's nail faces the wrong way), look for scissoring or overlap on weight-bearing, and check that the toe points straight on standing — clinical assessment beats the radiograph for rotation.
- The hallux is stricter. The great toe tolerates far less; articular incongruity of the IP or MTP joint, malrotation, or displacement over about 2 mm justify reduction or fixation, because the hallux drives push-off and a malunion there is symptomatic.
- The practical rule. Reduce for malrotation, scissoring, an intra-articular step-off (especially the hallux), or an open injury; accept modest isolated angulation in a lesser toe that sits straight and fits a shoe.
Q: A lesser toe fracture is angulated but the patient's main problem is the toe crossing its neighbour - what matters and how do you assess it? A: Malrotation, not sagittal angulation, is the key indication to reduce a lesser toe, because a rotated toe scissors/overrides and causes footwear conflict and pressure sores. Assess by comparing the nail plane with the other toes and looking for scissoring on weight-bearing. Lesser toes tolerate angulation; the hallux is stricter (reduce for articular incongruity, malrotation, or displacement over ~2 mm).
Investigations
Standard X-ray Protocol
AP view:
- Shows fracture pattern
- Assess displacement
- Check alignment
Lateral view:
- Shows angulation
- Assess IP joint (great toe)
Oblique view:
- May show fracture better
- Less commonly needed
Key point: X-rays usually sufficient for diagnosis.
Management Algorithm
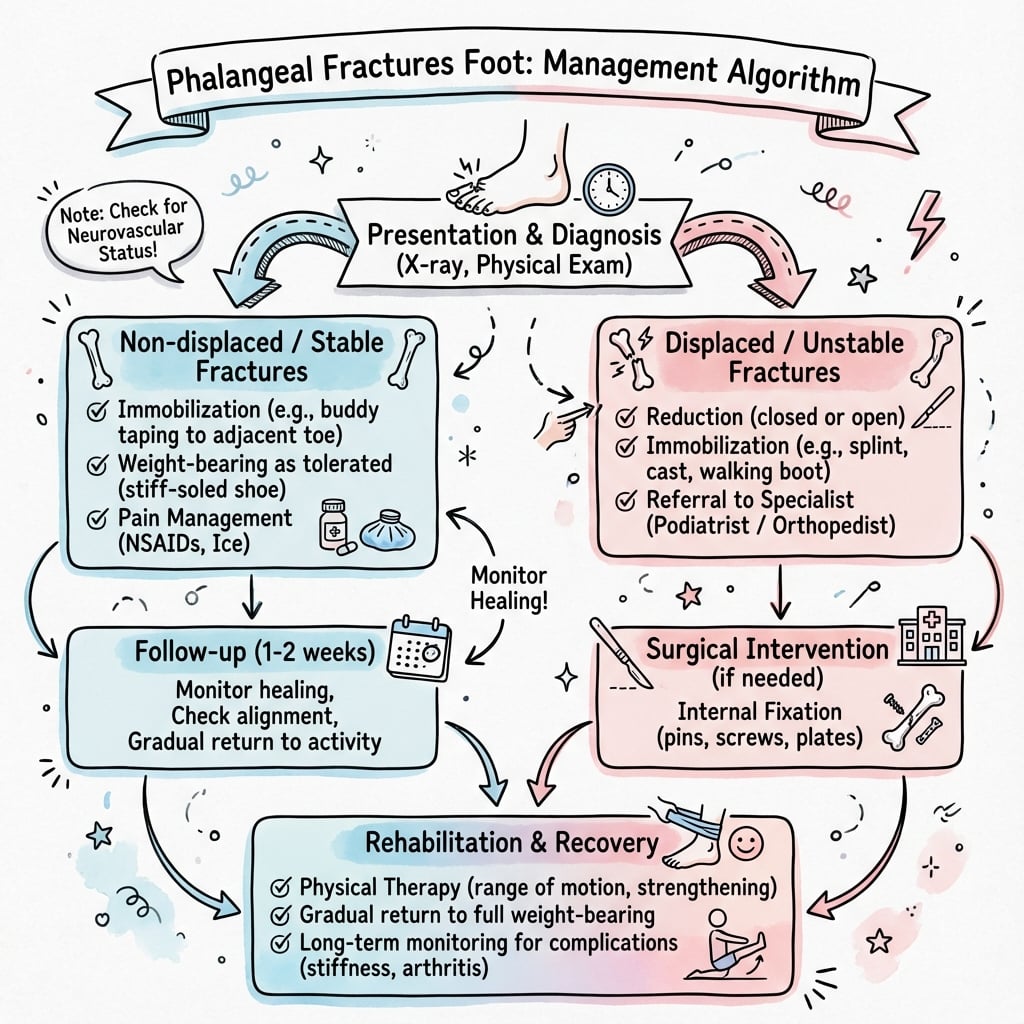
Management Pathway
Phalangeal Fracture Foot Management
X-rays usually sufficient for diagnosis - AP and lateral views show fracture pattern and displacement. Assess alignment, articular involvement, and displacement.
