Dial Test | Arcuate Sign | Combined PCL | Reconstruction
- PLC = primary restraint to EXTERNAL ROTATION and VARUS
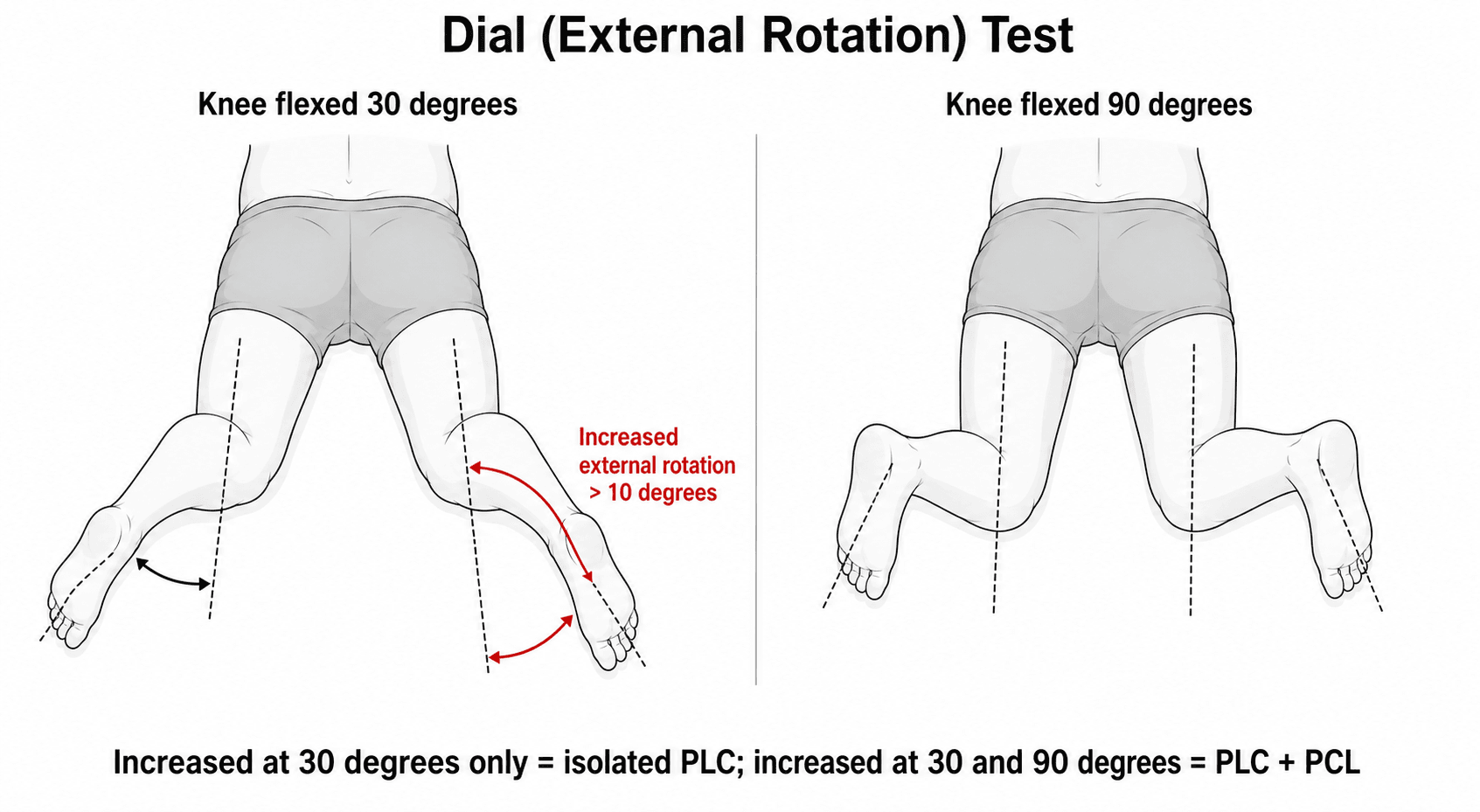
- Dial test at 30 degrees only = isolated PLC. At 30 AND 90 degrees = combined PCL
- Arcuate sign on X-ray = avulsion of PLC attachment to fibula
- Missing PLC injury = ACL/PCL graft failure
- Reconstruct rather than repair for best outcomes
- “Varus thrust gait = chronic PLC deficiency
- “Common peroneal nerve at risk (20%+ injuries)
- “LaPrade anatomic reconstruction = gold standard
- “Address varus alignment with osteotomy before/with PLC
Dial test at 30 and 90 degrees distinguishes isolated PLC (30 only) from combined PCL/PLC (30 and 90). Critical for surgical planning.
