Acetabular Overcoverage | Females | Labral Damage
Causes of Overcoverage
Critical Must-Knows
- Acetabular overcoverage causes impingement during flexion
- Lateral center-edge angle greater than 40° indicates overcoverage
- Middle-aged females predominantly affected
- Labrum crushed between rim and femoral head (inside-out damage)
- Rim trimming or periacetabular osteotomy may be needed
Clinical Pearls
- "Coxa profunda: Acetabular floor medial to ilioischial line
- "Cross-over sign: Indicates acetabular retroversion
- "Contre-coup lesion: Posteroinferior cartilage damage
- "Combined FAI (cam + pincer) most common (86%)
Critical Pincer FAI Exam Points
Pathoanatomy
Acetabular overcoverage - socket covers too much of femoral head. May be global (deep socket, protrusio) or focal (retroversion with anterior overcoverage).
LCE Angle
Lateral center-edge angle greater than 40° indicates overcoverage. Measured on AP pelvis. Normal 25-40°. Less than 25° = dysplasia.
Mechanism of Damage
Labrum crushed between rim and head (inside-out, different from cam). Contre-coup lesion: Posteroinferior acetabular cartilage damage from levering of femoral head.
Treatment
Rim trimming arthroscopically or open. Labral repair/debridement. Periacetabular osteotomy for retroversion to reorient acetabulum. Address cam if combined.
CAM-PINCam vs Pincer
| C | Cam = Femoral Alpha angle elevated |
| A | Aspherical head Bump at head-neck junction |
| M | Males (young athletes) Predominant demographic |
| P | Pincer = Acetabular LCE angle elevated |
| I | Inside-out labral damage Labrum crushed |
| N | Normal head, overcovered Socket is problem |
| C | Cam = Femoral Alpha angle elevated | M | Males (young athletes) Predominant demographic | I | Inside-out labral damage Labrum crushed |
| A | Aspherical head Bump at head-neck junction | P | Pincer = Acetabular LCE angle elevated | N | Normal head, overcovered Socket is problem |
Hook:PIN = Pincer is acetabular, Inside-out damage, Normal head!
CPCOvercoverage Signs
| C | Coxa profunda Floor touches ilioischial line |
| P | Protrusio acetabuli Head medial to line |
| C | Cross-over sign Anterior overcoverage |
| C | Coxa profunda Floor touches ilioischial line |
| P | Protrusio acetabuli Head medial to line |
| C | Cross-over sign Anterior overcoverage |
Hook:CPC = Coxa profunda, Protrusio, Cross-over for overcoverage!
CPIAcetabular Retroversion Signs
| C | Cross-over sign Anterior wall crosses posterior wall before the lateral edge |
| P | Posterior wall sign Posterior wall lies medial to femoral head centre |
| I | Ischial spine sign Ischial spine projects into the pelvis (prominent) |
| C | Cross-over sign Anterior wall crosses posterior wall before the lateral edge |
| P | Posterior wall sign Posterior wall lies medial to femoral head centre |
| I | Ischial spine sign Ischial spine projects into the pelvis (prominent) |
Hook:CPI = Cross-over, Posterior wall, Ischial spine = retroversion triad (only valid on a well-centred AP pelvis)!
Overview & Pathoanatomy
Pincer-type femoroacetabular impingement occurs when the acetabulum provides excessive coverage of the femoral head, leading to impingement during hip motion.
Types of Overcoverage
Global Overcoverage:
- Coxa profunda: Deep acetabulum with the floor touching or medial to the ilioischial line.
- Protrusio acetabuli: Femoral head projects medial to the ilioischial line. More severe form.
Focal Overcoverage:
- Acetabular Retroversion: The anterior rim extends beyond the posterior rim creating focal anterior overcoverage (cross-over sign on AP pelvis).
Pathophysiology — Mechanism of Damage
During hip flexion, the femoral head impinges on the overcovered acetabular rim. The labrum is crushed between the rim and head (inside-out damage). This differs from cam FAI, where the cartilage is sheared off the bone (outside-in) by an aspherical head while the labrum is initially spared. Beck's analysis of 302 hips confirmed these distinct patterns: pincer produces a circumferential narrow strip of rim damage with labral crushing, degeneration and ossification.
