Failed Index Surgery | Complex Osteotomies | High Complication Rate
Revision Indications
Critical Must-Knows
- Pseudarthrosis most common at lumbosacral junction and osteotomy sites
- PJK criteria: greater than 10-15 degree kyphosis at UIV segment
- PSO corrects approximately 30 degrees per level
- SPO corrects approximately 10-15 degrees per level
- Medical optimization critical - frailty assessment mandatory
Clinical Pearls
- "Identify failure mechanism BEFORE planning revision strategy
- "Know contraindications - greater than 3 major comorbidities, severe osteoporosis, frailty
- "Describe staged revision protocol for deep infection
- "PSO requires greater anterior column support than SPO
Revision Deformity Surgery
Clinical Warning
High-Risk Surgery: Revision deformity surgery has complication rates of 40-60%. Examiners will assess your understanding of failure mechanisms, patient selection, and when NOT to operate. Medical frailty and severe osteoporosis may be absolute contraindications.
At a Glance
Essential Mnemonics
IMAGINGIMAGING Protocol for Revision Assessment
| I | Identify Failure mechanism (pseudarthrosis, PJK, alignment) |
| M | Measure Sagittal parameters (SVA, PI-LL, PT) |
| A | Assess Hardware (screws, rods, connectors) |
| G | Gold standard CT For fusion evaluation |
| I | Infection ruled out CRP, ESR, MRI if needed |
| N | Nuclear medicine SPECT-CT if CT equivocal |
| G | Get bone density DEXA for osteoporosis |
| I | Identify Failure mechanism (pseudarthrosis, PJK, alignment) | G | Gold standard CT For fusion evaluation | G | Get bone density DEXA for osteoporosis |
| M | Measure Sagittal parameters (SVA, PI-LL, PT) | I | Infection ruled out CRP, ESR, MRI if needed | ||
| A | Assess Hardware (screws, rods, connectors) | N | Nuclear medicine SPECT-CT if CT equivocal |
Hook:Systematic imaging protocol ensures no failure mechanism is missed
Overview
Revision deformity surgery represents one of the most challenging domains in adult spine surgery, with documented complication rates of 40-60% across major series. The incidence of revision surgery has increased with greater numbers of primary adult deformity corrections being performed, improved patient longevity, and heightened expectations for quality of life.
Epidemiology (global):
- Revision rates after primary adult deformity surgery range from 15-30% at 5 years across international multicentre series (ISSG, European Spine Study Group)
- Mean time to revision is 2-3 years, though can range from months to decades
- Patient age at revision typically 55-75 years (older than primary surgery cohort)
- Rising volume worldwide reflects ageing populations, more index deformity corrections, and higher patient expectations
Primary Indications for Revision:
- Pseudarthrosis (35-40%): Most common indication, particularly at lumbosacral junction
- Proximal junctional kyphosis (25-30%): Increasingly recognized complication
- Sagittal imbalance (20-25%): Undercorrection or loss of correction
- Infection (10-15%): May present acutely or as late chronic infection
Practice Context: Complex revision deformity surgery is concentrated worldwide at tertiary spine centres with multidisciplinary support, advanced neuromonitoring, and intensive care. International registries and study groups (Scoliosis Research Society Morbidity & Mortality database, International Spine Study Group, European Spine Study Group) provide the benchmark complication and revision-rate data used for counselling.
Pathophysiology
Pathophysiology of Deformity Recurrence
Mechanical Failure Mechanisms:
-
Pseudarthrosis (35-40% of Revisions):
- Incomplete osseous bridging leads to ongoing motion
- Micromotion prevents bone healing
- Results in progressive deformity and hardware failure
- Most common at lumbosacral junction and three-column osteotomy sites
-
Proximal Junctional Kyphosis/Failure (25-30%):
- Acute angular kyphosis at UIV or UIV+1
- Caused by stress concentration at construct terminus
- Biomechanical mismatch between rigid construct and mobile spine
- Osteoporotic compression fractures at junctional vertebrae
-
Sagittal Imbalance (20-25%):
- Undercorrection at index surgery
- Loss of correction over time
- Progressive adjacent segment degeneration
- Leads to positive sagittal vertical axis (SVA greater than 50mm)
-
Distal Junctional Failure:
- Less common than PJK (approximately 5-10%)
- Typically at lumbosacral junction
- Inadequate sacropelvic fixation
- S1 screw pullout or rod fracture
Biological Failure Mechanisms:
Infection:
- Disrupts fusion biology
- Creates biofilm on implants
- Requires staged revision in most cases
- May present as persistent pain or delayed wound healing
Osteoporosis:
- Screw loosening and pullout
- Compression fractures at junctional vertebrae
- Impaired fusion biology
- Higher pseudarthrosis rates
Medical Comorbidities:
- Diabetes impairs wound healing and fusion
- Smoking profoundly inhibits fusion (3-5 fold increased pseudarthrosis)
- Obesity increases mechanical stress on construct
- Malnutrition impairs healing
Anatomical Considerations in Revision Surgery
Scar Tissue and Epidural Adhesions:
- Extensive scar from prior surgery
- Neural elements adherent to dura and bone
- Risk of durotomy increased (10-15% in revisions)
- Risk of nerve injury during dissection
Altered Anatomy:
- Facets and posterior elements may be removed
- Pedicles violated by prior screws
- Bone quality compromised by prior decortication
- Vascular anatomy distorted by scarring
Loss of Fixation Points:
- Previous screw trajectories limit new screw placement
- Osteoporotic bone from stress shielding
- May require alternative fixation (hooks, sublaminar wires, iliac screws)
Classification
Revision Complexity Classification (Kim et al.)