Great toe requires better alignment - Displacement greater than 2mm or intra-articular step-off requires ORIF. Conservative treatment for non-displaced or minimally displaced. Success rate 80-85% with ORIF.
Lesser toes usually conservative - Buddy taping and protected weight bearing usually sufficient. ORIF rarely needed - only for severe displacement or open fractures. Success rate 85-90% with conservative treatment.
Intra-articular fractures require ORIF if step-off greater than 2mm - Prevents arthritis. Great toe IP joint most critical. Screw or K-wire fixation. Success rate 80-85%.
GREATTreatment Decision
Hook:GREAT: Great toe critical, Requires better alignment, Extra care needed, Articular fractures ORIF, Treatment ORIF if displaced!
Surgical Technique
ORIF Great Toe Technique
Indications:
- Displacement greater than 2mm
- Intra-articular step-off greater than 2mm
- Unstable fracture pattern
Approach:
- Medial or dorsal approach
- Expose fracture
- Protect neurovascular structures
Technique:
- Exposure: Medial or dorsal approach to great toe, expose fracture, protect neurovascular structures
- Reduction: Anatomic reduction of fracture, restore IP joint congruity if intra-articular
- Fixation: Screws (1.5-2.0mm) or K-wires (1.0-1.5mm)
- Verification: Confirm reduction and hardware position fluoroscopically
Advantages:
- Restores alignment
- Prevents arthritis
- Allows early motion
ORIF for great toe displacement.
How to Reduce and Buddy-Tape a Toe Fracture
The topic repeatedly prescribes closed reduction and buddy taping but never describes the technique — here is the practical "how".
- Anaesthetise first. For a displaced or painful reduction use a digital (ring) block (or a hallux block) at the base of the toe; a bloodless, pain-free field lets you feel the reduction.
- The reduction manoeuvre. Apply longitudinal traction, then re-create and reverse the deformity; for a dorsally-angulated proximal phalanx a pencil or a finger placed in the web space as a fulcrum helps lever the fragment down. Confirm rotation and length clinically, then re-image.
- Buddy taping done properly. Strap the injured toe to the adjacent, longer, more stable toe, with a gauze or felt spacer between the toes to prevent skin maceration and pressure sores; add a rigid-soled or post-operative shoe that offloads toe-off, and encourage early protected weight-bearing.
- Pitfalls. Do not tape skin-to-skin (maceration), do not buddy-tape across an open or nailbed wound, and re-check the neurovascular status and rotation after taping.
Q: How do you reduce and immobilise a displaced lesser-toe fracture? A: Digital (ring) block, then longitudinal traction and reversal of the deformity (a pencil/finger in the web space as a fulcrum for a dorsally-angulated proximal phalanx). Immobilise by buddy taping to the adjacent stable toe with a gauze/felt spacer between the toes (never skin-to-skin, never across an open wound), plus a rigid-soled shoe and early protected weight-bearing; recheck rotation and perfusion afterwards.
TOEPhalangeal Fracture Foot Features
Hook:TOE: Toe fractures, Often conservative, Except great toe displacement!
