Non-Hodgkin Lymphoma of Bone | Permeative Round Cell Tumour | Chemo-Sensitive
- Bone lymphoma is treated medically, not by wide surgical resection - chemotherapy (R-CHOP) is the backbone, surgery is for biopsy, fracture fixation or cord decompression only
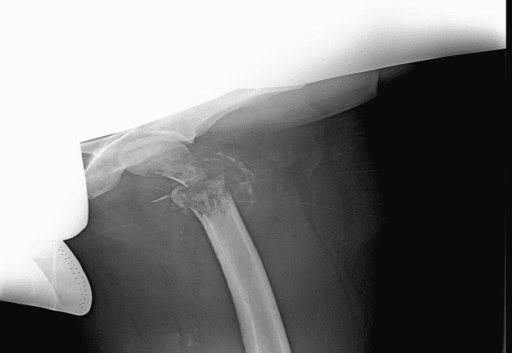
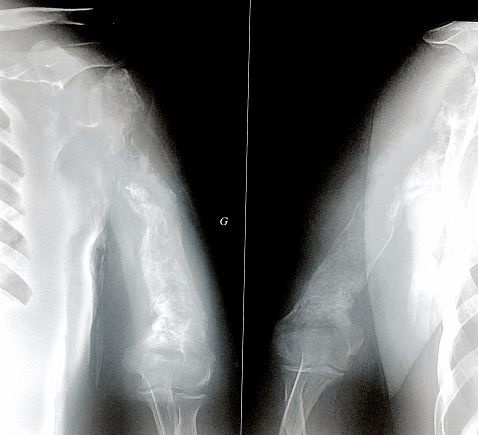
- Classic radiograph: a permeative, moth-eaten metadiaphyseal lesion with a large soft-tissue mass but surprisingly little cortical destruction
- Over 80% are diffuse large B-cell lymphoma (DLBCL) - a high-grade non-Hodgkin lymphoma
- Diagnosis needs a generous core or open biopsy sent fresh for flow cytometry and immunohistochemistry - small needle samples often non-diagnostic
- Prognosis is far better than osteosarcoma or Ewing sarcoma - around 60-70% survive 5 years, driven by age and International Prognostic Index
- “The patient who looks 'too well' for the size of the bone lesion - good performance status with a big destructive tumour - think lymphoma
- “MRI shows extensive marrow and soft-tissue disease that is out of proportion to the modest cortical break on X-ray
- “Always tell the lab you suspect lymphoma so fresh tissue goes for flow cytometry, not just formalin
- “Staging is by Ann Arbor and IPI (a lymphoma framework), not only Enneking - this is a haematological malignancy that happens to live in bone
Do NOT perform a wide en-bloc resection. Bone lymphoma is exquisitely chemosensitive. The orthopaedic role is biopsy, stabilising an impending/actual fracture, and decompressing the cord - definitive treatment is R-CHOP chemotherapy.
Send fresh tissue for flow cytometry and immunohistochemistry. A crushed or formalin-only small needle sample is often non-diagnostic. Take a generous core/open sample and warn the pathologist that lymphoma is on the differential.
Large soft-tissue mass, little cortical destruction. A permeative metadiaphyseal lesion that looks modest on X-ray but huge on MRI, in a patient over 30, is highly suggestive of lymphoma.
Vertebral lymphoma can cause acute cord compression. Give corticosteroids, get urgent MRI, and decide between urgent decompression/stabilisation versus radiotherapy with the haematology and spinal teams.
BONEDefining True Primary Bone Lymphoma
Hook:If it does not satisfy all of BONE, it is secondary skeletal lymphoma - a different staging and treatment conversation.
APLESPrognostic Drivers (International Prognostic Index)
Hook:APLES are the five IPI factors - they predict survival far better than the bone site or whether the patient fractured.
Overview and Epidemiology
What Primary Bone Lymphoma Is
Primary bone lymphoma (PBL) is a malignant lymphoma that arises within bone, with no evidence of nodal or other extraskeletal disease at presentation. It is a non-Hodgkin lymphoma that happens to live in the skeleton, and the overwhelming majority - over 80% - are diffuse large B-cell lymphoma (DLBCL), a high-grade B-cell malignancy. Because it is a haematological cancer rather than a true bone-forming tumour, it is staged and treated largely with the lymphoma toolkit (Ann Arbor stage, International Prognostic Index, chemotherapy), while the orthopaedic surgeon manages biopsy and the mechanical consequences in bone.