Revision Deformity Surgery Complexity Grading
| category | characteristics | surgicalRequirements | expectedORTime | complicationRisk | example |
|---|---|---|---|---|---|
| Grade 1 - Simple Revision | Focal pseudarthrosis, solid fusion elsewhere, no deformity progression | Limited exposure, no osteotomy, autograft supplementation | 3-5 hours | Low (15-25%) | Single-level pseudarthrosis at L4-L5 in otherwise solid construct |
| Grade 2 - Moderate Revision | Multi-level pseudarthrosis or PJK requiring extension, mild deformity | Extended exposure, may need SPO, autograft + BMP | 5-8 hours | Moderate (25-40%) | PJK requiring 2-3 level cranial extension with SPO |
| Grade 3 - Complex Revision | Major deformity progression, requires osteotomy (PSO), extensive hardware revision | Full revision, PSO or VCR, dual rods, iliac fixation | 8-12 hours | High (40-60%) | Flatback deformity with SVA 150mm requiring L3 PSO and full construct revision |
| Grade 4 - Ultra-Complex Revision | Multiple prior revisions, severe rigid deformity, infection, major comorbidities | Staged procedures, combined approaches, multi-level osteotomies | Greater than 12 hours or staged | Very High (60-80%) | Third revision for infected pseudarthrosis with severe fixed kyphosis requiring VCR |
Etiology-Based Classification
Mechanical Failures:
- Type A: Pseudarthrosis (most common)
- Type B: Proximal junctional failure
- Type C: Distal junctional failure
- Type D: Hardware failure (rod fracture, screw breakage)
Alignment Failures:
- Type E: Sagittal imbalance (positive SVA)
- Type F: Coronal imbalance (trunk shift)
- Type G: Combined sagittal and coronal imbalance
Biological Failures:
- Type H: Infection (acute or chronic)
- Type I: Implant-related complications (prominence, pain)
Combined Failures:
- Type J: Multiple concurrent failure mechanisms (common in revisions)
Proximal Junctional Kyphosis (PJK) Classification
Hart et al. Classification:
- Type 1: Bony failure (compression fracture at UIV or UIV+1)
- Type 2: Ligamentous failure (disruption of PLL, supraspinous ligament)
- Type 3: Combined bony and ligamentous failure
Clinical Severity:
- Asymptomatic PJK: Greater than 10 degrees but no pain or dysfunction
- Symptomatic PJK: Pain limiting function
- PJF (Proximal Junctional Failure): Neurological deficit or severe deformity requiring revision
Clinical Presentation
History
Timeline of Symptoms:
- Early Recurrence (Less than 6 months): Suggests technical error, infection, or inadequate correction
- Intermediate (6 months to 2 years): Typical for pseudarthrosis or junctional failure
- Late (Greater than 2 years): Adjacent segment disease, late infection, hardware fatigue
Pain Patterns:
- Mechanical Back Pain: Worse with activity, better with rest (pseudarthrosis, hardware failure)
- Radicular Pain: Nerve root compression from deformity or foraminal stenosis
- Neurogenic Claudication: Spinal canal stenosis in deformity
- Constant Pain: Consider infection, especially if night pain
Functional Impact:
- Inability to stand upright (positive sagittal balance)
- Gait disturbance (stooped forward posture, compensatory knee flexion)
- Loss of horizontal gaze (cannot see ahead when walking)
- Decreased walking tolerance and distance
- Impact on activities of daily living
Red Flags:
- Fever, chills, night sweats (infection)
- Progressive neurological deficit
- Bladder or bowel dysfunction
- Rapid deformity progression
- Wound drainage or breakdown
Physical Examination
Global Alignment Assessment:
- Plumb Line Test: C7 plumb line to sacrum (SVA measurement)
- Coronal Balance: C7 plumb line to CSVL (coronal vertical axis)
- Compensatory Mechanisms: Knee flexion, ankle dorsiflexion, pelvic retroversion
- Horizontal Gaze: Can patient look straight ahead when standing?
Local Examination:
- Inspect incision for healing, drainage, erythema
- Palpate for tenderness, fluid collection, implant prominence
- Assess paraspinal muscle bulk (atrophy suggests denervation)
- Check for gibbus or step-off deformity
Neurological Examination:
- Motor strength (all myotomes L2-S2)
- Sensory examination (light touch, pinprick all dermatomes)
- Reflexes (knee, ankle, Babinski)
- Gait assessment (antalgic, Trendelenburg, foot drop)
- Upper motor neuron signs if myelopathy suspected
Functional Assessment:
- Walking distance and speed
- Sit-to-stand test
- Ability to maintain upright posture
- ODI (Oswestry Disability Index) or SRS-22 scores
Differential Diagnosis
Differential Diagnosis of Failed Deformity Surgery
| category | clinicalFeatures | imaging | labWork | management |
|---|---|---|---|---|
| Pseudarthrosis | Mechanical pain, pain-free interval then recurrence | CT shows less than 50% bridging bone, possible hardware failure | Normal inflammatory markers | Revision fusion with biologics |
| Infection | Persistent or recurrent pain, constitutional symptoms possible | MRI shows fluid collection, bone edema; loosening on radiographs | Elevated CRP/ESR, positive cultures on aspiration | Staged revision: explant, antibiotics, reconstruct |
| Adjacent Segment Disease | New radicular symptoms at unfused levels | Degeneration, stenosis, or instability adjacent to fusion | Normal | Conservative vs extension of fusion |
| Proximal Junctional Kyphosis | Progressive kyphotic deformity, pain at UIV region | Acute kyphosis at UIV/UIV+1, possible fracture | Normal, check DEXA for osteoporosis | Observation vs cranial extension with osteotomy |
| Chronic Pain Syndrome | Pain out of proportion to findings, multiple prior surgeries | May show solid fusion and normal alignment | Normal | Pain psychology, avoid further surgery |
Investigations
Radiographic Assessment
Standing Full-Length Spine Radiographs (Mandatory):
- AP and Lateral: Must be standing weight-bearing to assess true deformity
- Coronal Parameters: Cobb angle, coronal vertical axis (CVA), trunk shift
- Sagittal Parameters:
- SVA (sagittal vertical axis): C7 plumb line to posterior-superior S1 (normal less than 50mm)
- Pelvic incidence (PI): Fixed anatomic parameter
- Lumbar lordosis (LL): L1-S1 Cobb angle
- PI-LL mismatch: Normal within 10 degrees
- Pelvic tilt (PT): Compensatory mechanism (normal less than 20 degrees)
- Thoracic kyphosis (TK): T5-T12 Cobb angle
Hardware Assessment:
- Screw position and haloing (greater than 1mm lucency = loosening)
- Rod integrity (fractures, breakage)
- Connector and cross-link integrity
- Proximal and distal junctional vertebrae assessment
Flexion-Extension Views (Selected Cases):
