Plantar Plate Insufficiency & Lesser MTP Instability
Pain localised to the MTP joint (plantar/under the metatarsal head), synovitis/swelling, toe deviation and a positive plantar drawer test. Progresses to crossover toe. The plantar plate is hypointense on MRI; a tear shows hyperintensity at the phalangeal insertion.
Pain in the web space (commonly 3rd), radiating to the toes, with a Mulder's click and toe-splaying, but a stable MTP joint and a negative drawer. Pericapsular oedema from a plate tear can mimic a neuroma on imaging - do not confuse them.
Joint versus webPlantar plate tear versus Morton's neuroma
Hook:Plate disease is a JOINT problem (drawer +, toe drifts); a neuroma is a WEB-SPACE problem (Mulder's click, toe splays). Image to be sure.
Overview & Epidemiology
Plantar plate insufficiency is now recognised as the true pathology behind most lesser-toe metatarsophalangeal (MTP) instability and the crossover-toe deformity — a problem long misattributed to, or conflated with, a Morton's neuroma. It is predominantly a condition of middle-aged and older adults, more common in women, and overwhelmingly affects the second MTP joint (the longest lesser ray and the one that bears the most load, especially when a hallux valgus shifts weight laterally). It frequently coexists with hallux valgus, hammertoe and metatarsalgia, and is more common in inflammatory arthropathy and with chronic forefoot overload (long second metatarsal, high-heeled footwear). Recognising it as a distinct, gradeable, repairable entity — rather than vague "metatarsalgia" — is the conceptual shift the topic tests.
Pathophysiology & Pathoanatomy
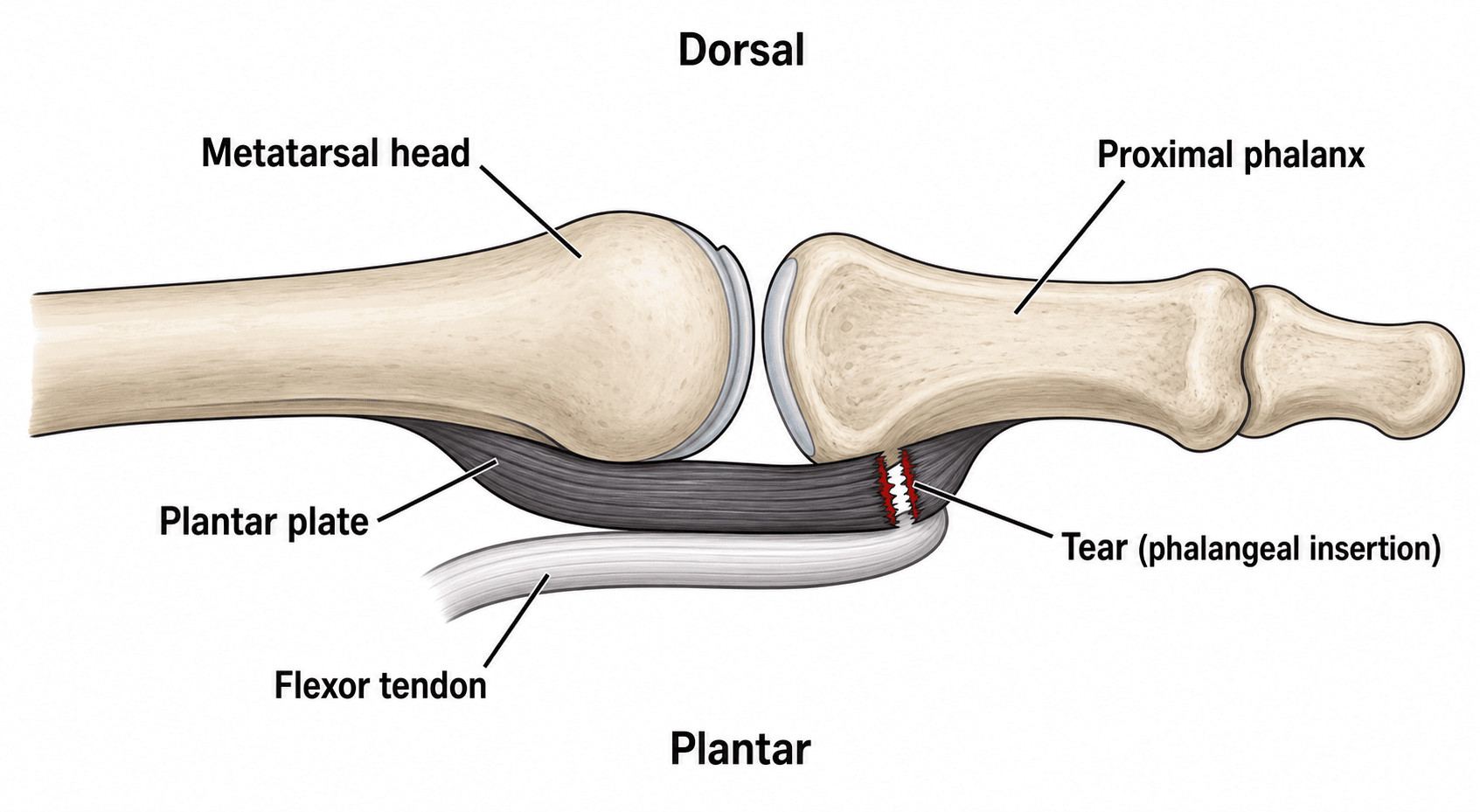
The plantar plate is a strong fibrocartilaginous structure on the plantar aspect of each lesser MTP joint. It originates loosely from the metatarsal neck and inserts firmly onto the base of the proximal phalanx, blending with the collateral ligaments, joint capsule and flexor sheath. Anatomical study shows it is the major stabiliser of the joint because of its central position and multiple attachments.
