The Stiffness is the Key
Etiological Classification
Critical Must-Knows
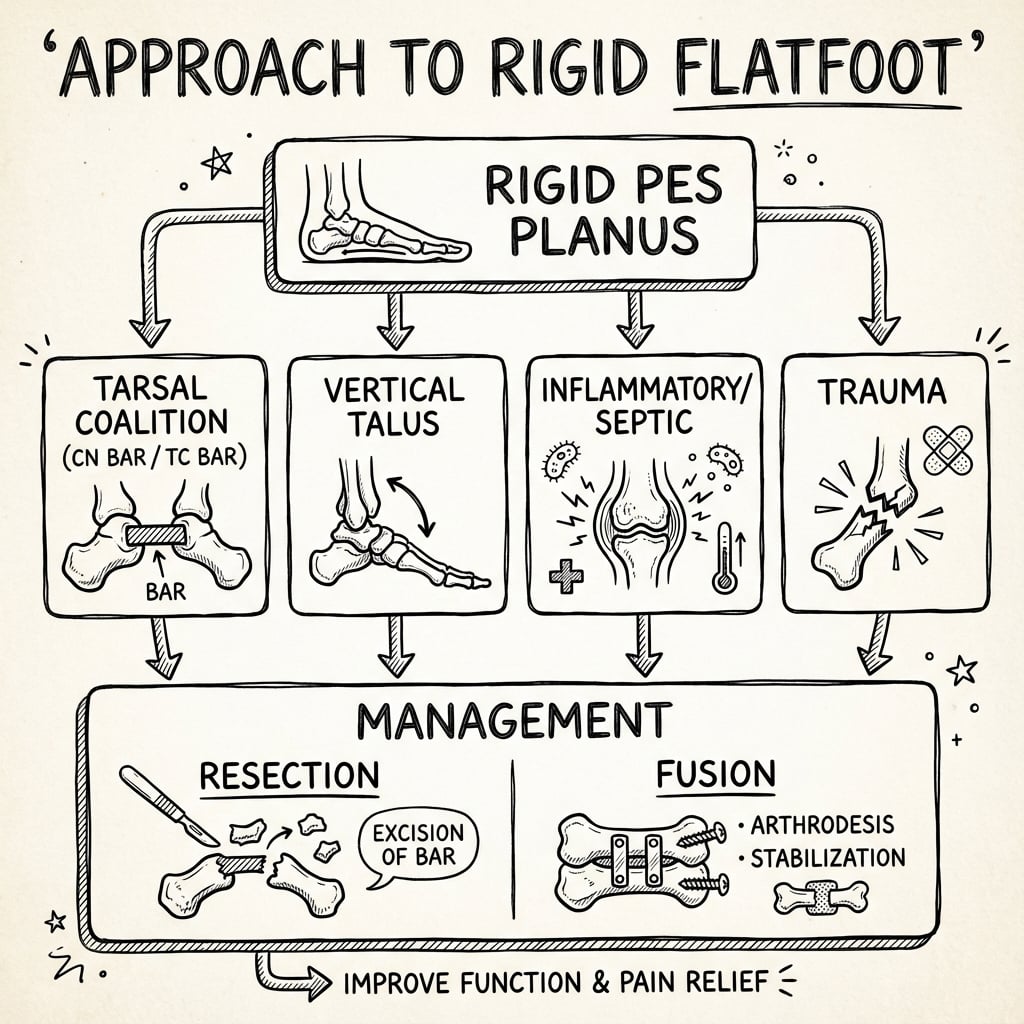
- Definition: A flatfoot with restricted subtalar motion and no arch reconstitution
- Peroneal Spastic Flatfoot: A clinical description (not a diagnosis) usually caused by Coalition
- Differential: Tarsal Coalition, Vertical Talus, Septic Arthritis, JIA, Trauma
- Workup: Weight-bearing X-rays are first line; CT is gold standard for bony coalition; MRI for fibrous
- Management: Depends on cause (Resection vs Fusion)
Clinical Pearls
- "If the heel stays in valgus when they go on tiptoes, think RIGID
- "Always check subtalar motion - if it's stiff, get a CT
- "Unilateral flatfoot is suspicious
- "Pain in the sinus tarsi or medial malleolus suggests coalition
Terminology Trap
"Peroneal Spastic Flatfoot" is a historical term describing the clinical appearance of a rigid flatfoot where the peroneal tendons are tight/spastic.