- Assess for motion at suspected pseudarthrosis
- Greater than 5 degrees motion suggests non-union
- Limited value if hardware intact
Advanced Imaging
CT Scan with Metal Artifact Reduction:
- Gold Standard for Fusion Assessment
- Multiplanar reconstructions (sagittal, coronal, axial)
- Assess each interspace: bridging bone, bone quality
- Greater than 50% bridging bone = solid fusion
- Evaluate screw trajectories for revision planning
- Hounsfield units for bone density assessment
MRI (Selected Indications):
- Infection Suspected: Fluid collections, marrow edema, discitis
- Neurological Symptoms: Neural compression, epidural hematoma
- Soft Tissue Assessment: Muscle atrophy, paraspinal masses
- Use MARS (metal artifact reduction sequences) protocols
Nuclear Medicine:
- SPECT-CT: Functional assessment of fusion
- Hot spots indicate active stress or non-union
- Useful when CT equivocal
- Labeled WBC Scan: Infection diagnosis (sensitivity 85-90%)
- PET-CT: Infection or oncologic concerns
Bone Density Assessment:
- DEXA Scan: Essential for all revision candidates
- T-score less than -2.5 indicates osteoporosis
- Adjust surgical plan based on bone quality
- Consider teriparatide pretreatment if severe
Laboratory Evaluation
Baseline Studies:
- CBC: Anemia (blood loss risk), leukocytosis (infection)
- CMP: Renal function (contrast studies), electrolytes
- Coagulation Studies: Baseline for major surgery
- Type and Screen: Anticipate transfusion needs
Infection Workup (If Suspected):
- CRP and ESR: Elevated suggests infection (CRP greater than 10 mg/L)
- Blood Cultures: If systemic sepsis suspected
- Aspiration: Cell count, culture, sensitivity
- Greater than 3000 WBCs with greater than 80% PMNs suggests infection
- Send for aerobic, anaerobic, fungal cultures
Bone Health and Nutrition:
- Vitamin D: Target greater than 30 ng/mL
- Calcium, PTH: Assess calcium metabolism
- Albumin, Prealbumin: Nutritional status (albumin greater than 3.5 g/dL)
- HbA1c: Glycemic control (target less than 7.0%)
Specialized Tests:
- Teriparatide Level: If considering anabolic therapy
- Bone Turnover Markers: Assess bone metabolism (research setting)
High Yield
Management
Non-Operative Management
Indications for Conservative Treatment:
- Medical comorbidities prohibitive for surgery
- Frail patients with limited life expectancy
- Patient preference after informed discussion
- Asymptomatic radiographic findings (incidental PJK, asymptomatic pseudarthrosis)
- Mild symptoms manageable conservatively
Conservative Management Strategies:
Bracing:
- TLSO: For mechanical back pain, pseudarthrosis
- Limited efficacy in adult deformity (poor compliance)
- May temporize symptoms while optimizing for surgery
- Custom-molded braces for better fit in deformed spine
Pain Management:
- Multimodal Analgesia: Acetaminophen, NSAIDs (if renal function allows)
- Neuropathic Agents: Gabapentin, pregabalin for radicular pain
- Muscle Relaxants: Short-term for spasm
- Avoid Long-Term Opioids: Risk of dependence, minimal long-term benefit
- Interventional Pain: Epidural injections, radiofrequency ablation (limited role)
Physical Therapy:
- Core strengthening to unload spine
- Gait training and assistive devices
- Postural exercises (limited effectiveness in fixed deformity)
- Aquatic therapy (buoyancy reduces spinal load)
Lifestyle Modifications:
- Activity modification (avoid prolonged standing, heavy lifting)
- Weight optimization (reduce mechanical load)
- Assistive devices (walker, cane for balance and unloading)
Expected Outcomes:
- Approximately 20-30% achieve acceptable symptom control
- Most patients with significant deformity eventually require surgery
- Conservative management buys time for optimization
Preoperative Optimization
Medical Optimization (Critical for Success):
Bone Health:
- Vitamin D supplementation (target greater than 30 ng/mL, ideally greater than 40)
- Calcium 1500mg daily
- Osteoporosis Treatment:
- Bisphosphonates: Controversial (may impair fusion, stop 3 months preop)
- Teriparatide: Anabolic agent, excellent for fusion augmentation
- Start 3-6 months preoperatively if possible
- Continue 6-12 months postoperatively
Nutritional Optimization:
- Albumin greater than 3.5 g/dL (target greater than 4.0)
- Consider nutritional supplementation if malnourished
- Protein 1.5 g/kg/day for bone healing
Smoking Cessation:
- Absolute Requirement: Minimum 6 weeks, ideally 3 months
- Increases pseudarthrosis risk 3-5 fold if continued
- Consider nicotine replacement therapy
- Verify with serum cotinine levels
Glycemic Control:
- HbA1c less than 7.0% (target less than 6.5%)
- Infection risk increased with poor control
- Coordinate with endocrinology
Weight Optimization:
- BMI less than 35 preferred (less than 40 acceptable)
- Weight loss reduces surgical risk and mechanical stress
- May require bariatric surgery consultation
Psychosocial Optimization:
- Assess expectations (often unrealistic in revision setting)
- Screen for depression and anxiety (common after failed surgery)
- Ensure social support for prolonged recovery
- Consider psychology clearance for complex cases
Infection Prevention:
- MRSA Screening and Decolonization: Nasal swab, mupirocin ointment
- Chlorhexidine body wash 3 days preoperatively
- Dental evaluation (eradicate oral infection sources)
Operative Management
Surgical Planning Principles:
-
Define Objectives:
- Achieve solid fusion
- Restore sagittal and coronal balance
- Decompress neural elements if indicated
- Create durable construct
-
Choose Appropriate Technique:
- Match complexity to failure mechanism
- Consider patient factors (age, bone quality, comorbidities)
- Balance risk versus benefit
-
Staged vs Single-Stage:
- Single-Stage: Most revisions if medically fit
- Staged: Infection (explant then reconstruct), ultra-complex cases, medical fragility
Surgical Techniques by Indication:
Revision Strategies by Failure Mechanism
| category | assessment | surgicalStrategy | fixationStrategy | osteotomy | expectedFusionRate |
|---|---|---|---|---|---|
| Pseudarthrosis | CT showing less than 50% bridging bone, possible hardware failure | Expose pseudarthrosis, remove fibrous tissue, decorticate, autograft + BMP | Revise failed screws, extend fixation 1 level proximally and distally | Rarely needed unless deformity progression | 80-90% if isolated, 70-80% if multilevel |
| Proximal Junctional Kyphosis | Kyphosis greater than 20 degrees at UIV, compression fracture possible | Extend fusion 2-3 levels cranially, SPO at apex if rigid | Prophylactic vertebroplasty at new UIV, hooks + screws hybrid | SPO (Smith-Petersen Osteotomy) if flexible, PSO if rigid | 75-85%, PJK recurrence 15-25% |