PBL sits in the differential of an aggressive, permeative round cell lesion in an adult - alongside Ewing sarcoma, metastatic carcinoma, multiple myeloma and infection. Distinguishing it matters enormously because the treatment and prognosis are completely different.
Epidemiology
- Accounts for less than 5% of all primary bone tumours
- Roughly 3-7% of extranodal lymphomas
- A genuinely rare tumour - most data come from registry and single-centre series
- Adults, with a broad peak around 45-60 years
- Older than the typical Ewing sarcoma patient
- Slight male predominance in most series; no strong sex preponderance in large registry data
- Long-bone metadiaphysis (femur most common), plus pelvis and spine
- Appendicular and craniofacial sites carry a survival advantage over axial sites
- Can be single-bone or polyostotic while remaining bone-limited
According to PubMed, the largest population-based analysis (SEER, 2558 patients) confirmed that DLBCL is the dominant histology, that axial-skeleton primaries do worse than appendicular or craniofacial primaries, and that chemotherapy is an independent favourable prognostic factor (DOI).
Pathophysiology and Histology
Cell of Origin and Pathology
Primary bone lymphoma is a clonal proliferation of malignant lymphocytes within the marrow space. The dominant subtype, diffuse large B-cell lymphoma, is composed of sheets of large, atypical lymphoid cells (centroblast-like or immunoblast-like) that diffusely efface the marrow and permeate between bony trabeculae rather than forming bone or cartilage. This permeative growth - infiltrating through marrow and Haversian canals - explains the imaging signature of extensive marrow and soft-tissue disease with relatively preserved cortex.
Key Histological and Immunophenotypic Features
- Diffuse sheets of large atypical lymphoid cells
- Marrow effacement and permeation between trabeculae
- Frequent crush artefact - emphasising the need for careful, generous biopsy
- Reactive fibrosis can make small samples look non-specific
- B-cell markers: CD20, CD19, CD79a, PAX5 in DLBCL
- High proliferation index (Ki-67)
- Cell-of-origin profiling (germinal-centre vs activated B-cell) by Hans algorithm
- Flow cytometry on fresh tissue confirms clonality rapidly
WHO Classification Context
Within the WHO classification of haematolymphoid tumours, primary bone lymphoma is not a separate entity but a primary extranodal presentation of an established lymphoma type - most often diffuse large B-cell lymphoma, with smaller numbers of follicular, marginal zone, T-cell rich B-cell, anaplastic large cell and (in children) lymphoblastic lymphomas. The histological subtype, defined by morphology plus immunophenotype, drives treatment more than the fact that the tumour is in bone.
Lymphoid cells are fragile and crush easily. A small core that is crushed, or one sent only in formalin, frequently returns as "small round blue cell tumour, non-diagnostic." A generous core or open biopsy, with fresh tissue split off for flow cytometry and adequate material for immunohistochemistry, gives the pathologist what they need to subtype the lymphoma and avoid a repeat procedure.
Classification and Staging

Frameworks You Must Be Able to Apply
Primary bone lymphoma is staged with two parallel systems: the surgical/musculoskeletal frameworks (Enneking, AJCC) that you use for any bone tumour, and the lymphoma-specific Ann Arbor stage with the International Prognostic Index, which actually drive treatment and prognosis.

Ann Arbor staging (adapted for extranodal/bone disease) is the working staging system:
- Stage IE - single extranodal (bone) site only
- Stage IIE - bone site plus regional nodes on the same side of the diaphragm
- Stage IIIE - involvement on both sides of the diaphragm
- Stage IV - disseminated/multifocal extranodal disease
The International Prognostic Index (IPI) then risk-stratifies and predicts survival using five factors (remember APLES): Age over 60, poor Performance status, elevated LDH, more than one Extranodal site, advanced Stage. Age-adjusted IPI is the single strongest predictor of long-term survival in bone DLBCL.