PLC injuries often missed. Always check with PCL and ACL injuries. Missing PLC leads to cruciate graft failure.
Common peroneal nerve injury in 20%+ of PLC injuries. Check foot drop, lateral leg sensation. Document preoperatively.
Reconstruction superior to repair. Isolated repairs have high failure rates. LaPrade anatomic reconstruction is gold standard.
- 30 Degrees
- Symmetric
- 90 Degrees
- Symmetric
- Diagnosis
- No injury
- 30 Degrees
- Greater than 10 degree increase
- 90 Degrees
- Symmetric
- Diagnosis
- PLC injury only
- 30 Degrees
- Greater than 10 degree increase
- 90 Degrees
- Greater than 10 degree increase
- Diagnosis
- PCL + PLC injury
FAPPLC Structures
Hook:FAP structures form the PLC!
VERSEPLC Function
Hook:The PLC controls VERSE directions of instability!
Overview and Epidemiology
PLC injuries are frequently missed on initial presentation. Have high index of suspicion with PCL and ACL injuries. Missing PLC leads to cruciate graft failure - must address all injured structures.
- 16% of knee ligament injuries
- 60-70% with cruciate injury
- Usually high-energy trauma
- Sports: football, soccer, skiing
- MVCs common cause
- Varus force: Direct blow to medial knee
- Hyperextension: With varus component
- External rotation: On planted foot
- Knee dislocation: Multiligament pattern
- Contact sports: Direct lateral blow
Pathophysiology and Mechanisms
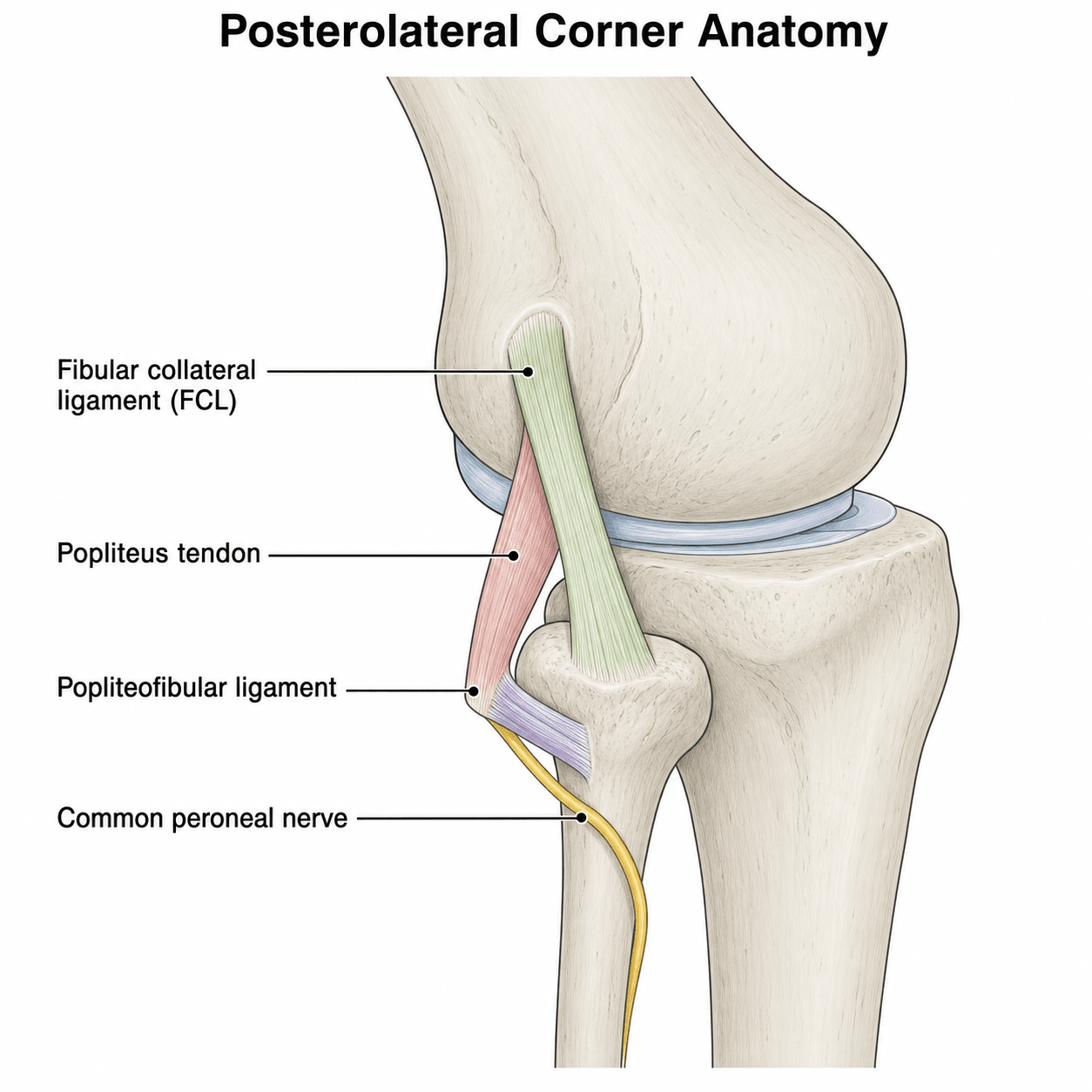
PLC Anatomy (LaPrade)
- Origin: Lateral femoral epicondyle
- Insertion: Lateral fibular head
- Primary varus restraint
- Popliteus tendon: Femoral origin, inserts on tibia
- Popliteofibular ligament: Connects popliteus to fibula
- Primary external rotation restraint
Static stabilizer, arcuate ligament.
Common peroneal nerve injury occurs in 20%+ of PLC injuries. Check ankle dorsiflexion and toe extension. Document sensation. Nerve injury affects rehabilitation and prognosis.
Classification Systems
PLC Injury Grading
- External Rotation
- Less than 5 degree increase
- Varus
- Minimal
- Implication
- Sprain, intact structures
- External Rotation