| Flatback/Sagittal Imbalance | SVA greater than 50mm, PI-LL mismatch greater than 20 degrees | Restore lordosis with osteotomy, posterior column release | Robust fixation with dual rods, iliac screws, extend to upper thoracic | PSO (Pedicle Subtraction Osteotomy) for 30-40 degree correction | 70-80%, high complication risk (neurological 5-10%) |
| Distal Junctional Failure | Lumbosacral instability, S1 screw pullout, rod fracture distally | Revise lumbosacral junction, autograft + BMP | Bilateral iliac screws, S2-alar-iliac screws, cement augmentation | L5-S1 release if ankylosis present | 85-90% with adequate sacropelvic fixation |
| Infection | Elevated CRP/ESR, positive cultures, fluid on MRI | STAGE 1: Explant hardware, debridement, culture-directed antibiotics; STAGE 2: Reconstruct after infection cleared (6-12 weeks) | New hardware after infection eradicated, robust fixation | Defer until second stage if needed | 60-75% (lower due to infection history) |
Advanced Surgical Techniques:
Osteotomy Selection:
-
Smith-Petersen Osteotomy (SPO):
- Posterior column release (facets, ligamentum flavum)
- Correction: 10 degrees per level (flexible deformity)
- Multiple levels for gradual correction
- Lower neurological risk than PSO
-
Pedicle Subtraction Osteotomy (PSO):
- Three-column osteotomy through single posterior approach
- Correction: 30-40 degrees per level
- Indicated for rigid flatback deformity
- Higher neurological risk (5-10%)
- Requires robust fixation (dual rods, extension 3-4 levels each side)
-
Vertebral Column Resection (VCR):
- Complete vertebrectomy (all three columns)
- Maximum correction potential (50-70 degrees)
- Reserved for severe rigid deformity, ultra-complex revisions
- Highest neurological risk (10-20%)
- Requires ICU monitoring, neuromonitoring, experienced team
Fixation Strategies:
Screw Placement in Revision:
- New Trajectories: Angle screws to avoid prior screw tracks
- Salvage Techniques:
- Larger diameter screws (6.5mm vs 5.5mm)
- Longer screws for bicortical purchase
- Cement augmentation in osteoporotic bone (polymethylmethacrylate)
- Cortical bone trajectory screws (alternative to pedicle screws)
Supplemental Fixation:
- Hooks: Laminar or pedicle hooks at proximal levels
- Sublaminar Wires: Polyester bands for additional fixation
- Iliac Screws: Mandatory for lumbosacral revisions
- S2-Alar-Iliac (S2AI) Screws: Lower profile alternative to traditional iliac screws
Rod Configuration:
- Dual Rods: Bilateral rods on each side (four rods total)
- Satellite Rods: Supplemental rods to reinforce high-stress zones
- Cobalt-Chromium: Preferred for high-stress constructs (better fatigue resistance)
- Larger Diameter: 6.0mm or 6.35mm (5.5mm inadequate for long revisions)
Biological Augmentation:
- Autograft: Iliac crest or local bone (gold standard)
- Allograft: Structural support, bulk (cancellous chips, DBM)
- BMP-2: Off-label for posterior fusion, 1.5 mg/mL concentration
- Higher doses increase complications (seroma, ectopic bone)
- Avoid in anterior cervical spine (swelling risk)
- Bone Marrow Aspirate: Adjunct to autograft/allograft
Neuromonitoring:
- Somatosensory Evoked Potentials (SSEPs): Monitor dorsal column function
- Motor Evoked Potentials (MEPs): Monitor corticospinal tract (more sensitive for motor deficit)
- Triggered EMG: Pedicle screw placement, nerve root monitoring
- Free-Running EMG: Continuous nerve root monitoring during dissection
- Stagnara Wake-Up Test: Backup if neuromonitoring unavailable or questionable changes
Postoperative Management
ICU Care (First 24-48 Hours):
- Neurological checks every 2 hours
- Hemodynamic monitoring (PSO/VCR cases)
- Pain control (epidural, PCA, multimodal)
- Strict I/O monitoring (blood loss replacement)
- Drain management (remove when output less than 50 mL/8 hours)
Early Mobilization (Critical):
- Out of bed to chair POD1 if neurologically intact
- Physical therapy initiated immediately
- Early mobilization reduces complications (DVT, pneumonia, ileus)
- TLSO brace for first 3 months if osteotomy performed
Thromboprophylaxis:
- Mechanical: Sequential compression devices, early mobilization
- Chemical: Enoxaparin or heparin starting POD1 (after drain removal)
- Duration: Minimum 4 weeks, consider extended prophylaxis to 12 weeks
Nutritional Support:
- High-protein diet (1.5 g/kg/day)
- Vitamin D and calcium supplementation
- Consider nutritional consultation if poor intake
Bone Health Continuation:
- Continue teriparatide 12-24 months if started preoperatively
- Vitamin D and calcium indefinitely
- Repeat DEXA at 1-2 years
Surveillance Protocol:
- 2 weeks: Wound check, staple/suture removal, pain assessment
- 6 weeks: Radiographs (AP/Lateral standing full-length), advance PT
- 12 weeks: Radiographs, discontinue brace if appropriate
- 6 months: Radiographs, CT if fusion concern
- 12 months: Radiographs and CT to confirm fusion
REVISIONREVISION Success Checklist
| R | Remove All fibrous tissue at pseudarthrosis site |
| E | Extend Fixation adequately (3-4 levels beyond osteotomy) |
| V | Verify Sagittal balance correction intraoperatively |
| I | Iliac screws For lumbosacral constructs |
| S | Supplement Biology (autograft, BMP, teriparatide) |
| I | Infection Ruled out and treated |
| O | Osteotomy Selection appropriate for deformity |
| N | Neuromonitoring Throughout procedure |
| R | Remove All fibrous tissue at pseudarthrosis site | I | Iliac screws For lumbosacral constructs | O | Osteotomy Selection appropriate for deformity |
| E | Extend Fixation adequately (3-4 levels beyond osteotomy) | S | Supplement Biology (autograft, BMP, teriparatide) | N | Neuromonitoring Throughout procedure |
| V | Verify Sagittal balance correction intraoperatively | I | Infection Ruled out and treated |
Hook:Examiners assess systematic approach - demonstrate reproducible method for complex revision cases
Complications
Major Complications
Neurological Injury (5-15% in Complex Revisions):
Risk Factors:
- Osteotomy procedures (PSO, VCR)
- Severe deformity correction
- Epidural scarring from prior surgery
- Prolonged retraction
Prevention:
- Multimodal neuromonitoring
- Meticulous technique during dural dissection
- Gradual deformity correction
- Triggered EMG during screw placement
- Maintain mean arterial pressure greater than 85 mmHg
Management:
- Immediate recognition (neuromonitoring changes)
- Release correction if needed