- Lymphoma Systems (Ann Arbor + IPI)
- Define extent of lymphoma and predict survival
- Surgical Systems (Enneking / AJCC)
- Guide surgical margins for bone tumours
- Lymphoma Systems (Ann Arbor + IPI)
- Yes - stage and IPI determine number of cycles and need for radiotherapy
- Surgical Systems (Enneking / AJCC)
- No
- Lymphoma Systems (Ann Arbor + IPI)
- No - resection is not the treatment
- Surgical Systems (Enneking / AJCC)
- Would normally drive wide resection in a sarcoma, but NOT here
- Lymphoma Systems (Ann Arbor + IPI)
- Age-adjusted IPI
- Surgical Systems (Enneking / AJCC)
- Grade and compartment status (less relevant for lymphoma)
Clinical Presentation
How Patients Present
The commonest story is localised bone pain, often present for weeks to months and frequently worse at night, in a patient who is otherwise relatively well. A palpable mass or soft-tissue swelling may be present. A minority present acutely with a pathological fracture or, when the spine is involved, with spinal cord compression.
- Bone pain - often persistent and night pain
- Palpable mass / swelling over the affected bone
- Pathological fracture in a minority
- Reduced function of the adjacent joint
- Back pain with vertebral involvement
- Radiculopathy from nerve root compression
- Spinal cord compression - an emergency
- Half of spinal cases in some series present with cord compression
- Fever, drenching night sweats, weight loss (the lymphoma B-symptoms)
- Often absent in truly bone-limited disease
- Their presence should prompt a search for systemic spread
A recurring exam and clinical clue is the patient whose general condition seems too good for the size and aggressiveness of the bone lesion. A large permeative destructive tumour in a comfortable, well-looking adult should move lymphoma up your differential, ahead of osteosarcoma or metastatic carcinoma.
Investigations and Imaging
Imaging Findings
According to PubMed, the classic radiographic-MRI description is a solitary permeative metadiaphyseal lesion with a layered periosteal reaction and a soft-tissue mass, associated with surprisingly little cortical destruction, in a patient older than 30 - a pattern highly suggestive of bone lymphoma (DOI). Because the lesion can look near-normal on plain films, a second modality (MRI or bone scintigraphy) is essential.
- What It Shows
- Permeative/moth-eaten metadiaphyseal lytic lesion, often with subtle layered periosteal reaction
- Why It Matters
- First test, but can underestimate disease - a near-normal film does not exclude lymphoma
- What It Shows
- Extensive marrow infiltration and a large soft-tissue mass out of proportion to cortical break
- Why It Matters
- Best for local extent, marrow involvement, soft-tissue mass and cord compression; guides biopsy
- What It Shows
- Cortical detail and degree of bony destruction; helps surgical/biopsy planning
- Why It Matters
- Clarifies cortical integrity and fracture risk
- What It Shows
- Whole-body metabolic staging and response assessment
- Why It Matters
- Stages the lymphoma and assesses chemotherapy response - but bone uptake can persist after remission, so interpret with caution
- What It Shows
- Increased uptake at affected sites
- Why It Matters
- Sensitive second modality when MRI is unavailable; non-specific
Interpret post-treatment PET-CT of bone with caution. Bone lesions can retain FDG uptake even after the lymphoma has gone into remission. A persistently "hot" bone lesion on follow-up PET does not automatically mean residual disease - correlate with biopsy, MRI and the clinical picture before changing treatment.
Lymphoma PET response (the Lugano framework) is reported with the Deauville 5-point score, comparing lesion uptake to two reference organs - the mediastinal blood pool and the liver: 1 = no uptake above background; 2 = uptake at or below mediastinum; 3 = above mediastinum but at or below liver; 4 = moderately above liver; 5 = markedly above liver and/or new lesions. Scores 1-3 are generally a complete metabolic response, while 4-5 suggest inadequate response/residual disease - but in bone this must be read against the caveat above, because bone can stay FDG-avid after true remission.

LYMPHOMARecognising Primary Bone Lymphoma on Imaging
Hook:Spell LYMPHOMA when an adult has a big permeative bone lesion but looks surprisingly well - the imaging-clinical mismatch is the giveaway.
