An Overuse Injury (Classically of Rowers)
- A RIB STRESS FRACTURE is an OVERUSE (fatigue) fracture of a rib from REPETITIVE cyclical loading of the thoracic cage - repeated muscular, respiratory and rotational forces exceeding the bone's remodelling capacity - and it is the rib counterpart of the stress fractures seen at other load-bearing sites.
- The CLASSIC setting is ROWING, where the repetitive drive/recovery cycle loads the POSTEROLATERAL mid-ribs; rib stress fractures also occur in THROWING athletes (notably the FIRST RIB, from serratus anterior/scalene traction), in GOLFERS (the leading-side ribs), and from BACK-PACK/load carriage and other repetitive activities.
- The PRESENTATION is LOCALISED, activity-related CHEST-WALL PAIN with point TENDERNESS over the affected rib, worse with the causative ACTIVITY, deep breathing, coughing and trunk rotation; the onset is typically insidious and progressive with continued training.
- CONTRIBUTORY FACTORS: a recent increase in TRAINING LOAD/volume or a technique change is the best-supported driver - incidence rose significantly in the pre-Olympic year of an elite squad. Energy availability and bone health (RED-S, calcium, vitamin D, menstrual status) should still be screened and corrected, but be careful with the bone-density claim: in the collegiate study most often quoted for it, the female rowers' skeletal measures were EQUIVALENT TO CONTROLS AND WITHIN NORMAL RANGES. The clearest nutritional signal was that injury-free rowers consumed over 500 mg/day more CALCIUM.
- WHAT DID NOT PREDICT INJURY. In the elite cohort there was no significant difference in prevalence by SEX, by SWEEP versus SCULL, or by WEIGHT CLASS - the three factors most commonly assumed to matter. With only 19 events these are undetected differences rather than proven equivalence, but do not assert them as risk factors.
- DIAGNOSIS: plain radiographs are often NEGATIVE in the early stress-reaction phase. MRI is the modality of choice and is recommended FIRST-LINE - it grades the injury by distinguishing a stress REACTION from a completed FRACTURE, which changes the expected time lost, and avoids irradiating a young athlete. Bone scan is sensitive but non-specific and cannot grade. The differential includes intercostal/serratus strain and costochondral pathology, and a pathological fracture must be excluded if the history is atypical.
- MANAGEMENT is PREDOMINANTLY NON-OPERATIVE - relative rest, load management, graded return, analgesia, correction of training/technique error, and attention to bone health and nutrition - but QUOTE THE COST HONESTLY. In elite rowers a stress FRACTURE cost a median 69 days lost to full on-water training (IQR 56-157) and a stress REACTION a median 57 days (IQR 45-78): a median of about 10 WEEKS, which the authors noted was longer than previously published. Surgery is rarely needed.
- “Rib stress fracture = OVERUSE (fatigue) fracture of a rib from repetitive thoracic-cage loading. CLASSIC in ROWERS (posterolateral mid-ribs); also throwers (FIRST rib), golfers (leading side), load carriage.
- “Localised activity-related chest-wall pain + point tenderness, worse with the activity/deep breathing/rotation. Radiographs often NEGATIVE early -> MRI FIRST-LINE (grades reaction vs fracture; no radiation). Commonest site on imaging: mid-axillary line, rib 6.
- “TIME LOST: median 69 days for a fracture (IQR 56-157), 57 days for a reaction (IQR 45-78) - about 10 weeks, longer than usually taught. Reactions outnumber fractures 12:7.
- “Contributors: training load/technique (incidence rose in the pre-Olympic year). Calcium intake differed by 500 mg/day between injured and injury-free rowers - but their bone density was NORMAL. No difference by sex, sweep vs scull, or weight class.
Features, Diagnosis & Management
A rib stress fracture is an overuse (fatigue) fracture of a rib from repetitive thoracic-cage loading, classically in rowers (posterolateral mid-ribs), also in throwers (first rib), golfers and from load carriage. It presents with localised, activity-related chest-wall pain and point tenderness, worse with the causative activity, deep breathing and trunk rotation. Contributors are training load/technique and impaired bone - low bone mineral density and low energy availability (RED-S), especially in female athletes. Plain radiographs are often negative early, so a bone scan or MRI confirms it. Management is predominantly non-operative: relative rest with load management and graded return, analgesia, correcting training/technique, and addressing bone health/nutrition (RED-S) to prevent recurrence; surgery is rarely needed.