- Wake-up test to confirm
- Urgent MRI if postoperative deficit
- Emergent revision if hematoma or hardware malposition
Infection (8-15% in Revisions):
Risk Factors:
- Diabetes (HbA1c greater than 7.5%)
- Obesity (BMI greater than 35)
- Prolonged surgery (greater than 8 hours)
- Prior infection
- Malnutrition (albumin less than 3.5)
Prevention:
- Preoperative optimization (glycemic control, weight loss)
- Prophylactic antibiotics (cefazolin 2g, redose every 4 hours)
- Meticulous hemostasis and dead space obliteration
- Closed suction drainage
- Negative pressure wound therapy in high-risk cases
Management:
- Early (Less than 3 months): Irrigation and debridement, retain hardware, culture-directed antibiotics 6 weeks IV then 6 weeks PO
- Late (Greater than 3 months): Staged revision (explant, antibiotics 6-12 weeks, reconstruct)
- Biofilm-disrupting antibiotics (rifampin for staphylococci)
Proximal Junctional Kyphosis (20-30% Recurrence After Revision):
Risk Factors:
- Osteoporosis (T-score less than -2.5)
- Overcorrection of lumbar lordosis
- UIV at inflection point (T10-L1)
- Age greater than 65
Prevention:
- Gradual lordosis transition at UIV
- Prophylactic vertebroplasty at UIV and UIV+1
- Extend fusion to upper thoracic (T2-T4) in high-risk cases
- Avoid fusion termination at T10 (extend to T9 or stop at T11)
Management:
- Observation if asymptomatic (kyphosis less than 20 degrees)
- Revision if symptomatic or severe (kyphosis greater than 30 degrees)
- Further cranial extension with osteotomy
Pseudarthrosis (15-30% in Complex Revisions):
Risk Factors:
- Smoking (3-5 fold increased risk)
- Diabetes
- Osteoporosis
- Multilevel revision
- Osteotomy site
- Inadequate biologics
Prevention:
- Smoking cessation (absolute requirement)
- Optimize bone health (vitamin D, teriparatide)
- Generous autograft + BMP
- Robust fixation (extend fixation, dual rods)
- Postoperative immobilization (TLSO 12 weeks)
Management:
- Observation if asymptomatic and no hardware failure
- Revision if symptomatic or hardware failure
- Address all risk factors before re-revision
Medical Complications
Medical Complications in Revision Deformity Surgery
| category | incidence | riskFactors | prevention | management |
|---|---|---|---|---|
| Venous Thromboembolism | 3-5% (DVT), 0.5-1% (PE) | Prolonged surgery, immobility, obesity, age | SCDs, early mobilization, chemical prophylaxis, risk stratification | Anticoagulation (balancing bleed risk), IVC filter if recurrent |
| Cardiac Complications | 2-5% (MI, arrhythmia) | Age greater than 70, CAD, CHF, prolonged surgery | Preoperative cardiac clearance, beta-blocker if indicated, fluid management | Cardiology consultation, ICU monitoring, treat underlying cause |
| Pulmonary Complications | 5-10% (pneumonia, atelectasis) | Smoking, COPD, prolonged intubation, poor mobilization | Smoking cessation, incentive spirometry, early mobilization, minimize opioids | Respiratory therapy, antibiotics if pneumonia, oxygen support |
| Acute Kidney Injury | 2-5% | Preexisting renal disease, hypotension, contrast exposure, rhabdomyolysis | IV hydration, avoid nephrotoxic agents, maintain MAP greater than 65 | Nephrology consultation, correct reversible causes, dialysis if severe |
| Delirium | 10-20% (age greater than 65) | Age, dementia, prolonged surgery, pain, medications | Minimize opioids and benzodiazepines, sleep hygiene, orientation, family presence | Treat underlying cause, avoid antipsychotics unless severe, supportive care |
Prognosis and Outcomes
Expected Outcomes
Successful Revision:
- Pain Relief: 60-70% achieve significant improvement (greater than 30% reduction in VAS)
- Functional Improvement: 50-60% meaningful improvement in ODI or SRS-22
- Fusion Rate: 70-85% depending on complexity and bone quality
- Patient Satisfaction: 50-65% satisfied or very satisfied (lower than primary surgery)
Radiographic Outcomes:
- SVA Correction: Target SVA less than 50mm achieved in 75-85%
- PI-LL Restoration: Within 10 degrees in 70-80%
- Coronal Balance: CVA less than 30mm in 80-90%
Complication Rates:
- Any Complication: 40-60% (Grade 1-2: 30-40%, Grade 3-4: 10-20%)
- Reoperation: 15-25% within 2 years
- Mortality: 0.5-1% (higher in elderly or ultra-complex cases)
Predictors of Success
Positive Predictors:
- Achievement of solid fusion
- Restoration of sagittal balance (SVA less than 50mm, PI-LL within 10 degrees)
- Younger age (less than 65)
- Good bone quality
- Non-smoker
- Optimal nutritional status
- Single failure mechanism
- First revision (versus multiple prior revisions)
Negative Predictors:
- Multiple prior revisions (greater than 2)
- Active smoking
- Severe osteoporosis (T-score less than -3.0)
- Multiple comorbidities (Charlson Comorbidity Index greater than 3)
- Unrealistic expectations
- Psychological comorbidity (depression, chronic pain syndrome)
- Chronic opioid use preoperatively
Long-Term Outcomes
5-Year Outcomes:
- Fusion rate: 75-85% if first revision
- Adjacent segment disease: 20-30%
- Need for further revision: 20-30%
- Maintained improvement: 60-70% of those initially improved
10-Year Outcomes:
- Limited data due to heterogeneous patient population
- Cumulative revision rate: 30-40%
- Adjacent segment degeneration: 35-45%
- Patient satisfaction maintained: 50-60%
OUTCOMEOUTCOME Predictors for Success
| O | Optimize Bone health (vitamin D, teriparatide, DEXA) |
| U | Undercorrection Avoided (achieve target SVA and PI-LL) |
| T | Tobacco Cessation (absolute requirement) |
| C | Complications Minimized (infection prevention, neuromonitoring) |
| O | Osteotomy Appropriate (match technique to deformity) |
| M | Multilevel Biologics (autograft + BMP at all levels) |
| E | Expectations Realistic (60-70% pain relief, not cure) |
| O | Optimize Bone health (vitamin D, teriparatide, DEXA) | C | Complications Minimized (infection prevention, neuromonitoring) | E | Expectations Realistic (60-70% pain relief, not cure) |
| U | Undercorrection Avoided (achieve target SVA and PI-LL) | O | Osteotomy Appropriate (match technique to deformity) | ||
| T | Tobacco Cessation (absolute requirement) | M | Multilevel Biologics (autograft + BMP at all levels) |
Hook:Patients with greater than 4 favorable factors have best outcomes - use for counseling
Controversies and Areas of Uncertainty
The evidence base in revision deformity surgery is dominated by retrospective cohorts and registry data; few questions have Level I answers. Examiners reward candidates who can articulate the genuine areas of equipoise.