Biopsy Principles
Getting the Diagnosis Right
Biopsy is the single most important orthopaedic step, and it is easy to get wrong in lymphoma. The tumour is chemosensitive and rarely resected, so the biopsy is not just a staging step - it is essentially the only tissue you may take.
- Take a generous core or open biopsy
- Split off fresh tissue for flow cytometry before fixation
- Warn the pathologist that lymphoma is on the differential
- Place the biopsy tract so it can be excised if later surgery is needed, ideally planned with the operating tumour surgeon
- Send adequate material for immunohistochemistry and molecular studies
- Tiny crushed needle samples that return non-diagnostic
- Formalin-only handling with no fresh sample for flow cytometry
- Transverse incisions or poorly placed tracts that compromise later surgery
- Proceeding to wide resection before a tissue diagnosis is confirmed
Never perform a definitive resection of a suspected bone lymphoma before histological diagnosis. Wide en-bloc resection is the correct operation for osteosarcoma or chondrosarcoma - but for lymphoma it is unnecessary morbidity, because chemotherapy is the definitive treatment. Confirm the diagnosis first, then treat medically.
Differential Diagnosis of the Permeative Round-Cell Lesion
The aggressive permeative bone lesion in an adult has a short, high-stakes differential, and the distinction is ultimately made on the immunohistochemistry panel - which is exactly why the biopsy must be generous and the right stains requested.
- Typical age
- 45-60 years
- Imaging clue
- Permeative metadiaphyseal lesion, big soft-tissue mass, little cortical break; patient 'too well'
- Histology / immunohistochemistry
- Large atypical lymphoid cells; CD20+, CD45/LCA+, PAX5+, CD79a+, high Ki-67
- Typical age
- Under 20-30 years
- Imaging clue
- Diaphyseal permeative lesion, lamellated 'onion-skin' periosteal reaction
- Histology / immunohistochemistry
- Small round blue cells; CD99 (membranous)+, FLI-1/NKX2.2+, EWSR1-FLI1 t(11;22)
- Typical age
- Over 50 years
- Imaging clue
- Lytic (or blastic) lesion; known primary or multiple lesions
- Histology / immunohistochemistry
- Epithelial cells; cytokeratin (AE1/AE3)+, EMA+; site-specific markers
- Typical age
- Over 50 years
- Imaging clue
- Punched-out lytic lesion(s); marrow disease
- Histology / immunohistochemistry
- Plasma cells; CD138+, CD38+, monoclonal kappa/lambda light-chain restriction
- Typical age
- Any age
- Imaging clue
- Permeative lytic with periosteal reaction - a classic radiographic mimic
- Histology / immunohistochemistry
- Mixed acute/chronic inflammation; organisms on culture (always send microbiology)
When a "small/large round blue cell tumour" report comes back, the discriminating immunostains are: lymphoma = CD20/CD45(LCA)/PAX5, Ewing = CD99/FLI-1 (and the EWSR1 translocation), carcinoma = cytokeratin/EMA, myeloma/plasmacytoma = CD138 with light-chain restriction. Always send microbiology as well, because osteomyelitis is the great radiographic imitator of a permeative tumour.
Management Algorithm
Principles
Treatment is systemic chemotherapy first, with radiotherapy as consolidation in selected cases, and surgery reserved for biopsy and mechanical problems. The standard regimen is R-CHOP - rituximab plus cyclophosphamide, doxorubicin, vincristine and prednisone - reflecting that most cases are DLBCL.
Chemotherapy is the backbone of treatment.
- R-CHOP (rituximab-CHOP) is standard for DLBCL bone lymphoma
- According to PubMed, adding rituximab to CHOP markedly improved 3-year progression-free survival (88% with R-CHOP vs 52% with CHOP-like therapy) in primary bone lymphoma (DOI)
- Number of cycles is guided by Ann Arbor stage, IPI and PET response
- CNS prophylaxis is considered in high-risk disease, as bone/extranodal involvement is itself a risk factor for CNS relapse
Managing the Bone Itself
- Action
- Biopsy, refer to haematology, start chemotherapy
- Rationale
- Chemosensitive disease - bone often heals with systemic treatment
- Action
- Prophylactic fixation (often intramedullary) around chemotherapy
- Rationale
- Prevents catastrophic fracture; preserves function during treatment
- Action
- Stabilise (fixation); resection rarely needed
- Rationale
- Lymphoma bone heals well with chemotherapy once stabilised
- Action
- Steroids, urgent MRI, decompress/stabilise or radiotherapy
- Rationale
- Neurological emergency - protect cord function
Surgical Technique - Biopsy and Stabilisation
Operative Principles
Although bone lymphoma is a medical disease, the orthopaedic surgeon performs two operations that must be done well: the diagnostic biopsy and fracture stabilisation.