Contre-coup Lesion: As the femoral head abuts the anterior rim, it levers within the socket and drives cartilage damage at the posteroinferior acetabulum — the contre-coup lesion characteristic of pincer mechanics.
Why most FAI is combined: Isolated pincer is uncommon (16/302 in Beck's series). In practice the additive cam (shear) and pincer (crush) mechanisms coexist, which is why both the femoral and acetabular sides usually need addressing.
Clinical Presentation
History
Middle-aged females typically present with groin pain. Pain is activity-related, particularly with hip flexion. May have symptoms for longer duration than cam FAI as cartilage damage is less aggressive initially.
Examination
FADIR Test: Positive (flexion, adduction, internal rotation reproduces groin pain).
Range of Motion: Reduced rotation, particularly internal rotation in flexion.
Provocative Maneuvers: End-range flexion may cause impingement symptoms.
Investigations & Diagnosis
AP Pelvis - Key measurements:
Lateral Center-Edge (LCE) Angle: Line from center of femoral head perpendicular to a line to lateral sourcil edge. Normal 25-40°. Greater than 40° = overcoverage (pincer). Less than 25° = dysplasia.
Cross-Over Sign: Indicates acetabular retroversion. Anterior wall crosses posterior wall before reaching lateral sourcil, creating focal anterior overcoverage.
Coxa Profunda: Acetabular floor (fossa) touches or is medial to the ilioischial line.
Protrusio Acetabuli: Femoral head medial to the ilioischial line.
Management
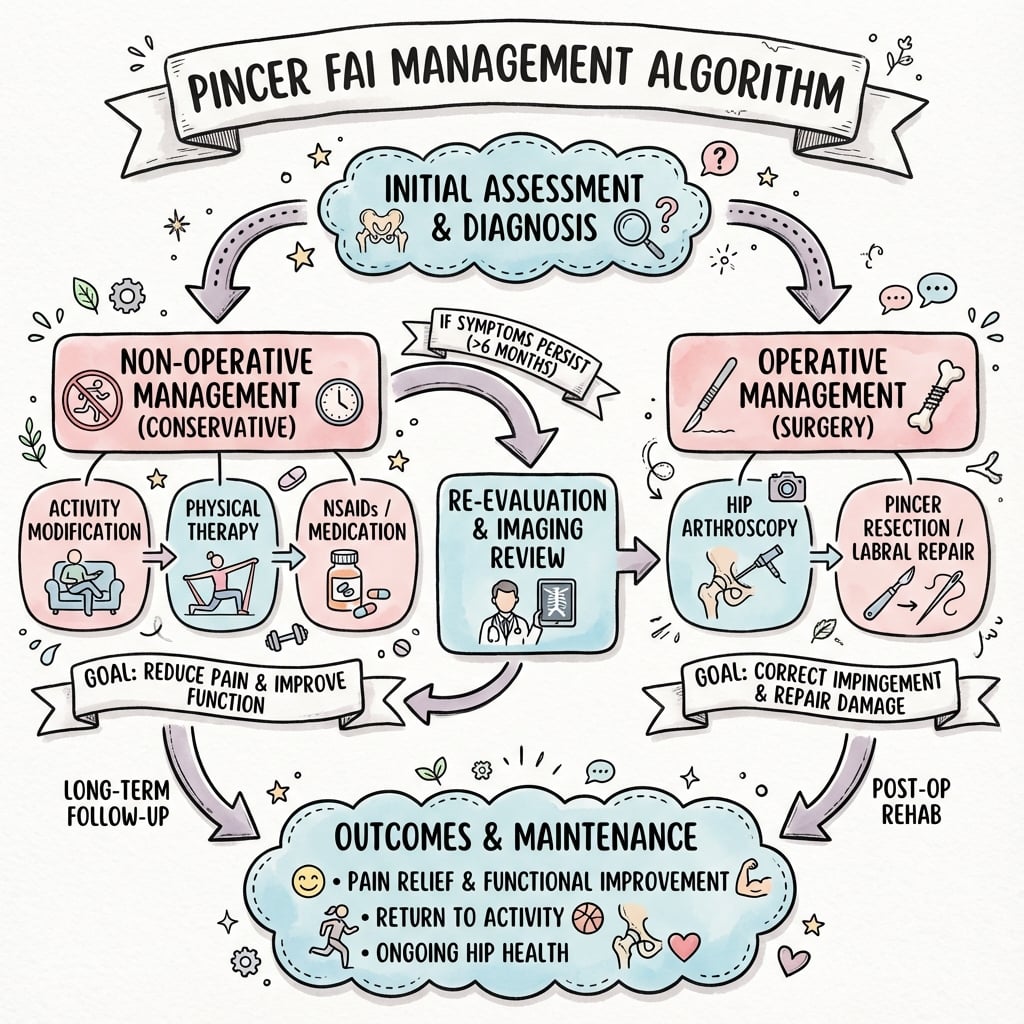
Activity Modification: Avoid end-range flexion positions.