- rhBMP-2 use: Reduces pseudarthrosis and revision odds (Passias 2016) but carries cost, off-label status, and dose-dependent complications (seroma, ectopic bone). Optimal dose and patient selection remain unsettled; use has risen then plateaued, with lower doses over time.
- Bisphosphonates versus anabolics: Teriparatide has Level I support for enhancing fusion (Ebata 2017). Whether perioperative bisphosphonates impair fusion is debated - the older "stop before surgery" dogma is increasingly questioned, but anabolic therapy is preferred when osteoporosis coexists with prior pseudarthrosis.
- Prophylactic vertebroplasty/tethering at the UIV: Reduces proximal junctional failure in some series, but durability, ideal technique (cement vs ligamentous tethers vs hooks), and cost-effectiveness are not established.
- SPO versus PSO for a given correction: Multiple short SPOs can rival a single PSO for moderate flexible deformity with less blood loss; a head-to-head meta-analysis in ankylosing spondylitis found no clear superiority of PSO and flagged rare aortic injury with SPO. Choice remains surgeon- and deformity-specific.
- Single-stage versus staged revision for infection: Acute infection may be managed with debridement and implant retention, but the threshold (commonly cited as under versus over 3 months), the role of biofilm-active agents (rifampicin), and when to stage explantation are not standardized.
- When NOT to operate: There is no validated threshold for prohibitive risk. Frailty indices and the SRS-Schwab/age-adjusted alignment targets help, but the decision to decline revision in the frail, osteoporotic, or chronic-pain patient remains a judgement call - and is itself a high-yield examiner theme.
Evidence Base
- New neurological deficit in 1.0% overall; revision cases 1.25% vs primary 0.89% (41% higher, p less than 0.001)
- Cases with implants had more than double the deficit rate of cases without (1.15% vs 0.52%)
- Of new spinal cord deficits, neuromonitoring changes were reported in only 40% - imperfect sensitivity
- Weekly teriparatide for 6 months after lumbar interbody fusion in osteoporotic women significantly increased CT-confirmed fusion vs controls
- Effect seen as early as 4 months (modified intention-to-treat) and at 6 months (per-protocol)
- Bone metabolic markers confirmed increased formation and decreased resorption
- Mean lordosis increase of 34.1 degrees and mean C7 plumb-line improvement of 13.5 cm
- Pseudarthrosis through the osteotomy site in only 1 patient; thoracic pseudarthrosis in 6
- Significant Oswestry and pain-score improvement; worse results with comorbidity and thoracic pseudarthrosis
- Pseudarthrosis in 29% (10 of 35), all at adjacent fused levels - none at the osteotomy site
- No significant regional radiographic loss between 2 years and ultimate follow-up, though C7 plumb crept anterior over time
- Maintaining SVA under 8 cm at final follow-up predicted better SRS outcome scores
- Acute proximal junctional failure in 5.6% within 28 weeks; mean time 11.4 weeks
- Fracture was the commonest failure mode (47%), followed by soft-tissue failure (44%)
- Thoracolumbar failures (66%) were more often fracture-related; upper-thoracic failures more often soft-tissue
- Radiographic/implant-related complications in 31.7%; 52.6% of those required reoperation
- Rod breakage accounted for 47% of implant complications; PJK for 54.5% of radiographic complications
- Independent predictors: higher ASA grade and severe sagittal vertical axis modifier (++)
- Revision (excluding infection) in 16.5%; nearly half occurred between 1 and 2 years
- Implant complications, then PJK and rod failure, were the leading indications
- Larger-diameter rods (OR 0.51) and rhBMP-2 (OR 0.16) were associated with lower revision odds; higher body mass and preoperative SVA increased risk
- Restore age-adjusted sagittal alignment (PI-LL, SVA, pelvic tilt) rather than uniform targets
- Mandatory multimodal intraoperative neuromonitoring for three-column osteotomy
- Multidisciplinary preoperative optimization (bone health, nutrition, smoking, glycaemia, frailty) before elective revision
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Failed Deformity Surgery with Flatback
"A 68-year-old woman presents 2 years after T10-pelvis fusion for degenerative scoliosis. She reports excellent initial pain relief, but over the past 6 months developed progressive inability to stand upright. She can only walk 50 meters stooped forward with a walker. Examination shows she cannot achieve horizontal gaze when standing. Standing radiographs show SVA of 180mm, PI-LL mismatch of 45 degrees, and CT demonstrates solid fusion at all levels. She has osteoporosis (T-score -2.8) and controlled diabetes (HbA1c 6.8%)."
Early Proximal Junctional Kyphosis After Deformity Correction
"A 72-year-old man underwent T10-pelvis fusion for adult scoliosis 4 months ago. He initially did well but now presents with acute worsening back pain over 2 weeks and progressive forward stooping. Radiographs show new kyphosis of 35 degrees at T8-T9 with T9 compression fracture. His pain limits walking to inside his home only. Medical history includes osteoporosis (on alendronate), coronary artery disease with stents 3 years ago, and obesity (BMI 38)."
Late Deep Infection of a Long Deformity Construct
"A 60-year-old woman is 14 months out from a T4-pelvis fusion for adult scoliosis. She presents with 8 weeks of insidious mid-back pain, intermittent low-grade fevers, and a 2-week history of clear-then-cloudy drainage from the caudal end of her incision. CRP is 65 mg/L and ESR is 70 mm/hr. Radiographs show intact alignment but a 2mm lucency around the S1 screws. MRI shows a paraspinal fluid collection adjacent to the lower instrumentation. She is otherwise well with no neurological deficit."
MCQ Practice Points
Clinical Pearl
Q: What are the common indications for revision spinal deformity surgery?
