Fatigue Failure | Pseudarthrosis Association | Long Construct Risk
Rod Fracture Classification
Critical Must-Knows
- Pseudarthrosis is the dominant cause - without solid fusion the rod bears the entire cyclic load and fails by fatigue
- Pedicle subtraction osteotomy (PSO) is the single highest-risk site (rod fracture up to ~40% in some series)
- Cobalt-chrome rods fracture less than titanium (meta-analysis), at the cost of higher proximal junctional kyphosis
- Accessory rods across an osteotomy reduce rod fracture/pseudarthrosis - but simply adding rods elsewhere is not reliably protective
Clinical Pearls
- "Rod fracture = fatigue failure - the rod alone cannot sustain cyclic loading
- "CT is gold standard for fusion assessment - less than 50% bridging = pseudarthrosis
- "Symptomatic fracture with pseudarthrosis must revise - will progress without fusion augmentation
- "Address root cause: fusion, alignment, and biomechanics - not just bigger rods
Rod Fractures in Spinal Instrumentation
Clinical Warning
Biomechanical Complication: Rod fracture indicates construct failure, usually from underlying pseudarthrosis. Examiners expect understanding of fatigue failure principles, ability to differentiate observation versus revision candidates, and comprehensive revision strategy addressing both biomechanics AND biology.
At a Glance
Essential Mnemonics
FRACTUREHigh-Risk FRACTURE Criteria
| F | Fusion length Greater than FIVE levels |
| R | Rod diameter REDUCED (5.5mm) |
| A | Alignment Not corrected (positive SVA) |
| C | Connectors Offset or cross-links inadequate |
| T | Titanium Rods in long construct |
| U | Under-fixed Sacrum (no iliac screws when needed) |
| R | Revision Surgery |
| E | Elderly With osteoporosis |
| F | Fusion length Greater than FIVE levels | C | Connectors Offset or cross-links inadequate | R | Revision Surgery |
| R | Rod diameter REDUCED (5.5mm) | T | Titanium Rods in long construct | E | Elderly With osteoporosis |
| A | Alignment Not corrected (positive SVA) | U | Under-fixed Sacrum (no iliac screws when needed) |
Hook:Three or more FRACTURE criteria = very high risk requiring aggressive preventive strategies
Overview
Rod fractures are a biomechanical complication representing fatigue failure of spinal instrumentation under cyclic loading. They occur in roughly 2-26% of spinal fusions, with incidence directly related to construct length, three-column osteotomy, and residual sagittal malalignment.
Epidemiology:
- Incidence: low single digits for short segment fusions (1-3 levels); 18-26% in long adult deformity constructs incorporating a pedicle subtraction osteotomy
- Pedicle subtraction osteotomy is the highest-risk osteotomy, with the osteotomy site the dominant fracture location
- Peak occurrence: typically 12-36 months postoperatively (mean time to distal junctional failure ~32 months)
- Strong association with pseudarthrosis - without solid fusion the rod bears load without biological support
- Higher rates in revision surgery compared to primary
Key Anatomical Sites:
- Lumbosacral junction: Highest stress zone due to moment arm and motion
- Rod-connector junctions: Stress concentration from offset connectors
- Three-column osteotomy sites: High mechanical demands
- Transition zones: Between rigid fusion mass and mobile spine
Clinical Significance:
- Often indicates underlying pseudarthrosis (fusion failure)
- May be incidental finding or cause significant symptoms
- Symptomatic cases with pseudarthrosis require revision surgery
- Reported rates are consistent across international deformity series
Pathophysiology
Biomechanical Principles
Rod fractures represent fatigue failure under cyclic loading conditions. The basic principles include:
Stress Concentration Sites:
- Rod-connector junctions (offset connectors create bending moments)
- Tulip-rod interface (stress riser from pedicle screw clamp)
- Cross-link attachment points
- Rod bends or contouring sites (cold working creates microcracks)
- Transition zones between fused and mobile segments
Material Properties:
- Cobalt-chromium alloys: higher strength but lower ductility than titanium