- 5-10 degree increase
- Varus
- Moderate
- Implication
- Partial tear
- External Rotation
- Greater than 10 degree increase
- Varus
- Significant
- Implication
- Complete rupture, surgery indicated
Grade based on dial test asymmetry compared to contralateral side.
Fanelli Classification of PLC Injury
Beyond the dial-based grade and the isolated-versus-combined split, the examiner expects the Fanelli classification, which grades the injury by external rotation plus the degree of varus laxity - and so maps onto which structures are torn.
- Findings
- Increased external rotation ONLY (no varus laxity)
- Structures involved
- Popliteofibular ligament and popliteus tendon
- Findings
- Increased external rotation plus MILD varus laxity (about 5 mm)
- Structures involved
- Popliteofibular ligament, popliteus, and an attenuated FCL
- Findings
- Increased external rotation plus GROSS varus laxity (about 10 mm)
- Structures involved
- FCL, popliteofibular ligament and popliteus all disrupted, with lateral capsular avulsion (often with cruciate injury)
The progression from A to C reflects increasing FCL involvement: a pure rotational (Type A) injury spares the FCL, whereas the varus laxity of Types B and C signals FCL attenuation then complete rupture.
The Fanelli classification grades the PLC injury by rotation and varus: Type A = rotation only (popliteus/PFL, FCL intact); Type B = rotation plus mild varus (FCL attenuated); Type C = rotation plus gross varus (FCL ruptured plus capsular avulsion, often with a cruciate). The appearance of varus laxity is the clue that the FCL - the primary varus restraint - has failed, which raises the injury from A to B or C and makes reconstruction (rather than rehab) the answer.
The Multiligament Knee: Schenck Classification and Vascular Assessment
PLC injuries are frequently part of a knee dislocation, so the examiner expects the Schenck (KD) classification and the vascular assessment that a dislocated knee demands - the topic flags "check vascular injury / ABI / CT angiography" but never sets it out.