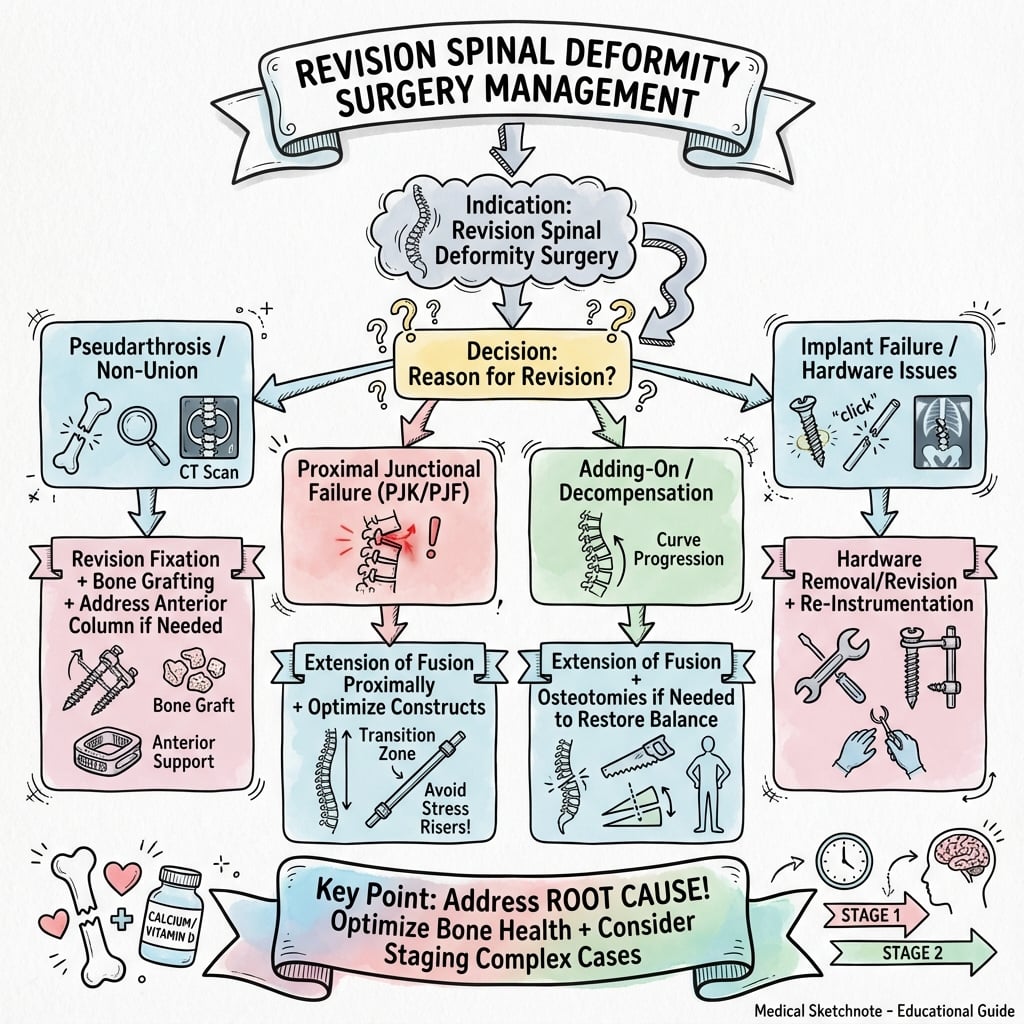
A: Mechanical failures: Pseudarthrosis (most common), rod fracture, screw pullout, proximal junctional kyphosis (PJK)/failure (PJF), distal junctional failure, loss of correction. Clinical failures: Persistent pain (adjacent segment disease, nonunion), neurological deterioration (spinal stenosis, foraminal stenosis), infection (implant-associated). Inadequate initial correction: Persistent sagittal imbalance (SVA greater than 5cm), residual coronal deformity, flatback syndrome. Understanding why the primary surgery failed is critical for planning revision - addressing root cause prevents recurrent failure.
Clinical Pearl
Q: What is proximal junctional kyphosis (PJK) and what are the risk factors?
A: PJK definition: Kyphosis greater than 10 degrees at the proximal junction (between upper instrumented vertebra and first non-instrumented vertebra) OR increase greater than 10 degrees from preoperative. Proximal junctional failure (PJF): Symptomatic PJK with structural failure (fracture, implant failure). Risk factors: Age greater than 60 years, osteoporosis, large sagittal correction (greater than 30 degrees), UIV at thoracolumbar junction (T10-L1), disruption of posterior ligamentous complex, long fusions to pelvis, high BMI, preoperative SVA greater than 5cm. Prevention: Optimize bone quality, consider prophylactic vertebroplasty, avoid abrupt transitions in stiffness.
Clinical Pearl
Q: What preoperative planning is essential for revision deformity surgery?
A: Clinical assessment: Pain location, neurological status, functional limitations, patient expectations. Imaging: Full-length standing radiographs (sagittal and coronal balance), CT (assess fusion, screw position, bone quality), MRI (neural compression, disc degeneration, infection), consider DEXA (bone density). Laboratory: Inflammatory markers (rule out infection), nutritional markers (albumin, prealbumin). Calculate targets: Ideal lumbar lordosis (PI minus 10), target SVA (less than 5cm), pelvic parameters. Identify failure mechanism: Pseudarthrosis site, implant failure location, cause of junctional failure. Plan osteotomy type and level if correction needed.