- It is NOT a diagnosis in itself.
- It is a sign of an underlying pathology (usually Tarsal Coalition).
- Do not stop at "Peroneal Spastic Flatfoot" - always find the underlying cause!
Flexible vs Rigid Flatfoot
| Feature | Flexible Flatfoot | Rigid Flatfoot (e.g. Coalition) |
|---|---|---|
| Heel Rise Test | Heel Inverts (Varus) | Heel Remains Valgus |
| Jack's Test | Arch Reconstitutes | Arch Remains Flat |
| Subtalar Motion | Normal | Restricted / Absent |
| Pain | Usually Asymptomatic | Often Painful |
| Imaging | Normal Anatomy (just flat) | Bony/Cartilaginous Abnormalities |
Differential Diagnosis of the Rigid Flatfoot
| Cause | Typical Age / Clue | Discriminating Feature | Confirmatory Test |
|---|---|---|---|
| Tarsal Coalition | Child-adolescent, recurrent sprains | C-sign / anteater nose, restricted subtalar motion | CT (bony) or MRI (fibrous) |
| Congenital Vertical Talus | Newborn, rocker-bottom sole | Irreducible dorsal navicular dislocation | Forced plantarflexion lateral X-ray |
| Septic Arthritis (subtalar) | Any age, acute, febrile | Refusal to weight-bear, raised CRP/ESR | Aspiration / MRI, washout |
| Juvenile Idiopathic Arthritis | Child, insidious, may be bilateral | Morning stiffness, synovitis, warmth | MRI synovitis, inflammatory markers |
| Osteoid Osteoma | Adolescent, night pain | Pain relieved by NSAIDs/aspirin | CT nidus |
| Tibialis Posterior Dysfunction | Adult, unilateral, progressive | Flexible early then rigid, too-many-toes sign | MRI / dynamic exam |
| Trauma (malunion / dislocation) | Any age, history of injury | Prior fracture, deformity | X-ray / CT |
CAVETCauses of Rigid Flatfoot
| C | Coalition Tarsal Coalition (TC/CN) |
| A | Arthritis JIA, Septic |
| V | Vertical Talus Congenital Vertical Talus |
| E | Exostosis/Tumor Osteoid Osteoma |
| T | Trauma Fracture malunion |
| C | Coalition Tarsal Coalition (TC/CN) | E | Exostosis/Tumor Osteoid Osteoma |
| A | Arthritis JIA, Septic | T | Trauma Fracture malunion |
| V | Vertical Talus Congenital Vertical Talus |
Hook:Don't CAVE To the rigid foot.
TCCoalition Locations
| T | Talocalcaneal Middle facet (Subtalar) |
| C | Calcaneonavicular Anterior Process to Navicular |
| T | Talocalcaneal Middle facet (Subtalar) |
| C | Calcaneonavicular Anterior Process to Navicular |
Hook:The two main bars.
ACBRadiographic Signs
| A | Anteater Nose Calcaneonavicular Coalition (Lateral view) |
| C | C-Sign Talocalcaneal Coalition (Lateral view) |
| B | Beak (Talar) Dorsal osteophyte (Traction spur) |
| A | Anteater Nose Calcaneonavicular Coalition (Lateral view) |
| C | C-Sign Talocalcaneal Coalition (Lateral view) |
| B | Beak (Talar) Dorsal osteophyte (Traction spur) |
Hook:The Zoo of Radiology.
Overview/Epidemiology
Rigid Flatfoot is a descriptive term for a foot that lacks a medial longitudinal arch and is stiff. Unlike the ubiquitous flexible flatfoot, a rigid flatfoot is almost always pathological.
The "Peroneal Spastic" Foot: Historically, this described a foot held in rigid valgus by spasm of the peroneal muscles. We now know that the peroneal spasm is usually a protective reflex to splint a painful, stiff subtalar joint (typically due to a coalition). It may also be seen in inflammatory conditions (Subtalar arthritis).
Etiology by Age:
- Infant: Congenital Vertical Talus (CVT).