- Ligament pattern
- One cruciate intact (single cruciate plus a collateral)
- Ligament pattern
- Both cruciates torn, collaterals intact
- Ligament pattern
- Both cruciates plus ONE collateral - subdivided KD-IIIM (medial) or KD-IIIL (lateral/PLC)
- Ligament pattern
- Both cruciates plus BOTH collaterals
- Ligament pattern
- Dislocation with a periarticular fracture (fracture-dislocation)
A PLC injury with both cruciates is a KD-IIIL. The suffix C denotes an associated arterial injury and N a nerve injury.
Vascular assessment (the limb-threatening priority): the popliteal artery is tethered proximally at the adductor hiatus and distally at the soleal arch, so it is at high risk in any dislocation.
- Examine pulses and measure the ankle-brachial index (ABI).
- ABI of 0.9 or above: serial vascular observation is acceptable.
- ABI under 0.9: CT angiography to exclude an intimal or occlusive injury.
- Hard signs (absent pulses, expanding haematoma, bruit, active bleeding): straight to the operating theatre and vascular surgery - do not delay for imaging.
Classify the multiligament knee by Schenck (a both-cruciate-plus-PLC injury is KD-IIIL; add C for arterial, N for nerve injury) and never forget the popliteal artery. Examine pulses and the ankle-brachial index: 0.9 or above allows serial observation, under 0.9 mandates CT angiography, and hard signs of ischaemia go straight to theatre. Occult intimal injury can declare late, so serial examination is essential even with initially normal pulses.
Clinical Assessment
- Mechanism: Varus blow, hyperextension, MVA
- Pain: Lateral and posterolateral knee
- Instability: Varus, giving way
- Gait: Varus thrust (chronic)
- Nerve symptoms: Foot drop, numbness
- Dial test: 30 and 90 degrees (KEY)
- Varus stress: 0 and 30 degrees
- External rotation recurvatum: Lift toe
- Reverse pivot shift: Clunk on extension
- Peroneal nerve: Motor and sensory
Patient prone, knees flexed 30 degrees (then 90). Externally rotate both feet simultaneously. Compare tibial thigh angle. Greater than 10 degree asymmetry = positive. At 30 degrees only = isolated PLC. At 30 AND 90 = combined PCL.
Key Clinical Pearls
Lateral thrust during stance phase. Indicates chronic PLC deficiency and significant laxity.
Patient supine, lift great toe. Positive = tibia drops into hyperextension and external rotation.
Differential Diagnosis
- Key discriminator
- Dial positive at 30 only; varus laxity
- Best test
- Dial at 30 and 90; varus stress
- Pitfall
- Easily missed when subtle
- Key discriminator
- Dial positive at 30 AND 90; posterior sag
- Best test
- Posterior drawer + dial
- Pitfall
- Operating on PCL alone
- Key discriminator
- Posterior sag; dial symmetric
- Best test
- Posterior drawer
- Pitfall
- Mislabelling as PLC
- Key discriminator
- Varus laxity at 30 without rotational laxity
- Best test
- Varus stress at 30
- Pitfall
- Underestimating popliteus involvement
- Key discriminator
- Gross instability, possible vascular injury
- Best test
- ABI, CT angiography
- Pitfall
- Missing limb-threatening ischaemia
- Key discriminator
- Foot drop without major laxity
- Best test
- Motor/sensory exam, NCS
- Pitfall
- Attributing all weakness to pain

DRIVEPLC Examination
Hook:DRIVE through PLC examination!
Investigations
MRI Assessment
Good for PLC but structures can be subtle.
- FCL: Coronal images
- Popliteus: Sagittal and coronal
- Popliteofibular ligament: Often difficult to see
- Arcuate complex: Posterolateral capsule
Peroneal nerve edema, bone bruise, cruciate tears.
Arcuate sign = avulsion fracture of fibular head/styloid on plain X-ray. Pathognomonic for PLC injury. Indicates avulsion of FCL and/or biceps femoris. Suspect multiligament injury.