The rib stress fracture is, like other stress fractures, a signal that loading has outstripped the bone's capacity to adapt - so management must go beyond resting the rib. Two things must be addressed to achieve healing and prevent recurrence: the training load and technique (a recent increase in volume or a technique change in the rower, thrower or golfer should be identified and corrected with a graded return), and bone health and energy availability. Low energy availability - relative energy deficiency in sport (RED-S), with its links to low bone mineral density and menstrual disturbance - should be screened for and corrected through nutrition, calcium and vitamin D, and attention to hormonal and menstrual status. Be accurate about how strong that evidence is, though: the collegiate study usually cited for low bone mass in rowers in fact found their skeletal measures equivalent to matched controls and within normal ranges, and the clearest difference between injured and injury-free rowers was calcium intake, over 500 mg per day higher in those without injury. Diagnostically, the trap is that early rib stress injuries are often invisible on plain radiographs, so MRI is needed when clinical suspicion is high - it is recommended first-line and, unlike a bone scan, it separates a stress reaction from a completed fracture, which changes what you tell the athlete about time lost. An atypical history should prompt exclusion of a pathological fracture. With relative rest, load management and correction of the contributory factors these injuries heal and surgery is rarely required - but recovery is slower than often assumed, a median of roughly ten weeks off full on-water training in elite rowers, with the upper quartile after a completed fracture extending beyond five months.
Why the Posterolateral Rib Fails in Rowers: The Force Couple
- The force couple (Karlson). The posterolateral rib is caught between two opposing muscular pulls: the serratus anterior (pulling the scapula/rib forward and rotating it) and the external oblique / abdominal wall (pulling the rib down and in during the finish/lay-back of the stroke). This creates a repetitive bending moment at the posterolateral rib - its weakest, most-loaded point - which, cycled thousands of times per session, exceeds the bone's remodelling capacity and fatigues it.
- Where it actually happens. The bending stress is maximal over the posterolateral to lateral segment of the middle ribs (roughly ribs 5-9), and the rib fails in bending, not compression. Be precise about the commonest site: in the elite Australian cohort the injuries clustered at the mid-axillary line and at rib 6 - so "mid-axillary, rib 6" is the more accurate answer than a vague "posterolateral", and it is where you should palpate first.
- The contributory factors amplify it. A recent increase in volume, and a technique or rigging change, lower the threshold at which the repetitive bending exceeds the bone's capacity. Training load has direct support: incidence rose significantly in the pre-Olympic year (p less than 0.001) in that cohort.
- What did NOT differ. In the same cohort there was no significant difference in prevalence by sex, by sweep versus scull, or by weight class. Those are the three factors candidates most often name as risk factors, and none of them separated the injured from the uninjured - though with only 19 events the study could not have detected a modest difference.
Q: Why do rowers get posterolateral rib stress fractures - what is the mechanism?
A: The posterolateral rib is subjected to a repetitive bending moment from an opposing muscular force couple: the serratus anterior pulls the rib/scapula forward and rotates it, while the external oblique and abdominal wall pull it down and in during the finish/lay-back of the stroke (Karlson). Cycled thousands of times, this bending at the rib's weakest, most-loaded posterolateral segment (roughly ribs 5-9) fatigues the bone - amplified by training-load spikes, technique/rigging changes and impaired bone (RED-S/low BMD).
How Long Does It Actually Cost? The Numbers to Quote
"Relative rest and a graded return" is not an answer an athlete or a coach can plan around. The elite cohort gives real figures, and they are longer than most candidates expect.
- Time lost to full on-water training. A rib stress fracture cost a median 69 days (IQR 56-157); a bone stress reaction cost a median 57 days (IQR 45-78). That is a median of roughly 10 weeks either way, and the authors specifically observed that this is greater than previously published figures - so do not promise a four-to-six week recovery.