- Child: Tarsal Coalition (Calcaneonavicular - ossifies earlier).
- Adolescent: Tarsal Coalition (Talocalcaneal - ossifies later).
- Any Age: Septic Arthritis, Osteomyelitis, Trauma, Tumor (Osteoid Osteoma).
Pathophysiology: Tarsal Coalition
Pathogenesis: A failure of mesenchymal segmentation during fetal development. The bar is initially cartilaginous (synchondrosis) or fibrous (syndesmosis) and allows some motion, hence why young children are asymptomatic. As the child grows and the bar ossifies (synostosis), stiffness increases, micro-fractures occur across the rigid bar during activity, and pain develops.
Natural History of Ossification:
- Calcaneonavicular (CN): Ossifies between 8-12 years. Symptoms appear at this age.
- Talocalcaneal (TC): Ossifies between 12-16 years. Symptoms appear later in adolescence.
Why does it cause Spasm? The rigid subtalar joint loses its ability to invert/evert. When walking on uneven ground, the ground reaction force attempts to invert the heel. The rigid subtalar joint cannot invert. This places stress on the peroneal muscles which fire reflexively to hold the foot in eversion (valgus) to protect the stiff joint from forced inversion stress.
Associated Anomalies:
- Fibular Hemimelia (often associated with Tarsal Coalition).
- Apert Syndrome.
- Nievergelt-Pearlman Syndrome.
Deep Dive: Congenital Vertical Talus (CVT)
Definition: Also known as "Rocker Bottom Foot". It is a dorsolateral dislocation of the talonavicular joint. The talus is locked in a vertical (plantarflexed) position, and the navicular is dislocated onto the dorsal neck of the talus. This is the hallmark of a rigid flatfoot in a newborn.
Pathoanatomy:
- Hindfoot: Severe valgus and equinus (calcaneus is plantarflexed).
- Midfoot: Dorsally dislocated.
- Forefoot: Abducted and dorsiflexed.
- Soft Tissue Contractures: Tight Achilles, Peroneals, Tibialis Anterior, and Extensor Digitorum Longus.
Etiology:
- Idiopathic: 50% of cases.
- Syndromic: 50% of cases. Highly associated with Arthrogryposis, Spina Bifida (Myelomeningocele), and Genetic Syndromes (Trisomy 13, 15, 18).
Differentiation from Oblique Talus:
- CVT: Rigid. Navicular does not reduce on plantarflexion X-ray.
- Oblique Talus: Flexible/Reducible. Navicular slides back on plantarflexion.
Deep Dive: Inflammatory and Septic Causes
Septic Arthritis of the Subtalar Joint:
- Presentation: Acute onset rigid flatfoot, refusal to bear weight, fever, elevated CRP/ESR.
- Mechanism: Pus in the joint causes severe spasm (splinting) of the surrounding muscles (Peroneals).
- Urgency: Surgical emergency requiring washout.
Juvenile Idiopathic Arthritis (JIA):
- Presentation: Insidious onset stiffness, often bilateral (but starts unilateral). Subtalar joint is a common target.
- Signs: Warmth, swelling, morning stiffness.
- Natural History: If uncontrolled, leads to spontaneous fusion (ankylosis) of the subtalar joint. This causes a permanent rigid flatfoot in adulthood.
Osteoid Osteoma:
- Classic Site: Talar neck or Subtalar joint.
- Mechanism: The tumor secretes prostaglandins which cause intense local inflammation and reflexive muscle spasm (Peroneal Spastic Flatfoot).
- Key Symptom: Night pain relieved by Aspirin/NSAIDs.
- Imaging: CT reveals the "nidus".
Detail: Coalition Resection
Pre-operative Planning:
- CT Scan: Essential. Assess the size of the coalition. Rule of thumb: if the bar involves greater than 50% of the joint surface, resection is likely to fail (instability/pain). Fusion is preferred.
- Hindfoot Valgus: If severe (greater than 15-20 degrees), resection alone won't correct alignment. Need calcaneal osteotomy.
Calcaneonavicular (CN) Bar Resection:
- Incision: Lateral oblique incision in the lines of tension skin.
- Protection: Sural nerve (posterior) and Superficial Peroneal Nerve (dorsal).