Physiotherapy: Hip stability, core strengthening.
Analgesia/NSAIDs: Symptomatic relief.
Injection: Diagnostic and temporary therapeutic.
Complications
Iatrogenic dysplasia (over-resection)
The most feared complication: excessive rim trimming reduces the LCE angle below 25° and converts a stable overcovered hip into an unstable, undercovered one. Far more disabling than the original pathology and difficult to revise — keep resection to roughly 5-8 mm and reassess coverage dynamically.
Persistent / recurrent impingement
Most commonly from under-treating a coexisting cam component (residual alpha angle greater than 50°) or inadequate rim correction. Because most FAI is combined, failing to address both sides leads to ongoing pain.
Loss of labral seal
Labral debridement rather than repair removes the suction-seal and proprioceptive function, contributing to instability and accelerated fluid-pressurisation and cartilage wear.
Progression to osteoarthritis
Established chondral damage (Outerbridge III-IV, Tonnis 2-3) at the time of surgery predicts poor results and progression to OA — joint preservation cannot reverse advanced cartilage loss.
Arthroscopy-specific risks
Traction-related pudendal/sciatic neurapraxia and perineal injury, lateral femoral cutaneous nerve injury at portals, fluid extravasation, and (rarely) deep joint infection (one case in UK FASHIoN).
PAO-specific risks
For reverse PAO in retroversion: nerve injury (LFCN, sciatic), non-union of osteotomies, over- or under-correction, intra-articular extension, and heterotopic ossification.
Evidence Base
- Proposed femoroacetabular impingement as a mechanism of early osteoarthritis in non-dysplastic hips, based on more than 600 surgical dislocations
- Pincer mechanism: abnormal contact between an overcovering acetabular rim and the femoral head-neck junction during motion (not axial load)
- Surgical treatment aims to improve clearance for hip motion and relieve femoral abutment against the rim
- Early intervention proposed to decelerate degenerative progression in young patients
- 302 hips analysed; only 26 had isolated cam and 16 isolated pincer — combined impingement was by far the most common
- Pincer impingement: circumferential, narrow strip of acetabular cartilage damage; the labrum is crushed between rim and femoral neck (inside-out), with degeneration and ossification
- Cam impingement: anterosuperior cartilage shear with labrocartilage separation (outside-in), labrum initially spared
- Labral damage signals ongoing impingement and rarely occurs in isolation
- Defines the radiographic criteria separating pincer from cam morphology on a correctly oriented AP pelvis
- Pincer signs: cross-over (figure-of-eight) sign for retroversion, posterior wall sign, ischial spine sign, coxa profunda and protrusio for global overcoverage
- Emphasises pelvic tilt and rotation as major pitfalls that falsely create or mask a cross-over sign
- Lateral centre-edge angle quantifies coverage (overcoverage when elevated)
Differential Diagnosis
The overcovered, painful hip overlaps with several other causes of young-adult groin pain. The discriminator for pincer FAI is acetabular overcoverage with a crushed (inside-out) labrum and contre-coup posteroinferior damage.