- Titanium alloys: more ductile but lower fatigue strength
- Rod diameter: 5.5mm rods more prone to fracture than 6.0mm or 6.35mm
- Larger diameter rods reduce stress but increase stiffness
Loading Conditions:
- Cantilever bending in long constructs
- Cyclic loading from physiologic motion
- Increased loads in pseudarthrosis (rod bears entire load)
- Sagittal imbalance increases rod stress
Pathophysiology of Rod Failure
Three-Stage Failure Process:
- Crack Initiation: Microcrack formation at stress concentrations
- Crack Propagation: Cyclic loading extends crack through rod cross-section
- Final Fracture: Sudden failure when remaining cross-section cannot sustain load
Relationship to Pseudarthrosis:
- Rod fracture often indicates underlying pseudarthrosis
- Solid fusion protects rods by load-sharing
- In pseudarthrosis, rod bears 100% of load (no biological load-sharing)
- Rod fracture may occur before radiographic evidence of pseudarthrosis visible
High-Risk Anatomical Scenarios
Long Constructs:
- Adult deformity surgery (greater than 5 levels)
- Thoracolumbar kyphosis correction
- Sacropelvic fixation constructs
Transition Zones:
- Lumbosacral junction (high moment arm)
- Thoracolumbar junction (change from stiff thoracic to mobile lumbar spine)
- Upper instrumented vertebra (UIV) in long constructs
Sagittal Imbalance:
- Positive sagittal vertical axis increases rod stress
- Loss of lumbar lordosis increases flexion moments
- Flatback deformity dramatically increases rod loading
Classification
Practical (Descriptive) Classification of Rod Fractures
There is no universally adopted eponymous classification for rod fractures. In practice they are categorised by the status of the underlying fusion, alignment, and neurology, because this is what drives the decision to observe versus revise. The descriptive framework below is widely used in exam answers.
Rod Fracture Classification by Fusion/Alignment Status
| category | characteristics | biomechanics | treatment | prognosis |
|---|---|---|---|---|
| Type I - Isolated Rod Fracture | Single rod fracture, solid fusion, normal alignment | Low stress, likely manufacturing defect or trauma | Observation if asymptomatic, revision if symptomatic | Excellent, rarely requires intervention |
| Type II - Rod Fracture with Pseudarthrosis | Rod fracture with radiographic pseudarthrosis | Fatigue failure from repetitive loading without biological support | Revision fusion with augmentation | Good with revision, high recurrence if not revised |
| Type III - Rod Fracture with Deformity Progression | Rod fracture with loss of correction (kyphosis, translation) | Construct failure with progressive deformity | Urgent revision with osteotomy if needed | Moderate, depends on deformity magnitude |
| Type IV - Rod Fracture with Neurological Compromise | Rod fracture with new or progressive neurological deficit | Instability causing neural compression | Urgent/emergent revision surgery | Variable, depends on neural recovery |
Anatomical Location Classification
Proximal Junction (UIV ± 2 levels):
- Often associated with proximal junctional kyphosis
- High cantilever bending moments
- May require cranial extension of construct
Mid-Construct:
- Typically at connector sites or cross-links
- Suggests biomechanical design flaw
- May indicate inadequate rod size
Distal Junction (LIV ± 2 levels):
- Common in lumbosacral constructs
- High risk with inadequate sacropelvic fixation
- Often requires iliac screw augmentation
Temporal Classification
Early (Less than 1 year):
- Suggests technical error or manufacturing defect
- Consider inadequate rod size or contouring trauma
- Evaluate for infection
Late (Greater than 1 year):
- Typical fatigue failure pattern
- High association with pseudarthrosis
- Result of chronic biomechanical overload
Clinical Presentation
History
Classic Presentation:
- Initial pain relief following index surgery
- Pain-free interval (months to years)
- Sudden onset or gradual recurrence of back pain
- Mechanical pain (worse with activity, better with rest)
- May report audible "snap" or sudden sharp pain