Diagnostic biopsy steps:
- Plan the approach with the surgeon who would do any later definitive surgery, and place the tract so it can be excised later if needed
- Use a longitudinal incision in line with the limb, avoiding contamination of multiple compartments and neurovascular structures
- Take a generous core or open sample of representative tumour, avoiding necrotic centre
- Split off fresh tissue for flow cytometry and send adequate material for histology, immunohistochemistry and microbiology (infection is a key differential)
- Achieve meticulous haemostasis - a haematoma spreads tumour through tissue planes
Complications
Disease and Treatment Complications
- Pathological fracture of the affected bone
- Spinal cord or nerve root compression
- CNS relapse - bone/extranodal involvement is a recognised risk factor
- Relapsed or refractory lymphoma
- Chemotherapy toxicity - myelosuppression, neutropenic sepsis, cardiotoxicity (doxorubicin), neuropathy (vincristine)
- Radiotherapy late effects - including second malignancy and growth disturbance in the young
- Surgical complications - infection, fixation failure, wound problems compounded by immunosuppression
- Tumour lysis syndrome with rapid response to chemotherapy
According to PubMed, in diffuse large B-cell lymphoma, bone involvement is an independent risk factor for central nervous system relapse (hazard ratio around 4), and rituximab reduces overall CNS relapse rates (DOI). This is why CNS-directed risk assessment and, in selected cases, prophylaxis are part of the haematology plan.
Postoperative Care and Rehabilitation
Recovery and Follow-Up
Because treatment is led by chemotherapy, "postoperative" care after biopsy or fixation runs in parallel with systemic therapy.
- Wound surveillance, especially during chemotherapy-related immunosuppression
- Early mobilisation after stabilisation to preserve function
- Coordinate analgesia with the oncology team
- Monitor for neutropenic sepsis and treat promptly
- Protect the operated/affected limb until bone consolidates
- PET-CT response assessment guides ongoing treatment
- Regular clinical and imaging follow-up for relapse
- Watch for late chemo/radiotherapy effects
- Functional rehabilitation of the affected limb or spine
Outcomes and Prognosis
How Patients Do
Primary bone lymphoma has a substantially better prognosis than osteosarcoma or Ewing sarcoma of bone. According to PubMed, the large SEER analysis reported 5- and 10-year overall survival of approximately 66% and 54% (DOI), and the British Columbia cohort showed 5- and 10-year overall survival of 62% and 41% for bone DLBCL, rising to a 5-year survival of 90% in younger patients with a good IPI (DOI).
- Favourable
- Younger (under 60)
- Adverse
- Older (over 60)
- Favourable
- Low IPI / age-adjusted IPI
- Adverse
- High IPI
- Favourable
- Limited (IE / IIE)
- Adverse
- Advanced (III-IV)
- Favourable
- Rituximab-containing chemotherapy (R-CHOP)
- Adverse
- Chemotherapy without rituximab
- Favourable
- Appendicular / craniofacial
- Adverse
- Axial skeleton
A useful exam point: in the British Columbia series, neither primary site nor pathological fracture at presentation independently affected overall survival - outcome was driven by age and IPI. Reassure that a fracture at presentation, properly stabilised, does not by itself worsen the lymphoma prognosis.
Guidelines, Registries & Global Practice
Global Picture
Primary bone lymphoma is rare, so practice rests on registry and cohort data rather than randomised trials specific to bone. The principles below are consistent across major lymphoma and bone-tumour frameworks worldwide.