- Read the interquartile ranges, not just the medians. For a completed fracture the upper quartile stretches to 157 days - more than five months. The reaction group is far tighter (45-78 days). Catching the injury at the reaction stage does not merely shorten recovery a little; it removes the long tail.
- Reactions outnumber fractures. Of 19 rib stress injuries, 12 were stress reactions and only 7 were fractures. Most of what presents is pre-fracture bone stress, which is precisely why imaging that detects marrow oedema matters.
- How common. Period prevalence ranged from 4% to 15.4% across the years of one Olympiad, with incidence between 0.13 and 0.27 per 1000 athlete days - a common enough problem in an elite squad that it materially disrupts a season.
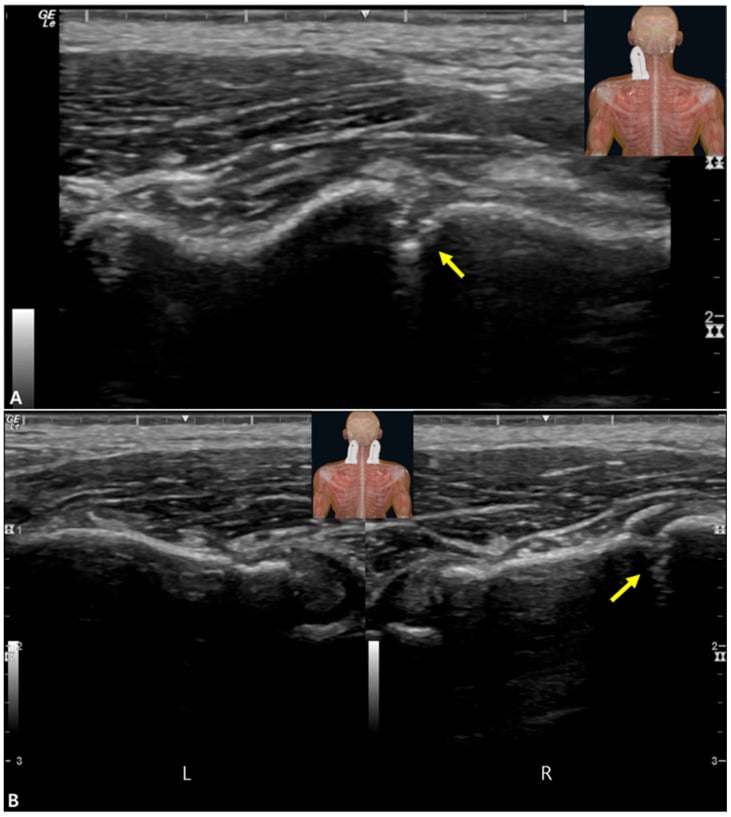
The traditional teaching pairs "bone scan or MRI" for the radiographically occult stress fracture. In the elite rowing cohort MRI was the most commonly used modality and the authors recommend it as the first-line investigation. MRI shows marrow oedema, distinguishes a stress reaction from a completed fracture - a distinction that carries a real difference in expected time lost - involves no ionising radiation in a young athlete, and simultaneously assesses the intercostal soft tissues in the differential. Bone scan remains sensitive but is non-specific, cannot grade the injury, and irradiates. Ultrasound is described as an emerging bedside adjunct, particularly at the first rib, but is not a substitute for MRI.