Management Algorithm
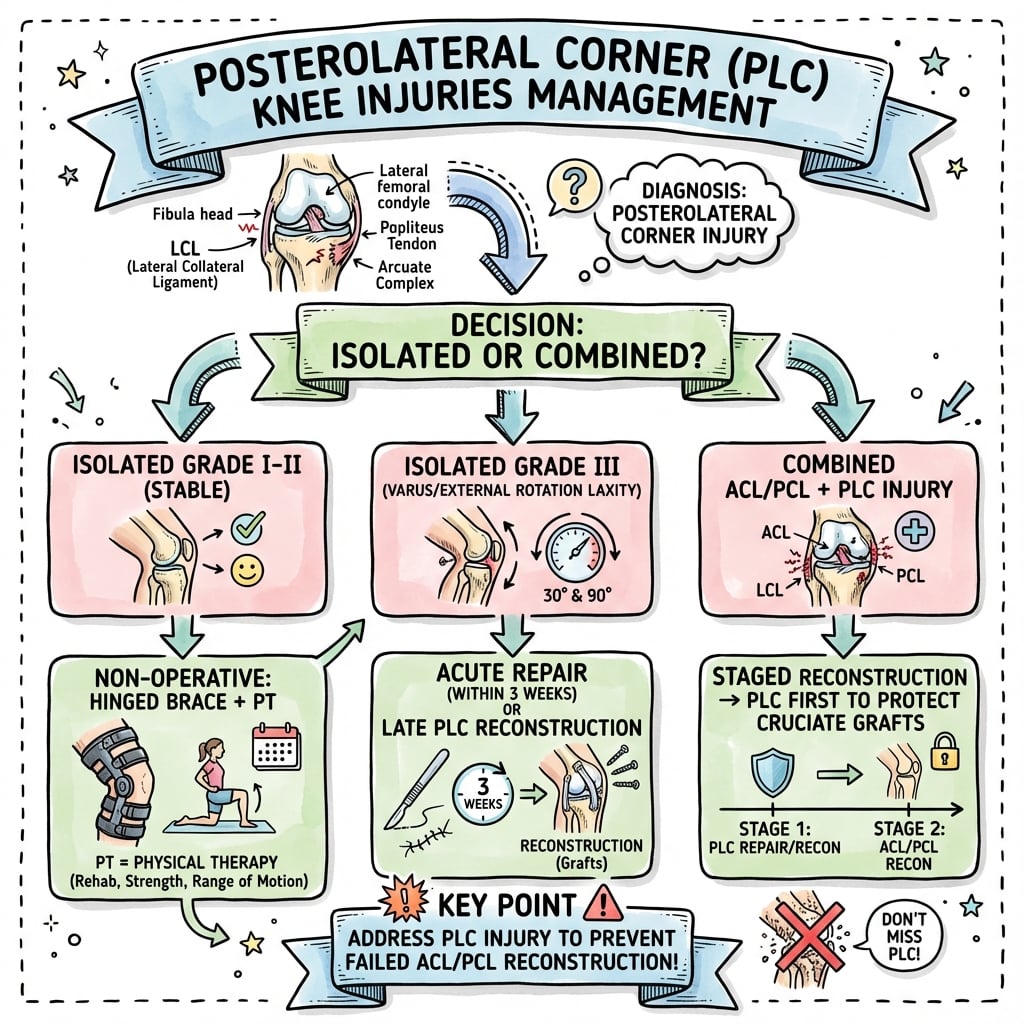
PLC Injury Management
Treatment Pathway
Document neurovascular status. MRI for full injury pattern. Assess alignment.
Limited evidence. Bracing, rehabilitation. Monitor for progressive laxity.
Anatomic reconstruction preferred. Address all injured structures. Early surgery (within 3 weeks) if combined.
Assess for varus thrust. May need HTO before or with PLC reconstruction.
Surgical Technique
Anatomic PLC Reconstruction
Achilles allograft with bone block, or split semitendinosus.
- Femoral: At FCL and popliteus origins (separate tunnels)
- Fibular: At FCL insertion
- Reconstruct FCL from femur to fibula
- Reconstruct popliteus and popliteofibular ligament
- Graft crosses from fibula to tibial sulcus
Anatomic reconstruction restores both varus and rotational stability.
Common peroneal nerve at risk during PLC reconstruction. Meticulous dissection required. Identify and protect nerve throughout. May be scarred/displaced in chronic cases.
Complications
- Cause
- Traction, direct
- Prevention
- Identify and protect
- Management
- Observation, EMG, may recover
- Cause
- Technical error, missed structure
- Prevention
- Anatomic reconstruction
- Management
- Revision
- Cause
- Scarring, immobilization
- Prevention
- Early ROM
- Management
- Physiotherapy, MUA
- Cause
- Missed varus alignment
- Prevention
- Correct alignment
- Management
- HTO then revision
Peroneal nerve injury occurs in 20%+ of PLC injuries. Complete lesions have poor recovery. Incomplete lesions may recover over 6-12 months. Consider nerve exploration/grafting if no recovery at 3-6 months.