- Function: resists dorsal subluxation and hyperextension of the MTP joint, cushions load under the metatarsal head, and maintains toe alignment.
- Pathophysiology: chronic overload (e.g. long second metatarsal, hallux valgus transferring load, high heels) causes attritional degeneration and tearing, typically at the distal (phalangeal) insertion, laterally first. Loss of the plantar restraint allows dorsal and medial drift of the toe, ending in a crossover toe and ultimately MTP dislocation.
- The second MTP joint is most commonly affected.
Clinical Presentation & Assessment
History
- Plantar forefoot pain under the metatarsal head (often the second), with a feeling of "walking on a pebble" or sock bunching.
- Progressive swelling of the MTP joint and deviation of the toe (medial/dorsomedial), then crossover over the hallux.
- Often confused with, or coexists with, metatarsalgia and is mistaken for a Morton's neuroma.
Distinct from the Nery anatomical (tear-pattern) grade assessed at surgery, examiners expect the clinical deformity staging of lesser-MTP instability (the Coughlin/Coughlin-Doty system), graded by alignment and instability:
- Grade 0 — MTP pain/synovitis, no deformity; the drawer may be mildly positive.
- Grade 1 — mild malalignment, widened web space, the toe starts to deviate medially; drawer mildly positive.
- Grade 2 — moderate malalignment with dorsomedial/medial (or lateral) deviation and hyperextension; the toe is still reducible.
- Grade 3 — severe, the second toe overrides the hallux (crossover toe) with a flexible-to-fixed hammertoe; marked drawer.
- Grade 4 — dislocated, fixed crossover/dislocated MTP joint.
The drawer (vertical Lachman) test is itself graded by translatability: G0 stable, G1 under 50% subluxation, G2 over 50% subluxation, G3 frankly dislocatable, G4 fixed dislocation. Use the clinical grade to track progression and decide timing, and the Nery grade (at surgery) to judge whether a direct repair will hold.

Investigations
Diagnosis is clinical (MTP-joint pain, a graded plantar drawer and toe deviation) but confirmed and staged with imaging.