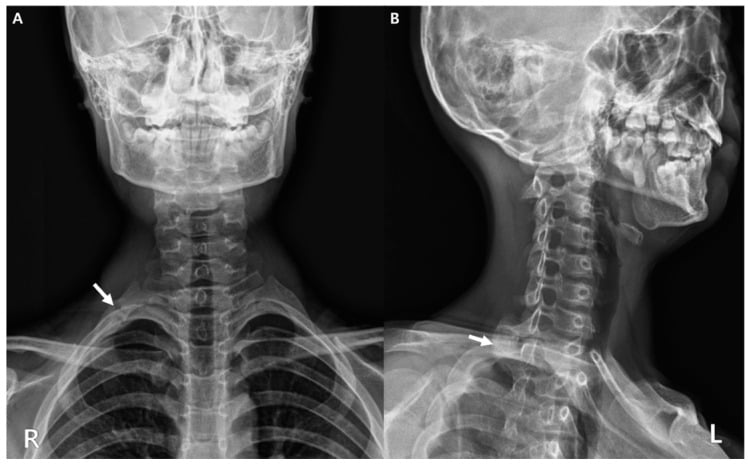
The First-Rib Stress Fracture: A Distinct Entity
- Where and why it fails. It occurs at the subclavian groove - the thinnest part of the first rib, between the insertions of the anterior scalene (in front) and middle scalene, with the subclavius and serratus anterior adding traction. The opposing pulls create a bending/shear stress at this weak point in overhead/throwing athletes (baseball pitchers, javelin throwers, weightlifters).
- Presentation. Vague shoulder/neck/upper-chest or scapular pain in an overhead athlete, sometimes referred - it is easily missed and often diagnosed late.
- Differential. Distinguish it from a congenital first-rib anomaly (a smooth, corticated, often bilateral variant) and an acute traumatic first-rib fracture (high energy); and note the first rib is crossed by the subclavian vessels and brachial plexus, so a rare thoracic-outlet / neurovascular concern exists (although stress fractures seldom cause it).
- Outcome. Like other rib stress fractures it is managed non-operatively (relative rest, load management) and usually heals, though the first rib can be slow to unite and non-union is described.
Q: Describe the first-rib stress fracture - site, mechanism and what to distinguish it from.
A: It occurs at the subclavian groove, the thinnest part of the first rib between the anterior and middle scalene insertions, with the subclavius and serratus anterior adding traction - a bending/shear force in overhead/throwing athletes. It presents as vague shoulder/neck/scapular pain and is easily missed. Distinguish it from a congenital first-rib anomaly (smooth, corticated) and an acute traumatic fracture; note the first rib is crossed by the subclavian vessels/brachial plexus (a rare thoracic-outlet concern). It is managed non-operatively and usually heals, though the first rib can be slow to unite.
Mnemonics & Memory Aids
RIBS
Hook:RIBS: Rowers (mid-axillary, rib 6), Image with MRI, Bone health/calcium, Stress injury (~10 weeks off).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A competitive rower has activity-related localised chest-wall pain; radiographs are normal. What is the likely diagnosis and how do you manage it?”
What it is & who
- Overuse (fatigue) fracture of a rib from repetitive thoracic-cage loading
- Classic in rowers (posterolateral mid-ribs)
- Also throwers (first rib), golfers (leading side), load carriage
Presentation & diagnosis
- Localised activity-related chest-wall pain + point tenderness (worse with activity/breathing/rotation)
- Commonest imaging location in elite rowers: mid-axillary line, rib 6
- Radiographs often negative early -> MRI FIRST-LINE (grades reaction vs fracture, no radiation)
- Exclude pathological fracture if the history is atypical
Numbers to quote
- Time lost: fracture median 69 days (IQR 56-157); stress reaction median 57 days (IQR 45-78) - about 10 weeks
- Reactions outnumber fractures 12:7 - most presentations are pre-fracture bone stress
- Period prevalence 4-15.4%; incidence 0.13-0.27 per 1000 athlete days (151 athletes, 88,773 athlete days)
- Incidence rose significantly in the pre-Olympic year (p less than 0.001) - load drives it
- NO difference by sex, sweep versus scull, or weight class
Contributors & management
- Training load/volume/technique is the best-supported driver; screen energy availability/RED-S
- Injury-free rowers consumed over 500 mg/day more calcium - but their bone density was NORMAL
- Non-operative: relative rest + load management + graded return; analgesia; correct technique
- Address nutrition (calcium/vitamin D, hormonal status); surgery rarely needed
Evidence & Key Studies
Rib stress injuries in the 2012-2016 (Rio) Olympiad: a cohort study of 151 Australian Rowing Team athletes for 88,773 athlete days
- The definitive epidemiological study: prospectively recorded medical records of the Australian Rowing Team across a full Olympiad, 151 athletes, 88,773 athlete days. 19 rib stress injuries - and note the split, 12 were bone stress REACTIONS and only 7 were frank FRACTURES.