Red Flag Symptoms:
- New radicular pain or weakness
- Progressive deformity (visible trunk shift)
- Loss of function or mobility
- Constitutional symptoms (fever, weight loss suggesting infection)
Physical Examination
Inspection:
- Assess global sagittal alignment (plumb line from C7 to sacrum)
- Evaluate for coronal decompensation (trunk shift)
- Look for visible step-off or gibbus deformity
- Check for wound healing issues or drainage
Palpation:
- Tenderness over rod fracture site
- Palpable step-off in subcutaneous patients
- Assess for fluid collection or warmth
Range of Motion:
- Often restricted due to pain
- Paradoxical increased motion at fracture site
- Functional assessment (gait, sit-to-stand)
Neurological Examination:
- Complete motor examination (L2-S1 myotomes)
- Sensory examination for dermatomal deficits
- Reflexes and pathological signs
- Sphincter tone if cauda equina suspected
Differential Diagnosis
Differential Diagnosis of Post-Fusion Pain
| category | keyFeatures | imaging | management |
|---|---|---|---|
| Rod Fracture | Sudden onset after pain-free interval, mechanical pain | Radiographs show rod discontinuity | Revision if symptomatic with pseudarthrosis |
| Pseudarthrosis Without Rod Fracture | Persistent or recurrent pain, no specific onset | CT shows lack of bridging bone, intact rods | Revision fusion with biologics |
| Adjacent Segment Disease | Pain at unfused levels, radicular symptoms | Degeneration at adjacent disc levels | Conservative vs extension of fusion |
| Infection | Constitutional symptoms, elevated inflammatory markers | MRI shows fluid collections, bone destruction | Antibiotics, debridement, retention vs removal |
| Screw Loosening | Mechanical pain, lucency around screws | Greater than 1mm radiolucency around screws | Revision with longer screws or cement augmentation |
Investigations
Radiographic Assessment
Standing Radiographs (Essential):
- AP and Lateral Full-Length Spine: Assess global alignment
- Identify Rod Fracture: Look for discontinuity, offset, or angulation
- Sagittal Parameters: SVA, PI-LL mismatch, pelvic tilt
- Coronal Parameters: Coronal vertical axis, Cobb angles
- Hardware Assessment: Screw position, connector integrity
Key Radiographic Signs:
- Rod offset or step-off
- Radiolucent line through rod (complete fracture)
- Angulation at fracture site
- Loss of correction (increased kyphosis)
- Screw haloing (greater than 1mm lucency suggests loosening)
Advanced Imaging
CT Scan with Metal Artifact Reduction:
- Gold Standard for Fusion Assessment: Evaluate bridging bone
- Identify Pseudarthrosis: Less than 50% fusion mass indicates non-union
- Hardware Integrity: Assess all rods, connectors, screws
- Bone Quality: Hounsfield units for osteoporosis assessment
- Fracture Characterization: Determine if partial or complete
MRI (Selected Cases):
- Evaluate for infection if suspected
- Assess neural compression if new radiculopathy
- Identify epidural fluid collections
- Limited by metal artifact but newer sequences (MARS) improving
SPECT-CT (Selected Cases):
- Functional assessment of fusion
- Hot spots indicate ongoing stress or non-union
- Helpful in equivocal cases
- Not routinely required
Laboratory Assessment
Baseline Tests:
- CRP and ESR: Elevated suggests infection
- Full Blood Count: Leukocytosis suggests infection
- Bone Health: Vitamin D, calcium, PTH if osteoporotic
- Metabolic Panel: Assess for medical optimization
If Infection Suspected:
- Blood cultures if systemic sepsis
- Aspiration with culture and sensitivity
- Cell count and differential (greater than 3000 WBCs, greater than 80% PMNs)
- Consider biofilm-disrupting techniques
Risk Factors
Patient Factors
Biomechanical Risk Factors:
- High BMI (greater than 30 kg/m²)
- Positive sagittal imbalance (SVA greater than 50mm)
- Severe coronal decompensation
- Poor bone quality (osteoporosis, osteopenia)
- Smoking (impairs fusion, increases pseudarthrosis risk)
Medical Comorbidities:
- Diabetes mellitus
- Chronic kidney disease
- Nutritional deficiency (vitamin D, protein)
- Immunosuppression
- Revision surgery (higher failure rates)