Complications
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate reduction
- Prevention/Management
- Anatomic reduction, ORIF if needed
- Incidence
- 10-15%
- Risk Factors
- Intra-articular malunion
- Prevention/Management
- Anatomic reduction, ORIF if step-off
- Incidence
- 10-15%
- Risk Factors
- Prolonged immobilization
- Prevention/Management
- Early motion, buddy taping
- Incidence
- 2-5%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation
Malunion
5-10% incidence:
- Cause: Displacement, inadequate reduction
- Prevention: Anatomic reduction, ORIF if needed
- Management: Corrective osteotomy if symptomatic
Arthritis
10-15% incidence (if intra-articular malunion):
- Cause: Intra-articular step-off, malunion
- Prevention: Anatomic reduction, ORIF if step-off greater than 2mm
- Management: IP joint fusion if severe
Postoperative Care
Immediate Postoperative
- Immobilisation: Buddy taping or splint
- Weight bearing: Protected weight bearing
- ROM: Toe ROM exercises early
- PT: Not usually needed
Rehabilitation Protocol
Weeks 0-3:
- Buddy taping or splint
- Protected weight bearing
- Toe ROM exercises
Weeks 3-4:
- Remove K-wires if used
- Progressive weight bearing
- Full activity
Weeks 4-6:
- Full weight bearing
- Return to sport (6-8 weeks)
Outcomes and Prognosis
Overall Outcomes
Conservative treatment:
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Great toe: 80-85% good results
ORIF (great toe):
- Success rate: 80-85% (union, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Arthritis: 10-15% develop IP joint arthritis
Conservative (lesser toes):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 85-90% return to pre-injury level
- Complications: Rare
Long-Term Prognosis
Arthritis progression:
- With proper treatment: 10-15% develop IP joint arthritis (great toe)
- Without treatment: 20-30% develop arthritis
- Risk factors: Intra-articular malunion, displacement
Guidelines, Registries & Global Practice
Global epidemiology. Toe phalangeal fractures are among the most common foot fractures worldwide. The first and fifth toes account for roughly two-thirds of cases, and about three-quarters arise from stubbing or crush in barefoot/open-footwear settings - a pattern reproduced across high- and low-resource populations. Over 95% are minimally displaced.
- Default stance
- Conservative: buddy taping + rigid-sole shoe
- Surgical threshold
- Displaced intra-articular hallux, open, gross deformity
- Follow-up
- Selective; ED advice for stable injuries
- Default stance
- Conservative; reduce ED-to-clinic burden
- Surgical threshold
- As above; few need theatre (about 3%)
- Follow-up
- Virtual / discharge for stable undisplaced (evidence-led)
- Default stance
- Non-operative for most; anatomic care of hallux IPJ
- Surgical threshold
- Intra-articular step-off, unstable/rotated
- Follow-up
- Radiographic check if reduced/fixed
- Default stance
- Conservative default; function over radiographic perfection
- Surgical threshold
- Hallux articular incongruity, open, malrotation
- Follow-up
- Symptom-driven
- No dedicated arthroplasty/implant registry tracks toe phalangeal fractures (no implants survived long-term)
- Evidence is observational: large cohorts confirm excellent conservative outcomes (median AOFAS 100)
- Convergent global guidance: conservative care is the default everywhere
- Well-resourced: ready radiographs, ED nailbed repair, selective CT, percutaneous K-wiring when indicated
- Limited-resource: clinical diagnosis and buddy taping suffice for most; reserve scarce imaging/theatre for open, intra-articular hallux, or grossly deformed injuries
- Outcomes are comparable because the great majority need only protection and time
Phalangeal fractures of the foot are a common viva topic. Know that great toe most important (requires better alignment, displacement greater than 2mm requires ORIF), lesser toes usually conservative (buddy taping, 85-90% good results), intra-articular step-off requires ORIF (prevents arthritis), and usually conservative treatment. Be prepared to discuss the difference between great toe and lesser toe treatment.
Controversies and Areas of Uncertainty
Evidence (Eves & Oddy, 2016) shows only about 3% of toe phalangeal fractures need surgery and none developed symptomatic malunion at 2 years. Many units now discharge stable, undisplaced fractures directly from ED with self-care advice rather than routine fracture-clinic review.
The "greater than 2mm displacement or intra-articular step-off" threshold for the hallux is pragmatic, not trial-derived. No randomised data define the exact cut-off; decisions weigh articular involvement, instability, rotation and patient demand.