- Exposure: Elevate the Extensor Digitorum Brevis (EDB) from its origin.
- Identification: The bar is palpable between the calcaneus and navicular.
- Resection: Using an osteotome or burr. The resection must be generous (rectangular block).
- Check: Visualize the talar head (medial) and cuboid (lateral) to ensure full width resection.
- Interposition: The EDB muscle belly is sewn into the defect with absorbable suture to act as a spacer.
Talocalcaneal (TC) Bar Resection:
- Incision: Medial curvilinear incision over the sustentaculum tali.
- Protection: Tibialis Posterior tendon, FDL, FHL, and Neurovascular bundle (retract posteriorly).
- Exposure: Open the sheath of FDL/Tib Post. Identify the middle facet.
- Resection: High speed burr to remove the bony bridge.
- Safety: Do not penetrate too deeply into the posterior facet (lateral) or sinus tarsi.
- Interposition: Fat graft (from Kager's triangle or local fat) or bone wax.
Anatomy/Biomechanics
Normal Subtalar Joint: Allows inversion/eversion. Essential for accommodating uneven ground. The "Torque Converter" of the foot.
Rigid Flatfoot Pathomechanics:
- Block to Motion: A bony or cartilaginous bar (coalition) or dislocation (CVT) prevents subtalar inversion/eversion.
- Fixed Valgus: The heel is locked in valgus.
- Midfoot Unlock: Because the hindfoot cannot invert, the midfoot cannot lock (via the locking wedge mechanism of the transverse tarsal joint) to become a rigid lever for push-off.
- Peroneal Overdrive: The peroneals shorten over time or spasm to prevent painful inversion against the bar.
Tarsal Coalition Anatomy:
- Calcaneonavicular (CN): Connection between the anterior process of the calcaneus and the navicular.
- Talocalcaneal (TC): Connection typically at the middle facet of the subtalar joint.
Classification Systems
Anatomical Classification of Coalition
- Syndesmosis: Fibrous union (Stiff but maybe some motion).
- Synchondrosis: Cartilaginous union (Stiffer).
- Synostosis: Bony union (Rigid).
Detail: Advanced Classification of Coalitions
Calcaneonavicular (CN) Classifications:
- Upasani Classification:
- Type 1: Fibrous/Cartilaginous (Irregular joint line).
- Type 2: Bony (Solid bar).
Talocalcaneal (TC) Classification (Rozansky): Based on CT scan morphology and percentage of posterior facet involvement.
- Type I: Linear (straight bond).
- Type II: Linear with posterior hook.
- Type III: Shingled (overlapping).
- Type IV: Complete bony block.
- Type V: Posterior facet involvement greater than 50%. (Poor prognosis for resection).
CT Measurement Protocol:
- Coronal Plane: Best for TC coalition (Middle facet).
- Sagittal Plane: Best for C-Sign.
- Oblique/Axial: Best for CN coalition.
- Impingement Signs: Check for dorsal "beaking" on the talus (Traction spur, not OA) vs true joint space narrowing (OA). Resection is contraindicated if greater than 50% joint narrowing.
Clinical Assessment
History:
- Pain: Often "vague" ankle pain or sinus tarsi pain. Worse with activity or uneven ground.
- Sprains: Recurrent ankle sprains (because the subtalar joint can't accommodate, the ankle rolls).
- Stiffness: "My foot doesn't move like the other one."
Physical Examination:
- Look:
- Flattened arch (Pes Planus).
- Heel Valgus (Hindfoot Valgus).
- "Too Many Toes" Sign (Forefoot abduction).
- Feel:
- Tender Sinus Tarsi (CN Coalition/Arthritis).
- Tender Medial Malleolus/Sustentaculum (TC Coalition).
- Tight Peroneal Tendons (bowstringing behind lateral malleolus).
- Move:
- Subtalar ROM: Lock the talus in the mortise (dorsiflex ankle) and swing the heel. Restricted or Absent in rigid flatfoot.
- Tiptoe Test: Heel fails to invert.
- Jack's Test: Arch fails to rise.
Investigations
Plain Radiographs (Weight Bearing):
- AP Foot: "Talonavicular uncoverage".