Distinguishing Pincer FAI from Its Mimics
| 0 | 1 | 2 | 3 |
|---|---|---|---|
| Pincer FAI | Overcoverage; pain at end-range flexion; middle-aged female | LCE greater than 40°, cross-over/posterior wall/ischial spine signs; contre-coup lesion | Mistaking pelvic malrotation for a true cross-over sign |
| Cam FAI | Aspherical head-neck junction; young athletic male; outside-in shear | Alpha angle 55° or more, loss of head-neck offset; anterosuperior chondral delamination | Assuming cam only — most FAI is combined |
| Acetabular dysplasia | Undercoverage and instability, not impingement | LCE less than 20-25°, increased Tonnis angle, lateralised head | Treating as pincer and rim-trimming a dysplastic hip (disastrous) |
| Acetabular protrusio (e.g. RA, Paget, OI) | Global overcoverage with axial migration; systemic disease | Head medial to ilioischial line; bilateral | Missing the underlying systemic cause |
| Athletic pubalgia / adductor pathology | Pain over pubic symphysis/adductor origin, resisted adduction | Normal acetabular coverage; symphyseal/adductor changes on MRI | Attributing groin pain to incidental rim morphology |
| Iliopsoas tendinopathy / internal snapping hip | Anterior snapping, pain with resisted hip flexion | Dynamic ultrasound shows tendon snap; coverage normal | Operating on FAI when psoas is the pain generator |
| Hip osteoarthritis | Older patient, rest/night pain, global ROM loss | Joint space narrowing, osteophytes (Tonnis 2-3) | Offering joint preservation when OA is established |
A diagnostic intra-articular local anaesthetic injection (greater than 80% temporary relief) is the single most useful test to confirm the hip joint as the pain source before any rim-altering surgery.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Hip Pain with Overcoverage
"A 40-year-old woman has groin pain. X-ray shows LCE angle of 45° and a cross-over sign. What is the diagnosis and how do you manage her?"
Scenario 2: Combined Cam-Pincer FAI - Comprehensive Surgical Planning
"You are seeing a 32-year-old recreational runner with 14 months of progressive right groin pain in your sports clinic. He has failed 6 months of physiotherapy and activity modification. On examination, he has a positive FADIR test and reduced internal rotation in flexion (15° vs 35° on the left). His plain radiographs show an alpha angle of 65° on the lateral view and a lateral center-edge (LCE) angle of 43° on the AP pelvis, with a positive cross-over sign indicating acetabular retroversion. MR arthrogram demonstrates an anterosuperior labral tear with adjacent chondral delamination (Outerbridge grade II) and a posteroinferior chondral lesion at the acetabulum (contre-coup lesion, Outerbridge grade II). He is asking about surgical treatment. How do you counsel this patient about his diagnosis and surgical management?"
Scenario 3: Iatrogenic Hip Dysplasia After Over-Resection - Complication Management
"You are seeing a 35-year-old woman in your clinic who underwent hip arthroscopy for pincer-type FAI 9 months ago at another institution. Her pre-operative lateral center-edge (LCE) angle was 42° with a cross-over sign. The operative report documents arthroscopic rim trimming and labral debridement. She initially improved for 3 months post-operatively but has developed new symptoms over the past 6 months: a sensation of hip instability, clicking, and feeling that her hip 'wants to come out' particularly with pivoting movements. She now walks with a limp and uses a stick for stability. On examination, she has an apprehension sign with hip extension and external rotation (concerned the hip will dislocate posteriorly), and her hip feels subluxable on dynamic testing. New plain radiographs show the joint space is preserved (3mm), but the post-operative LCE angle now measures 18° (down from pre-op 42°). The femoral head appears to be subluxing laterally on the standing AP pelvis. MRI shows the labrum has been completely debrided (absent), and there is thinning of the anterior acetabular rim. What is your assessment and management plan?"
MCQ Practice Points
LCE Angle
Q: What LCE angle indicates pincer morphology? A: Greater than 40 degrees. Normal is 25-40°. Less than 25° is dysplasia.
Cross-Over Sign
Q: What does the cross-over sign indicate? A: Acetabular retroversion - the anterior wall crosses the posterior wall on AP pelvis, indicating focal anterior overcoverage.
Labral Damage Pattern
Q: What is the pattern of labral damage in pincer FAI? A: Inside-out - the labrum is crushed between the acetabular rim and femoral head. This differs from cam where damage is from shear forces (outside-in).