- Region
- United States
- Contribution to Global Practice
- Largest dataset (2558 patients): DLBCL dominant, axial sites worse, chemotherapy independently improves survival
- Region
- Canada
- Contribution to Global Practice
- Established R-CHOP benefit and age/IPI-based prognostic groups for bone DLBCL
- Region
- France / Europe
- Contribution to Global Practice
- Supports immunochemotherapy with radiotherapy consolidation and caution interpreting post-treatment bone PET
- Region
- International
- Contribution to Global Practice
- Defines the histological subtypes (DLBCL and others) that drive treatment
- Region
- International
- Contribution to Global Practice
- Endorse R-CHOP-based therapy for DLBCL, with radiotherapy and CNS risk assessment as appropriate
Practice Points That Travel
- Multidisciplinary care (haematology, radiation oncology, orthopaedic/spinal surgery, pathology, radiology) is standard everywhere.
- R-CHOP is the global backbone for DLBCL bone lymphoma, with rituximab availability being the main source of practice variation in lower-resource settings.
- Surgery is supportive - biopsy and stabilisation - across all settings; wide resection is not standard anywhere.
- Prognosis is favourable relative to other malignant bone tumours, a message that holds across registries.
MCQ and Exam Practice Points
High-Yield Points to Drill
- Bone lymphoma is treated by chemotherapy (R-CHOP), not wide resection
- Over 80% are diffuse large B-cell lymphoma
- Classic imaging: permeative metadiaphyseal lesion, big soft-tissue mass, little cortical destruction
- Generous biopsy with fresh tissue for flow cytometry
- Choosing wide en-bloc resection (correct for osteosarcoma, wrong here)
- Forgetting to send fresh tissue for flow cytometry
- Ignoring the better prognosis versus other malignant bone tumours
- Over-calling residual disease on post-treatment bone PET
Primary bone lymphoma is a chemosensitive, DLBCL-dominant non-Hodgkin lymphoma of the skeleton: recognise the permeative metadiaphyseal lesion with a disproportionate soft-tissue mass, biopsy it properly, and treat with R-CHOP rather than resection.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man presents with 3 months of right thigh pain, worse at night. Radiographs show a permeative, moth-eaten lesion in the proximal femoral metadiaphysis with a subtle layered periosteal reaction. He looks remarkably well. How would you approach this?”
“A 62-year-old woman presents with progressive back pain and new lower-limb weakness. MRI shows a vertebral body lesion with an epidural soft-tissue mass compressing the spinal cord. Biopsy confirms diffuse large B-cell lymphoma with no disease elsewhere. How do you manage this?”
Key Definition
- Malignant lymphoma arising in bone with no nodal or visceral disease at presentation
- Less than 5% of primary bone tumours; over 80% are diffuse large B-cell lymphoma
- A chemosensitive haematological malignancy, NOT a tumour treated by wide resection
Classic Imaging (Must Know)
- Permeative, moth-eaten metadiaphyseal lytic lesion (femur most common)
- Layered periosteal reaction; often subtle on plain film
- Large soft-tissue mass with surprisingly little cortical destruction
- MRI shows extensive marrow disease; always use a second modality
Diagnosis
- Generous core or open biopsy with FRESH tissue for flow cytometry
- Immunohistochemistry: CD20 and other B-cell markers in DLBCL
- Warn the pathologist that lymphoma is suspected
- Send material for microbiology - infection is a key differential
Staging and Prognosis
- Stage by Ann Arbor plus International Prognostic Index (APLES factors)
- Age-adjusted IPI is the strongest predictor of long-term survival
- 5-year overall survival roughly 60-70% - far better than osteosarcoma/Ewing
- Appendicular/craniofacial sites do better than axial; fracture does not independently worsen survival
Treatment
- R-CHOP chemotherapy is the backbone (DLBCL)
- Radiotherapy as consolidation for residual/bulky disease or after cord compression
- Surgery only for biopsy, impending/actual fracture, or cord decompression
- Relapsed/refractory: salvage chemo, autologous transplant, CAR T-cell therapy
Common Exam Traps
- Choosing wide resection (right for osteosarcoma, wrong for lymphoma)
- Sending only a tiny formalin-fixed sample - no flow cytometry
- Over-calling residual disease on post-treatment bone PET
- Forgetting CNS relapse risk in extranodal/bone DLBCL