Postoperative Care
PLC Reconstruction Rehabilitation
Brace locked in extension. Non-weight bearing. Avoid external rotation.
Progressive flexion. Partial weight bearing. Quad strengthening.
Full ROM. Weight bearing progression. Closed chain exercises.
Sport-specific preparation. Pool running. Proprioception.
Functional testing. Full sport when strength and stability restored.
Avoid external rotation stress early - this stresses the PLC reconstruction. Avoid varus stress. Progress slower if combined with other reconstructions.
Outcomes and Prognosis
Outcome Factors
Anatomic reconstruction, early surgery, all structures addressed, alignment corrected.
Isolated repair, delayed surgery, missed varus alignment, incomplete reconstruction, peroneal nerve injury.
Long-Term
Progressive varus deformity, lateral compartment OA, cruciate graft failure.
Good return to activity, stable knee, preserved function.
Guidelines, Registries & Global Practice
- PLC injury accounts for roughly 16% of knee ligament injuries
- Up to 60-70% occur with a cruciate injury (rarely truly isolated)
- Common peroneal nerve involvement in 15-25% of cases
- Typical patient is young and male (mean age mid-20s to early 30s in published series)
- High-energy mechanisms predominate: road traffic trauma, contact sport, knee dislocation
- No single dedicated international society guideline exists; practice is driven by expert consensus and series
- ESSKA / European consensus: reconstruct rather than repair grade III injuries; address all structures anatomically
- AANA / AOSSM (North America): anatomic reconstruction is the reference standard for chronic and most acute grade III injuries
- AO / multiligament-knee principles: ankle-brachial index in suspected dislocation, early surgery, reconstruct the PLC/FCL
- Broad agreement that missed varus malalignment must be corrected before or with reconstruction
- European consensus (ESSKA)
- Anatomic reconstruction
- North American (AOSSM/AANA)
- Anatomic reconstruction
- Multiligament / AO principles
- Reconstruct PLC/FCL, not repair alone
- European consensus (ESSKA)
- Selective (good bony avulsion)
- North American (AOSSM/AANA)
- Selective; reconstruction favoured
- Multiligament / AO principles
- Repair carries higher failure
- European consensus (ESSKA)
- Early (within ~3 weeks)
- North American (AOSSM/AANA)
- Early for combined injuries
- Multiligament / AO principles
- Early after vascular clearance
- European consensus (ESSKA)
- Correct (staged or combined)
- North American (AOSSM/AANA)
- Correct before/with reconstruction
- Multiligament / AO principles
- Realign to protect the graft
- National knee-ligament registries (e.g. Scandinavian and UK datasets) capture mainly ACL; isolated PLC is under-represented, so high-quality outcome data come from specialist series
- Allograft is widely used in North America; many European and resource-limited settings rely on autograft (hamstring, peroneus longus, quadriceps) due to allograft cost and availability
- MRI and stress radiography availability shape how confidently PLC is diagnosed pre-operatively
- High-resource: anatomic multi-tunnel reconstruction, intra-operative fluoroscopy, allograft, structured bracing and physiotherapy
- Limited-resource: autograft, fibular-based (Larson-type) or hybrid techniques, greater reliance on clinical examination and plain films
- Universal priorities everywhere: document the peroneal nerve, exclude vascular injury in dislocations, and never miss the PLC alongside a cruciate tear
PLC injuries are high-yield viva topics. Know the dial test interpretation, arcuate sign significance, and why reconstruction is preferred. Be prepared to discuss combined injuries and the importance of addressing alignment.
Controversies and Areas of Uncertainty
The LaPrade anatomic two-graft technique reconstructs FCL, popliteus and popliteofibular ligament. Fibular-based (Larson) techniques are simpler and reconstruct FCL and popliteofibular ligament only. Anatomic methods better restore rotation biomechanically, but high-level comparative clinical data are limited and many surgeons obtain good results with a hybrid approach.
Reconstruction is more durable overall (repair failure around 37% vs 9%). However, a good acute bony avulsion with healthy tissue can be primarily fixed. The threshold for choosing repair over reconstruction in the acute setting remains debated.