Controversies & Areas of Uncertainty
Does isolated pincer truly exist?
Beck's data found isolated pincer in only 16 of 302 hips, and much of the early literature may have overdiagnosed it from rotated or tilted pelvic radiographs. Many apparent "cross-over signs" disappear on correctly oriented films, raising doubt about how often pure pincer is the real pathology.
Rim trimming vs reverse PAO for retroversion
For focal anterior overcoverage from acetabular retroversion, arthroscopic rim trimming risks worsening a globally deficient (posteriorly inadequate) socket, whereas reverse periacetabular osteotomy reorients the whole acetabulum. Distinguishing focal-anterior from global retroversion (posterior wall sign, ischial spine sign) is the key, unresolved selection question.
How much surgery does the RCT evidence justify?
UK FASHIoN showed only a modest benefit over physiotherapy (iHOT-33 difference 6.8), and the Australian secondary analysis found no morphology-specific predictor of surgical benefit. The size of the true treatment effect — and which overcovered hips genuinely benefit — remains debated.
Labral repair vs reconstruction vs debridement
Repair is generally preferred to preserve the suction seal, but the calcified, degenerate labrum of long-standing pincer disease is often not repairable, and the role of labral reconstruction (graft) versus selective debridement in this setting is not settled.
Guidelines, Registries & Global Practice
Global Epidemiology
- Pincer morphology (LCE greater than 40°, cross-over sign) is found in a minority of symptomatic FAI; combined cam-pincer dominates clinical series, with isolated pincer the least common subtype (Beck: 16/302).
- Isolated pincer tends to present in middle-aged women, whereas cam-dominant disease clusters in younger active men — a consistent demographic pattern across European, North American and Asian cohorts.
- Asymptomatic overcoverage exists in the general population, so morphology alone never equals disease; the FAI syndrome requires symptoms + signs + imaging together.
Side-by-Side Guidance
How Major Bodies Frame FAI / Pincer Management
| 0 | 1 | 2 |
|---|---|---|
| NICE / BOA (UK) | Arthroscopic surgery acceptable for symptomatic FAI without OA | Strict patient selection; trained hip arthroscopists; audit of outcomes |
| AAOS / academy consensus (US) | Supports surgery for appropriately selected FAI syndrome | Confirm intra-articular source; exclude established OA before correction |
| AO Foundation / Bernese school (Europe) | Open surgical dislocation and (reverse) PAO for complex/retroverted hips | Preserve the posterior wall; reorient rather than over-resect in retroversion |
| Warwick / international FAI consensus | Triad definition: symptoms + clinical signs + imaging findings | Treat the patient, not the radiograph; conservative care is legitimate first line |
Registry & Outcome Signals
- There is no dedicated FAI implant registry (the procedure is reshaping, not implantation), so the evidence base rests on RCTs (UK and Australian FASHIoN) and large arthroscopy cohorts rather than joint registries.
- Registry-level data become relevant only downstream: iatrogenic dysplasia and failed FAI surgery feed into PAO and early arthroplasty workloads, where national joint registries (NJR, AOANJRR, SHAR) track the high revision burden of THA in patients under 55.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: MR arthrogram or dGEMRIC, dedicated hip-arthroscopy expertise, structured physiotherapy programmes, and access to PAO for retroversion.
- Limited-resource settings: diagnosis rests on a good AP pelvis and clinical examination; management is weighted toward activity modification, analgesia and physiotherapy, with surgery reserved for clear, correctable morphology and referred to centres with arthroscopic capability.
PINCER-TYPE FAI
Clinical summary
Key Facts
- •Acetabular overcoverage
- •LCE angle greater than 40 degrees
- •Middle-aged females
- •Labrum crushed (inside-out)
Overcoverage Signs (CPC)
- •Coxa profunda (floor to line)
- •Protrusio (head medial to line)
- •Cross-over sign (retroversion)
Damage Pattern
- •Inside-out labral damage
- •Labrum crushed between rim and head
- •Contre-coup lesion posteroinferiorly
Treatment
- •Rim trimming (acetabuloplasty)
- •Labral repair
- •PAO for retroversion
- •Address cam if combined