- Lateral Foot:
- C-Sign: Continuous C-shaped line from talar dome to sustentaculum (TC Coalition).
- Anteater Nose Sign: Elongated anterior process of calcaneus (CN Coalition).
- Talar Beak: Dorsal osteophyte on talar head (traction spur from navicular capsule).
- Vertical Talus: Talus axis points to sole, Navicular dorsal.
- Harris Heel View: Special view to see the posterior and middle facets.
Advanced Imaging:
- CT Scan: Gold Standard for defining bony anatomy and mapping coalitions. Essential for surgical planning (size of bar, hindfoot valgus angle).
- MRI: Useful for Fibrous or Cartilaginous coalitions (which may be invisible on CT) and for assessing soft tissue/inflammatory causes (synovitis).
Deep Dive: The Talar Beak
Definition: A dorsal osteophyte located on the head of the talus.
Clinical Pearl: The presence of a Talar Beak is often the first clue on a lateral X-ray that the subtalar joint is stiff, even if the coalition itself is not visible. It signifies abnormal mechanics.
Pathomechanics:
- It is NOT a sign of osteoarthritis of the Talonavicular joint.
- It is a Traction Spur.
- Because the subtalar joint is rigid, the navicular overrides the talar head during dorsiflexion. This causes excessive tension on the dorsal talonavicular capsule/ligament.
- This tension pulls on the periosteum, leading to bone formation (Enthesophyte).
Radiographic Distinction:
- Talar Beak: Located proximal to the joint line. The joint space itself is preserved. Resection is still an option.
- Degenerative Spur: Located at the joint margin (lipping) and associated with joint space narrowing. Resection is contraindicated (Fusion needed).
Management Algorithm
Detail: Triple Arthrodesis
Indication: Severe rigid flatfoot with degenerative changes (arthritis) or failure of coalition resection. The "Gold Standard" salvage.
Principle: Fusion of the Talonavicular (TN), Calcaneocuboid (CC) and Subtalar (TC) joints to create a rigid, stable, plantigrade foot.
Technique (Single Incision Approach):
- Incision: Lateral Ollier's incision (extended).
- Exposure: EDB reflected. Retract peroneals plantarwards.
- Joint Prep (Resection):
- CC Joint: Resect cartilage to bleeding bone.
- Subtalar Joint: Resect posterior and anterior facets. Remove the coalition.
- TN Joint: Exposed from lateral side (challenging) or separate medial incision. Remove cartilage.
- Correction:
- Reduce the Talonavicular joint first (key to alignment).
- Correct Valgus at the Subtalar joint.
- Correct Abduction at the CC joint.
- Fixation:
- Subtalar: large screw (6.5mm/7.0mm) from heel to talus.
- TN: screws or staples.
- CC: screws or staples.
- Closure: Layered closure over a drain.
Algorithm:
- Position: Supine, sandbag under ipsilateral hip.
- Tourniquet: Thigh.
- Post-op: NWB for 6-12 weeks until union.
Surgical Technique
Calcaneonavicular Bar Excision
Approach: Lateral Ollier's incision (over sinus tarsi). Technique:
- Identify Extensor Digitorum Brevis (EDB).
- Reflect EDB distally.
- Identify the bar between Anterior Calcaneus and Navicular.
- Resect the bar thoroughly (rectangular block).
- Check motion (should improve immediately).
- Interposition: Sew the EDB belly into the defect to prevent regrowth.
Complications
| Complication | Risk Factors | Prevention/Management |
|---|---|---|
| Recurrence of Coalition | Inadequate resection, no interposition. | Prevention: Generous resection and EDB/Fat interposition. |
| Persistent Pain | Missed second coalition, underlying arthritis. | Prevention: Pre-op CT to scan whole foot. Management: Fusion. |
| Sural Nerve Injury | Lateral approach. | Prevention: Identify and protect. |
| Wound Dehiscence | Medial approach (TC coalition). | Prevention: Careful handling of skin. |
| Arthrofibrosis | Prolonged immobilization. | Prevention: Early ROM if stable. |
Postoperative Care
For Coalition Resection:
- Weeks 0-2: Splint/Cast, Non-Weight Bearing (NWB). Elevate significantly to prevent wound breakdown.