- Weight-bearing radiographs show toe malalignment, MTP subluxation or frank dislocation, a long second metatarsal and any associated hallux valgus — but the plantar plate itself is radiolucent.
- MRI is the reference standard: the normal plate is low signal; a tear shows high signal and discontinuity at the phalangeal insertion. It also grades the tear, shows associated collateral-ligament injury, and excludes a Morton's neuroma.
- High-resolution ultrasound (dynamic, with dorsiflexion stress) shows the normally hyperechoic plate developing an anechoic cleft; it is operator-dependent but cheap and dynamic.
- The Nery/Coughlin anatomical grade (assessed clinically and at surgery) runs 0 (attenuation/no tear) → I (distal transverse tear under 50% width) → II (over 50% width) → III (extensive transverse ± longitudinal) → IV (extensive tear with a buttonhole/dislocation), which guides whether repair is feasible.
Differential diagnosis of lesser-MTP / forefoot pain (imaging helps separate them): a Morton's neuroma (web-space pain, Mulder's click, stable joint — the classic confounder); Freiberg's disease (avascular necrosis of the metatarsal head, usually the 2nd, with a flattened/sclerotic head on radiographs); a metatarsal stress fracture (activity-related dorsal pain, periosteal reaction or MRI marrow oedema); inflammatory/crystal arthritis (rheumatoid synovitis or gout — bilateral, raised inflammatory markers); and lesser-MTP osteoarthritis or synovitis of another cause. Plantar plate disease is distinguished by MTP-joint (not web-space) pain, a positive drawer and progressive toe deviation — but it commonly coexists with several of these.
0 → IV by tear extentNery / Coughlin anatomical grades
Hook:Grades climb 0→IV with the size and pattern of the tear; the higher the grade, the less a simple repair will hold.
Management
Non-operative
- First-line for early/lower-grade disease and the comorbid patient.
- Toe taping/strapping (plantarflexion taping to hold the toe down), stiff-soled shoes / rocker sole, metatarsal pads/orthoses to off-load the head, activity modification and NSAIDs.
- Corticosteroid injection is used cautiously (risk of further plate attenuation and deformity).
A direct anatomic repair needs plate tissue to hold the suture. In a Nery Grade IV (buttonhole/dislocation) tear, a chronically dislocated joint, or a destroyed inflammatory (rheumatoid) forefoot, repair is unreliable — so know the alternatives:
- Flexor-to-extensor (Girdlestone-Taylor) transfer: the flexor digitorum longus is detached and transferred dorsally to act as a dynamic plantar restraint/flexor of the MTP, used for a flexible deformity or when the plate cannot be repaired (often combined with a Weil osteotomy).
- Salvage of the destroyed/rheumatoid joint: lesser metatarsal-head resection / Stainsby forefoot reconstruction, MTP excisional arthroplasty, or (with first-ray surgery) the classic rheumatoid forefoot reconstruction (first-MTP arthrodesis + lesser metatarsal-head excision).
- Counsel recurrence risk: inflammatory/rheumatoid feet recur more after any repair (the consistent caveat in the outcome series), so set expectations and have a salvage plan.
So match the operation to the tissue: repair a repairable plate, transfer/realign a flexible irreparable one, and salvage the destroyed joint.
Complications
Both the disease and its surgery have characteristic problems the examiner expects you to anticipate.
- Note
- The natural history of an untreated tear — deformity becomes fixed and the joint dislocates
- Note
- After repair, particularly in high-grade tears, inflammatory disease or an uncorrected long metatarsal or hallux valgus
- Note
- A toe that no longer purchases the ground — a recognised problem after a Weil osteotomy (from plantar translation of the metatarsal head and intrinsic imbalance)
- Note
- Over-shortening or mal-position of the osteotomy shifts load to adjacent metatarsal heads
- Note
- Loss of MTP motion after repair/osteotomy
- Note
- Repeated MTP steroid injections accelerate plate attenuation and can precipitate deformity — use sparingly
PLATEPlantar Plate Insufficiency
Hook:A failed PLATE drifts the toe up and over (crossover).