Lesser toes tolerate considerable angulation; significant malrotation or scissoring is the more important indication to reduce, because it causes footwear problems and skin pressure - angulation in the sagittal/coronal plane is often accepted.
A displaced distal phalanx fracture with nailbed disruption is functionally an open fracture, but routine prophylactic antibiotic duration and the need for formal theatre washout (vs ED nailbed repair) remain debated, especially in children with Seymour-type injuries.
MCQ Practice Points
Q: Why does the great toe require better alignment than lesser toes? A: Great toe is critical for push-off and gait - Displacement greater than 2mm or intra-articular step-off requires ORIF. IP joint most critical. Success rate 80-85% with ORIF.
Q: How are lesser toe fractures treated? A: Usually conservative with buddy taping - Lesser toes tolerate displacement better than great toe. Buddy taping and protected weight bearing usually sufficient. ORIF rarely needed. Success rate 85-90% with conservative treatment.
Q: When is ORIF required for phalangeal fractures of the foot? A: Great toe displacement greater than 2mm or intra-articular step-off greater than 2mm - Prevents malunion and arthritis. Lesser toes rarely need ORIF - only for severe displacement or open fractures.
Q: What is the treatment for phalangeal fractures of the foot? A: Usually conservative with buddy taping - Most heal with buddy taping and protected weight bearing. ORIF for great toe displacement (greater than 2mm) or intra-articular step-off. Success rate 85-90% with conservative, 80-85% with ORIF.
Q: What are the complications of phalangeal fractures of the foot? A: Malunion (5-10%), arthritis (10-15% if intra-articular malunion), stiffness (10-15%) - Prevent with anatomic reduction and ORIF if needed. Early motion prevents stiffness. Success rate 85-90% with proper treatment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old patient presents with great toe pain after stubbing injury. X-rays show displaced proximal phalanx fracture of great toe with 3mm displacement and 5 degrees angulation.”
“A 25-year-old patient presents with 3rd toe pain after crush injury. X-rays show displaced middle phalanx fracture with 4mm displacement and 10 degrees angulation.”
“A 9-year-old child stubbed the great toe on a bedpost. There is a subungual haematoma, blood at the nail fold and the nail is partly lifted. Radiographs show a displaced Salter-Harris II fracture of the distal phalanx physis.”
Key Concepts
- Most common foot fractures
- Great toe (hallux) most important - requires better alignment
- Lesser toes (2nd-5th) usually conservative
- Usually conservative treatment (85-90% good results)
Classification
- Great toe: Proximal or distal phalanx, IP joint - conservative or ORIF
- Lesser toes: Proximal, middle, or distal phalanx - usually conservative
- Intra-articular: Joint involvement - ORIF if step-off greater than 2mm
- Key Factor: Hallux vs lesser toe determines management
Treatment
- Great toe non-displaced: Conservative (buddy taping, 85-90% good results)
- Great toe displaced: ORIF if greater than 2mm (80-85% good results)
- Lesser toes: Conservative (buddy taping, 85-90% good results)
- Intra-articular: ORIF if step-off greater than 2mm (80-85% good results)
Surgical Technique
- Medial or dorsal approach: Protect neurovascular structures
- Reduction: Anatomic reduction, restore IP joint congruity if intra-articular
- Fixation: Screws (1.5-2.0mm) or K-wires (1.0-1.5mm)
- Verify reduction fluoroscopically
Complications
- Malunion: 5-10% (prevent with anatomic reduction, ORIF if needed)
- Arthritis: 10-15% if intra-articular malunion (prevent with ORIF if step-off)
- Stiffness: 10-15% (prevent with early motion, buddy taping)
- Nonunion: 2-5% (prevent with rigid fixation)
Evidence Base
Demographics and functional outcome of toe fractures
- First (38%) and fifth (30%) toes most commonly fractured
- 75.6% from stubbing or crush; over 95% displaced under 2 mm
- All treated conservatively; median AOFAS 100 at 27 months
- Outcome independent of toe, phalanx, or articular involvement
Do Broken Toes Need Follow-Up in the Fracture Clinic?
- Only 2 of 65 patients (about 3%) required surgery
- No symptomatic malunion at 2 years
- Stable undisplaced fractures need no fracture-clinic follow-up
- Supports community/GP management of most toe fractures