- Weeks 2-6:
- Motion: Start active ROM exercises (writing alphabet with foot).
- Physio: Focus on peroneal strengthening and subtalar eversion/inversion.
- Weight: Touch down weight bearing in a boot.
- Weeks 6+:
- Weight bearing as tolerated in shoes.
- Continue physio for 3-6 months.
- Return to sport at 3-4 months.
For Fusion (Triple Arthrodesis):
- Weeks 0-2: Backslab, strictly NWB. Elevation.
- Weeks 2-6: Conversion to lightweight fibreglass cast or CAM boot (locked). Still NWB to protect the fusion mass.
- Weeks 6-12:
- Progressive weight bearing in CAM boot.
- X-ray at 6 weeks to check alignment.
- X-ray at 12 weeks to confirm union.
- Months 3-6:
- Wean out of boot into stiff-soled shoe.
- Gait retraining (expect stiff gait).
- No impact sports.
Complications of Rehab:
- CRPS (Complex Regional Pain Syndrome): High risk in foot surgery. Early movement and desensitization are key prevention strategies. Vitamin C 500mg daily is often prescribed.
- Stiffness: Failure to mobilize after resection leads to fibrosis.
Outcomes/Prognosis
- Tarsal Coalition:
- Resection yields good results in young patients (~75-80% relief).
- Poorer results in older patients or large bars.
- Vertical Talus:
- Dobbs technique gives excellent functional results and avoids stiff, small feet associated with extensive releases.
- Untreated Rigid Flatfoot:
- Leads to progressive degenerative arthritis of the triple joint complex.
- May require Triple Arthrodesis in adulthood.
Evidence Base
- 11 patients (19 feet) with idiopathic congenital vertical talus, minimum 2-year follow-up
- Serial reverse-Ponseti casts (mean 5) then talonavicular pinning plus percutaneous Achilles tenotomy; no extensive releases needed
- Initial correction achieved in all 19 feet; recurrence in 3 feet - all of which had NOT had talonavicular pin fixation
- 24 children treated with the minimally invasive (Dobbs) method; radiographic recurrence in 7 (29%)
- Mean PROMIS scores within 1 SD of the reference population for pain interference, mobility and peer relations
- Children who started treatment after 12 months of age had significantly lower mobility scores
- 24 patients (32 resections: 19 calcaneonavicular, 13 talocalcaneal), mean follow-up to age 25-27 years
- CN and TC resections produced similar long-term function and satisfaction scores
- Favourable results were attained even for TC coalitions over 50% of the posterior facet and hindfoot valgus over 16 degrees
- 8 patients (13 painful talocalcaneal coalitions) treated with calcaneal lengthening osteotomy, with or without resection
- Osteotomy corrected valgus and relieved pain even when the coalition was unresectable, preserving talonavicular/calcaneocuboid motion
- All feet underwent concurrent gastrocnemius or Achilles lengthening
- 78 patients / 97 coalition resections (49 talocalcaneal, 47 calcaneonavicular, plus rarer types)
- Mean return to desired activity 18.3 weeks; mean post-operative Roles & Maudsley score 1.3 (excellent/good)
- Most patients returned to their desired activity level after excision
- 100 cadaver feet dissected after spiral CT: non-osseous coalition prevalence 12.7% (CN most common single type, 9.1%)
- True prevalence is far higher than the classically quoted under 1%, because most coalitions are asymptomatic
- Spiral CT detected only ~55% of coalitions and missed 4 non-osseous bars
- 27 adults (31 feet) with non-paralytic disease, mean 14-year follow-up; 93% satisfied with the result
- Severe adjacent-joint arthrosis developed in the ankle (7 ankles), naviculocuneiform and tarsometatarsal joints; 3 later needed ankle fusion
- 74% reported moderate-to-severe difficulty on uneven ground; SF-36 physical score well below the population mean
Surgical Tips and Tricks
For Coalition Resection:
- Headlight: Essential for visualization, especially medial approach.
- Bone Wax: Use liberally on the raw bone surfaces after resection to prevent hematoma and re-ossification.
- Fat Graft: Don't skimp. Harvest a large plug from the Kager's triangle (retro-calcaneal fat pad). It has a robust blood supply.