With genu varus, some advocate osteotomy first (a proportion then avoid ligament surgery), others perform combined realignment and reconstruction. Optimal sequencing, especially in multiligament knees, is unresolved.
Allograft versus autograft, optimal tensioning angle, and whether early peroneal nerve exploration changes outcomes are all areas without consensus. Complete peroneal lesions still carry a poor prognosis regardless of approach.
MCQ Practice Points
Q: Dial test positive at 30 degrees only vs 30 and 90 degrees? A: 30 degrees only = isolated PLC. 30 and 90 degrees = combined PCL + PLC. At 90 degrees, intact PCL prevents external rotation.
Q: What are the primary functions of the PLC? A: Varus restraint (FCL primary) and external rotation restraint (popliteus primary). Also resists hyperextension.
Q: What is the arcuate sign? A: Avulsion fracture of fibular head on X-ray. Pathognomonic for PLC injury. Indicates avulsion of FCL/biceps attachment.
Q: Why is reconstruction preferred over repair for PLC? A: Repair has 37% failure rate vs 9% for reconstruction. Reconstruction anatomically restores all structures.
Q: What nerve is at risk with PLC injuries? A: Common peroneal nerve - 20%+ injury rate. Check ankle dorsiflexion and lateral leg sensation. Document preoperatively.
Q: Why is varus alignment important in PLC injuries? A: Varus increases load on PLC. Must correct with HTO before or with reconstruction, or reconstruction will fail.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old motorcyclist presents after an MVC. He has a swollen knee. Posterior drawer shows Grade III laxity. Dial test shows 20 degrees increased external rotation at both 30 and 90 degrees compared to the opposite side. He has ankle dorsiflexion weakness. What is your assessment and management?”
“A 35-year-old presents with lateral knee instability for 2 years after a rugby injury. He walks with a noticeable varus thrust. Dial test shows 15 degrees increased external rotation at 30 degrees, symmetric at 90 degrees. X-rays show varus alignment (mechanical axis 5 degrees varus). What is your approach?”
“A 22-year-old presents after a knee hyperextension injury during soccer. X-ray shows a small avulsion fracture of the fibular head. He has tenderness posterolaterally. Dial test is positive at 30 degrees only. What is your management?”
PLC Structures (FAP)
- FCL: Primary varus restraint
- Arcuate complex: Posterolateral capsule
- Popliteus complex: External rotation restraint
- Popliteofibular ligament connects them
Dial Test Critical
- Test at 30 AND 90 degrees
- Positive at 30 only = isolated PLC
- Positive at 30 AND 90 = combined PCL + PLC
- Greater than 10 degree asymmetry = positive
Key Findings
- Arcuate sign: Fibular head avulsion = PLC
- Varus thrust gait: Chronic PLC deficiency
- Peroneal nerve injury: 20%+ cases
- Combined injuries most common
Treatment Principles
- Reconstruction superior to repair (37% vs 9% failure)
- LaPrade anatomic technique gold standard
- Early surgery (within 3 weeks) preferred
- Address varus alignment or reconstruction fails
Exam Pearls
- Commonly missed injury - high suspicion
- Always check with PCL and ACL injuries
- Document peroneal nerve status
- Early surgery prevents contracture
Evidence Base and Key Studies
Quantitative Posterolateral Attachment Anatomy
- Cadaveric study (10 fresh-frozen knees) mapping the FCL, popliteus tendon, popliteofibular ligament and lateral gastrocnemius attachments
- FCL femoral attachment averaged 1.4 mm proximal and 3.1 mm posterior to the lateral epicondyle; fibular attachment 8.2 mm posterior to the anterior fibular head
- Popliteus femoral attachment lies in the proximal-anterior fifth of the popliteal sulcus, always anterior to the FCL (mean separation 18.5 mm)
- Popliteofibular ligament had constant anterior and posterior divisions at the fibular styloid
Anatomic PLC Reconstruction (Biomechanical Validation)
- In-vitro biomechanical study in 10 cadavers describing a 2-graft technique reconstructing the FCL, popliteus tendon and popliteofibular ligament
- Restored varus stability versus the sectioned (grade III) state at 0, 30, 60 and 90 degrees of flexion
- Restored external rotation control, with no significant difference from the intact knee at any flexion angle
- Became the reference anatomic reconstruction technique