Guidelines, Registries & Global Practice
Global Practice Picture
Plantar plate insufficiency is increasingly recognised internationally as the true pathology behind lesser MTP instability and crossover toe, supported by anatomical, imaging and surgical-outcome work (notably from Nery and Coughlin). The consistent principles: localise to the MTP joint and grade with the drawer test; confirm and differentiate from Morton's neuroma with MRI/ultrasound; manage conservatively first; and repair the plate (commonly with a Weil osteotomy) for persistent instability.
Side-by-Side Synthesis
- Plantar plate tear
- MTP joint (plantar to head)
- Morton's neuroma
- Web space
- Plantar plate tear
- Positive drawer; toe deviation
- Morton's neuroma
- Mulder's click; toe splaying
- Plantar plate tear
- Unstable
- Morton's neuroma
- Stable
- Plantar plate tear
- Plate hyperintensity/cleft at insertion
- Morton's neuroma
- Web-space mass
- Plantar plate tear
- Plantar plate repair + Weil osteotomy
- Morton's neuroma
- Neuroma excision/decompression
Evidence Base
All four citations below were checked against PubMed. The anatomy/staging and the operation rest on the Nery/Coughlin body of work (the plantar plate as primary stabiliser, the second MTP as the usual site, dorsal-approach repair + Weil osteotomy), and Linklater anchors the imaging diagnosis and the Morton's-neuroma distinction. The outcome evidence is Level IV case series (Flint/Coughlin's 97-foot dorsal-approach series, AOFAS 49→81; Doh's plantar-approach series), so quote the operation as "reliable in case series" rather than RCT-proven — and note the recurring caveat that inflammatory (rheumatoid) feet recur more. No randomised comparison of approaches or against conservative care exists.
Lesser metatarsophalangeal joint instability: prospective evaluation and repair of plantar plate and capsular insufficiency
- Prospective study; the plantar plate is the major stabiliser of the lesser MTP joint
- The second MTP joint was most commonly affected (63%); Grade III tears were most frequent
- Direct plantar plate repair through a dorsal approach with a Weil osteotomy and lateral soft-tissue reefing restored alignment
- AOFAS score improved from a mean of 52 to 92 points
Imaging of Lesser Metatarsophalangeal Joint Plantar Plate Degeneration, Tear, and Repair
- Plantar plate degeneration/tear typically involves the second MTP joint at the lateral proximal phalangeal insertion
- It is frequently confused with a second web-space Morton's neuroma
- The normal plate is hypointense on MRI and hyperechoic on ultrasound; a tear shows hyperintensity (anechoic cleft on US), more conspicuous with dorsiflexion stress
- Pericapsular oedema/fibrosis from a tear should not be misread as a Morton's neuroma
Plantar Plate Repair for Lesser Metatarsophalangeal Joint Instability
- Prospective case series of 97 feet with 138 plantar plate tears repaired through a dorsal approach with a Weil osteotomy
- 80 percent of patients reported good-to-excellent satisfaction at 12 months
- Mean VAS pain fell from 5.4 to 1.5 and mean AOFAS rose from 49 to 81; MTP range of motion decreased slightly (43 to 31 degrees)
- The paper pull-out (toe purchase) test improved from 42 to 54 percent of toes
Radiologic Outcomes of Plantar Plate Repair through a Plantar Approach for the Dislocated Metatarsophalangeal Joint of the Lesser Toe
- 31 patients with a subluxated/dislocated second or third MTP joint repaired through a PLANTAR approach (with a shortening metatarsal osteotomy via a dorsal incision in longer rays)
- The plantar approach gives excellent direct visualisation of the torn plate; reduction (MTP overlap distance) improved significantly and was maintained at follow-up
- No clinical/radiologic factor independently predicted recurrence, but rheumatoid feet showed a recurrence tendency (3 of 12 RA feet recurred; 60 percent of recurrences were RA feet)
- Supports the plantar approach as an alternative to the dorsal/Weil technique for the dislocated joint