- Intra-op Fluoroscopy: Use it to confirm the amount of bone removed. The "Harris Line" (middle facet) must be clear.
- Dynamic Check: After resection, the subtalar motion should return immediately. If it's still stiff, you haven't taken enough bone, or there's another coalition.
For Triple Arthrodesis:
- Order of Fixation:
- Talonavicular (TN): This sets the version of the foot. Reduce this first.
- Subtalar (TC): Corrects the valgus/varus.
- Calcaneocuboid (CC): Follows the others.
- Screw Position:
- Subtalar screw should aim for the talar dome but NOT penetrate it.
- TN screws should be placed from navicular into talar head (or vice versa), avoiding the joint surface.
- Bone Graft: Use local autograft from the resected wedges to pack the fusion sites.
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Rigid Teenager
"13-year-old boy, recurrent ankle sprains, painful flat feet. Exam shows restricted subtalar motion."
This is the classic presentation of a Tarsal Coalition. The rigid flatfoot predisposes to sprains because the subtalar joint cannot accommodate ground reaction forces. I would order weight-bearing ankle/foot X-rays looking for the C-sign or Anteater sign. If X-rays are inconclusive but suspicion is high, a CT scan is the next step.
Infant with Rocker Bottom
"Newborn with a rigid flatfoot, convex sole (Rocker Bottom). Top of foot touches shin."
This is likely Congenital Vertical Talus (CVT). The differential includes Oblique Talus or posterior medial bowing. I would examine for reducibility of the navicular (rigid in CVT). I would also check the spine for neural tube defects and hips. Diagnosis is confirmed with a forced plantarflexion lateral X-ray showing the talar axis remaining vertical and dislocated.
The Unilateral Flatfoot
"35-year-old male, sudden onset painful unilateral flatfoot. No trauma. History of 'minor' sprains."
Sudden onset unilateral rigid flatfoot in an adult is worrying. It could be **Tibialis Posterior Tendon Dysfunction (TPTD)** (usually flexible initially then rigid), or it could be a previously asymptomatic **coalition** that has become symptomatic due to a micro-fracture or degeneration. Other causes include inflammatory arthritis or tumor. I would start with X-rays and likely proceed to MRI to assess the tendon and joint surfaces.
MCQ Practice Points
Radiology MCQ
Q: The 'Anteater Nose' sign is pathognomonic for which condition? A: Calcaneonavicular Coalition. It represents the elongated anterior process of the calcaneus.
Anatomy MCQ
Q: Which facet is most commonly involved in Talocalcaneal coalitions? A: Middle Facet. It is often hard to see on standard lateral views (requires Harris view or CT).
Management MCQ
Q: What is the primary contraindication to coalition resection? A: Degenerative Changes (Arthritis) in the subtalar or talonavicular joint. If arthritis is present, resection will fail; fusion is required.
Clinical MCQ
Q: What is the characteristic finding of Peroneal Spastic Flatfoot? A: Rigid Valgus that does not correct on tiptoeing, with tight/bowstrung peroneal tendons.
Imaging MCQ
Q: What is the gold standard imaging for diagnosing Talocalcaneal coalition? A: CT Scan. It best demonstrates bony anatomy and the extent of the coalition (less than 50% = resection, greater than 50% = fusion).
Surgical MCQ
Q: What tissue is interposed after calcaneonavicular coalition resection? A: Extensor Digitorum Brevis (EDB) muscle belly. This prevents bony regrowth and maintains the resection gap.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Tarsal coalition: Classically quoted at under 1% symptomatic prevalence, but cadaver/CT studies show non-osseous coalition in roughly 11-13% of feet - most are asymptomatic. Bilateral in 50-60%. Calcaneonavicular and talocalcaneal account for the vast majority; up to 20% of patients have more than one coalition.
- Congenital vertical talus: Rare (around 1 in 10,000 live births). Roughly half are syndromic (arthrogryposis, myelomeningocele, chromosomal anomalies).