- TIME LOST IS THE NUMBER TO KNOW, and it is longer than commonly taught: stress FRACTURE caused a median 69 days lost to full on-water training (IQR 56-157); bone stress REACTION a median 57 days (IQR 45-78). Median around 10 weeks - the authors note this is GREATER than previously published figures.
- Period prevalence varied from 4% to 15.4% between years; incidence ranged from 0.27 to 0.13 per 1000 athlete days. Incidence rose significantly in the pre-Olympic year (2015, p less than 0.001), consistent with training load driving the injury.
- The commonest injury location on imaging was the MID-AXILLARY LINE and RIB 6.
- NEGATIVE FINDINGS that matter: there were NO significant differences in prevalence by sex, by sweep versus scull, or by weight class. Cases were 12 female and 7 male, 11 open weight and 8 lightweight, 12 scull and 7 sweep.
- MRI was the most commonly used diagnostic modality and the authors recommend it as FIRST-LINE investigation.
- Limitations: a single national squad, 19 events in total, so the subgroup comparisons are underpowered - 'no difference by sex' means none was detected, not that none exists. Elite full-time athletes are not comparable to club or masters rowers.
Skeletal health and associated injury risk in collegiate FEMALE rowers
- 24 competitive collegiate FEMALE rowers versus 24 matched controls, with DXA and peripheral quantitative CT. Rib-injury comparisons were within the rowers only: 11 reporting injury versus 13 injury-free - so every within-rower finding rests on a group of about a dozen.
- IMPORTANT NEGATIVE: although rowing is generally said to be associated with low bone mass, these rowers had mostly EQUIVALENT skeletal measures to controls and their values were WITHIN NORMAL RANGES. They were taller with greater lean and less fat mass. This study therefore does not demonstrate low bone density in rowers.
- Injury-free rowers consumed over 500 mg per day more calcium than injured rowers - the clearest and most actionable difference.
- Counter-intuitively, the injury-free rowers were reported as LESS symmetrical at the 4% tibiae and hips (p less than 0.015), which sits awkwardly with the authors' own closing recommendation of balanced movement patterns; with 11 versus 13 participants this asymmetry finding should not be used to justify any clinical advice.
- The strongest predictive model of reported rib injury combined calcium intake and the hip strength index symmetry index (R-squared 0.833); a more practical model using calcium intake and bone-specific physical activity classified injury status correctly 75% of the time (R-squared 0.750).
- Limitations: cross-sectional, 48 participants total, female collegiate athletes only, and injury status was SELF-REPORTED rather than imaging-confirmed - so the outcome being predicted is a recollection of rib injury, not a verified stress fracture. These are prediction models developed in one small sample with no external validation.
The time lost (median 69 days for fracture, IQR 56-157; 57 days for stress reaction, IQR 45-78), the 12-to-7 split of reactions to fractures, the period prevalence of 4% to 15.4%, the incidence of 0.13 to 0.27 per 1000 athlete days, the mid-axillary and rib-6 location, the significant pre-Olympic-year rise, the absence of any difference by sex, sweep versus scull or weight class, and the recommendation of MRI as first-line all come from Harris (DOI) - 151 athletes of one national squad over 88,773 athlete days, with 19 events in total. The calcium-intake difference, the prediction models and the finding that these rowers' skeletal measures were within normal ranges come from Baker (DOI) - 24 collegiate female rowers, with rib-injury comparisons resting on 11 versus 13 participants and injury status self-reported. The Karlson force-couple mechanism, the first-rib subclavian-groove anatomy, the presentation, and the non-operative load-managed principles are standard, well-established teaching.
What does not exist: no validated return-to-sport criteria, no graded rehabilitation protocol tested against another, no imaging-based grading system that has been shown to predict time lost in ribs specifically, and no prospective trial of any preventive intervention. The Baker prediction equations were developed in a single small sample and have never been externally validated, so they should not be used to screen athletes. Almost all of the quantitative data above come from ELITE full-time rowers and should not be transferred unchanged to club, masters or school athletes.