Guidelines, Registries & Global Practice
Global Epidemiology
- Revision after primary adult deformity surgery occurs in 15-30% by 5 years across international multicentre cohorts (ISSG, European Spine Study Group)
- Mechanical failure (rod fracture, PJK/PJF, pseudarthrosis) drives most reoperations; implant-related complications affect roughly one-third of long constructs (Soroceanu 2015)
- Patients are typically 55-75 years, older and frailer than the primary cohort, amplifying medical and bone-quality risk
Side-by-Side Society Guidance
Major Society Positions Relevant to Revision Deformity Surgery
| society | alignmentTargets | neuromonitoring | registry |
|---|---|---|---|
| Scoliosis Research Society (SRS) | Age-adjusted sagittal targets (PI-LL, SVA, PT); SRS-Schwab classification for risk | Multimodal monitoring expected for deformity correction and osteotomy | SRS Morbidity & Mortality database benchmarks neurological and complication rates |
| AO Spine (Knowledge Forum Deformity) | Restore individualized alignment; structured osteotomy selection (Schwab grades 1-6) | Mandatory for three-column osteotomy (PSO/VCR) | AO Spine education and complication frameworks; AOSpine classification systems |
| BOA / NICE (UK) | Evidence-based selection; NICE NG59 cautions against surgery for non-specific pain alone | Recommended for high-risk corrective surgery | British Spine Registry captures outcomes and revision data |
| NASS / AAOS (US) | Emphasis on documented failure mechanism and realistic outcome counselling | Standard of care for instrumented deformity correction | Quality and outcomes registries inform appropriateness criteria |
Registry Evidence
- SRS M&M database (108,419 procedures): revision cases carry a 41% higher new-neurological-deficit rate than primary surgery (Hamilton/Smith 2011) - the global benchmark for consent
- National spine registries (British Spine Registry, Scandinavian Swespine, and others) track revision rates, PJK, and patient-reported outcomes, enabling cross-system comparison
- Registry data consistently identify rod fracture, PJK/PJF, and pseudarthrosis as the dominant mechanical reasons for reoperation
High- versus Limited-Resource Practice Variation
- Well-resourced centres: routine multimodal neuromonitoring, cell salvage, ICU, intraoperative imaging/navigation, BMP and anabolic bone agents, staged protocols for infection
- Limited-resource settings: neuromonitoring and ICU may be scarce, shifting practice toward lower-risk techniques (multiple SPOs rather than VCR), the Stagnara wake-up test as a monitoring backup, autograft over costly biologics, and a higher threshold for elective revision
- Across all settings the core principles are constant: define the failure mechanism, optimize the host, restore sagittal balance, secure robust fixation, and know when to decline surgery
Management Algorithm
Clinical summary
Revision Deformity Essentials
- •Ultra-complex surgery with 40-60% complication rate
- •Common indications: pseudarthrosis (35-40%), PJK (25-30%), sagittal imbalance (20-25%), infection (10-15%)
- •Multiple failure mechanisms often coexist
- •Success requires identifying ALL failure modes
- •Comprehensive medical optimization essential (bone health, nutrition, smoking cessation)
- •Realistic outcome expectations: 60-70% meaningful improvement, not cure
Assessment Protocol - IMAGING Mnemonic
- •I - Identify failure mechanism (pseudarthrosis, PJK, alignment)
- •M - Measure sagittal parameters (SVA, PI-LL, PT)
- •A - Assess hardware (screws, rods, connectors)
- •G - Gold standard CT for fusion evaluation
- •I - Infection ruled out (CRP, ESR, MRI if needed)
- •N - Nuclear medicine if CT equivocal
- •G - Get bone density (DEXA mandatory)
- •CT with metal artifact reduction is gold standard (greater than 50% bridging = solid)
Complexity Grading
- •Grade 1 (Simple): Focal pseudarthrosis, solid elsewhere, 3-5 hours, 15-25% complications
- •Grade 2 (Moderate): Multilevel pseudarthrosis or PJK, SPO possible, 5-8 hours, 25-40% complications
- •Grade 3 (Complex): Major deformity, requires PSO, 8-12 hours, 40-60% complications
- •Grade 4 (Ultra-complex): Multiple prior revisions, severe rigid deformity, staged, 60-80% complications
Osteotomy Selection
- •SPO (Smith-Petersen): Posterior column release, 10 degrees/level, flexible deformity, lower neuro risk
- •PSO (Pedicle Subtraction): Three-column, 30-40 degrees/level, rigid flatback, 5-10% neuro risk
- •VCR (Vertebral Column Resection): Complete vertebrectomy, 50-70 degrees, 10-20% neuro risk
- •Match osteotomy to deformity magnitude and rigidity
Fixation Strategies
- •Screw revision: new trajectories, larger diameter (6.5mm), longer for bicortical, cement if osteoporotic
- •Supplemental fixation: hooks proximally, sublaminar wires, iliac screws mandatory for lumbosacral
- •Rod configuration: dual rods (four total), cobalt-chromium preferred, 6.0-6.35mm diameter
- •Biologics: autograft + allograft + BMP-2 (1.5mg/mL), teriparatide perioperatively
Surgical Strategy by Failure Mechanism
- •Pseudarthrosis: expose, remove fibrous tissue, decorticate, autograft + BMP, extend fixation 1 level each
- •PJK: extend 2-3 levels cranially, SPO if rigid, prophylactic vertebroplasty at new UIV
- •Flatback: PSO for 30-40 degree correction, dual rods, extend to upper thoracic, iliac screws
- •Distal junctional failure: revise lumbosacral junction, bilateral iliac/S2AI screws, cement
- •Infection: STAGED - explant/debridement/antibiotics 6-12 weeks, then reconstruct
Preoperative Optimization - Critical
- •Bone health: vitamin D greater than 30 ng/mL, calcium 1500mg daily, teriparatide 3-6 months preop
- •Nutrition: albumin greater than 3.5 g/dL, protein 1.5 g/kg/day
- •Smoking: ABSOLUTE cessation minimum 6 weeks, ideally 3 months
- •Glycemic control: HbA1c less than 7.0%
- •Weight: BMI less than 35 preferred
- •MRSA decolonization, dental clearance, psychology assessment
Major Complications and Rates
- •Neurological injury: 5-15% (higher with PSO/VCR), prevent with neuromonitoring
- •Infection: 8-15%, prevent with preop optimization, prophylactic antibiotics
- •Recurrent PJK: 20-30%, prevent with prophylactic vertebroplasty, gradual lordosis transition
- •Pseudarthrosis: 15-30%, prevent with smoking cessation, biologics, teriparatide
- •Medical complications: 10-20% (VTE, cardiac, pulmonary), early mobilization essential
Expected Outcomes - Realistic Counseling
- •Pain relief: 60-70% significant improvement (NOT pain-free)
- •Functional improvement: 50-60%
- •Fusion rate: 70-85%
- •Patient satisfaction: 50-65% (lower than primary)
- •Reoperation: 15-25% within 2 years
- •Positive predictors: solid fusion, SVA less than 50mm, non-smoker, first revision
- •Negative predictors: multiple revisions, smoking, severe osteoporosis, chronic pain syndrome
Examiner Expectations - Demonstrate Judgment
- •Show systematic assessment (identify ALL failure mechanisms)
- •Demonstrate knowledge of complex techniques (osteotomy, fixation)
- •Emphasize importance of medical optimization
- •Discuss realistic outcomes (moderate success, high complication rate)
- •Show judgment about when NOT to operate (prohibitive risk, unrealistic expectations)
- •Discuss multidisciplinary care (medicine, cardiology, nutrition, psychology)