Side-by-Side Practice (no single national framework):
| Theme | Convergent global practice | Where opinion still differs |
|---|---|---|
| First-line imaging | Weight-bearing radiographs for every rigid flatfoot | CT vs MRI as the next study (CT for bony mapping; MRI better for fibrous/cartilaginous bars and marrow oedema) |
| CVT correction | Minimally invasive reverse-Ponseti (Dobbs) method is now the international standard of care | Role and extent of soft-tissue release in non-idiopathic/syndromic feet |
| Coalition surgery | Resection + interposition for symptomatic, non-arthritic bars | The 50% posterior-facet "rule" - newer data (Khoshbin) suggest larger TC bars can still do well |
| Deformity | Address hindfoot valgus, not just the bar | Calcaneal lengthening osteotomy vs subtalar/triple fusion for severe valgus |
High- vs Limited-Resource Settings:
- Well-resourced: Routine CT/MRI, motion-preserving reconstruction (resection plus lengthening osteotomy), early Dobbs-method CVT casting in infancy.
- Limited-resource: Diagnosis often delayed to symptomatic adolescence or neglected CVT; reliance on plain films; later presentation shifts the balance toward arthrodesis/salvage. Naviculectomy with limited release has been described as an affordable "third way" for neglected/complex CVT.
- Registries: There is no dedicated coalition or CVT registry; evidence is drawn from single-centre series and small cohorts, which is itself a key limitation (see Controversies).
Controversies & Areas of Uncertainty
- The 50% posterior-facet rule: The traditional teaching that talocalcaneal coalitions involving over 50% of the posterior facet require fusion rather than resection is being challenged. Khoshbin et al. found favourable long-term outcomes after resecting TC bars exceeding 50% of the facet with hindfoot valgus over 16 degrees, and Mosca's calcaneal lengthening offers a motion-preserving alternative even for "unresectable" coalitions.
- Treat the deformity or the bar?: Resecting the coalition without correcting fixed hindfoot valgus can leave a painful, poorly aligned foot. There is no consensus on the valgus threshold mandating an added calcaneal lengthening osteotomy versus resection alone.
- Interposition material: EDB, fat graft, bone wax and tendon have all been used to prevent reossification after resection; no high-level comparative evidence establishes one as superior.
- Pinning in CVT: Dobbs' own series showed recurrence only in feet that were NOT pinned, but the optimal duration of talonavicular K-wire fixation and casting is not standardised.
- Asymptomatic coalition: Whether an incidentally discovered coalition should ever be resected prophylactically (e.g. in a young athlete) remains unresolved - current practice treats symptoms, not the radiograph.
- Evidence quality: Nearly all data are Level III-IV retrospective series from single centres with no registry; there are no randomised trials comparing resection strategies or CVT techniques.
Parent's Guide: Frequently Asked Questions
Q: Will my child grow out of it? A: Unlike flexible flatfeet (which often improve), a rigid flatfoot (Tarsal Coalition) is a structural problem. The "bar" between the bones will not disappear. Symptoms might fluctuate, but the stiffness remains.
Q: Is surgery always needed? A: No. If the foot is not painful, we leave it alone. We treat the symptoms, not the X-ray. Many adults have coalitions they don't know about.
Q: Can they play sports after surgery? A: Yes. After resection, most children return to sports. If a fusion (Triple Arthrodesis) is performed, high-impact sports (running, soccer) may be difficult, but cycling and swimming are excellent.
Q: Why is the cast on for so long? A: To allow the swelling to settle (after resection) or to allow the bones to knit together (after fusion). Rushing rehabilitation can lead to persistent pain.
RIGID FLATFOOT
Clinical summary
DEFINITION
- •Restricted Subtalar Motion
- •No Arch Reconstitution
- •Fixed Valgus
- •Peroneal Spasm (Reactive)
DIFFERENTIAL
- •Tarsal Coalition
- •Vertical Talus
- •Arthritis (Septic/JIA)
- •Trauma
- •Tumor
WORKUP
- •Tip-Toe Test
- •Jack's Test
- •X-ray (C-sign, Anteater)
- •CT (Gold Standard for Bone)
MANAGEMENT
- •Symptomatic: Resection
- •Arthritic/Large: Fusion
- •Infant (CVT): Casting + Pinning
- •Always rule out 2nd coalition
RED FLAGS
- •Unilateral
- •Night Pain (Tumor)
- •Systemic Symptoms (Sepsis)
- •Fever / Elevated CRP