Surgical Factors
Construct Design:
- Long constructs (greater than 5 levels): exponentially increased risk
- Small diameter rods (5.5mm vs 6.35mm)
- Single rod constructs (unilateral fixation)
- Inadequate sacropelvic fixation in lumbosacral constructs
- Offset connectors (create bending moments)
Technical Factors:
- Excessive rod contouring (cold working weakens material)
- Sharp bends in rods (stress concentrations)
- Inadequate fusion mass (poor graft technique)
- Undercorrection of sagittal imbalance
- Use of titanium rods in long constructs (lower fatigue strength)
Biological Factors:
- Pseudarthrosis (strongest predictor of rod fracture)
- Inadequate biological supplementation (BMP, autograft)
- Infection (inhibits fusion)
- Postoperative complications (wound issues, prolonged immobility)
Evidence-Based Risk Stratification
Stratify each patient against three independent axes; the more boxes ticked, the more aggressive the preventive strategy:
- Construct/technique: long fusion to pelvis, three-column osteotomy (especially PSO), titanium rather than cobalt-chrome rods, no supplemental rod across an osteotomy
- Alignment: residual PI-LL mismatch, positive sagittal vertical axis, undercorrection (or, paradoxically, large acute correction concentrating stress at one level)
- Biology: osteoporosis/low Hounsfield units, smoking, diabetes, malnutrition, prior pseudarthrosis or revision
A patient with all three (e.g. an osteoporotic smoker undergoing a lumbar PSO with single titanium rods and residual malalignment) sits at the extreme of risk and warrants cobalt-chrome plus accessory rods, sacropelvic fixation, anterior column support, and bone-health optimisation.
Management
Non-Operative Management
Indications for Conservative Treatment:
- Isolated rod fracture with solid fusion (Type I)
- Asymptomatic patient
- No deformity progression
- No neurological compromise
- Medical contraindication to surgery
Conservative Protocol:
- Immobilization: TLSO brace for 12 weeks
- Activity Modification: Avoid heavy lifting, high-impact activities
- Pain Management: NSAIDs, acetaminophen, neuropathic agents
- Physical Therapy: Core strengthening once acute pain resolves
- Surveillance: Serial radiographs every 6 weeks for 3 months, then every 3 months
Expected Outcomes:
- Approximately 60-70% of Type I fractures remain asymptomatic
- 30-40% progress to symptomatic requiring revision
- Monitor for loss of correction or pseudarthrosis development
Operative Management
Indications for Revision Surgery:
- Symptomatic rod fracture (persistent pain limiting function)
- Rod fracture with pseudarthrosis (Type II)
- Progressive deformity (Type III)
- Neurological compromise (Type IV)
- Multiple rod fractures
- Infection
Surgical Planning Principles:
-
Identify and Address Root Cause:
- Achieve solid fusion if pseudarthrosis present
- Correct sagittal/coronal imbalance
- Optimize bone quality
- Treat infection if present
-
Enhance Construct Biomechanics:
- Upgrade to larger diameter rods (6.0mm or 6.35mm)
- Consider dual rods or satellite rods
- Add or optimize cross-links (reduce torsional stress)
- Extend fixation if junctional failure
- Add iliac screws for sacropelvic constructs
-
Maximize Biological Environment:
- Use osteobiologics (iliac crest autograft, BMP, allograft)
- Optimize nutrition and bone health preoperatively
- Smoking cessation minimum 6 weeks prior
- Treat osteoporosis (bisphosphonates, teriparatide)
Revision Surgical Techniques:
Revision Strategy by Fracture Type
| category | approach | technique | augmentation | biologics | expectedOutcome |
|---|---|---|---|---|---|
| Type I - Isolated Fracture, Solid Fusion | Focal revision at fracture site | Exchange fractured rod, retain well-fixed screws | Upgrade rod diameter, add cross-link | Local bone graft if exposed | Excellent, greater than 90% success |
| Type II - Fracture with Pseudarthrosis | Comprehensive revision of non-union | Expose pseudarthrosis, decorticate, remove fibrous tissue | Larger rods, extend fixation 1 level each direction | Structural autograft + BMP | Good, 75-85% fusion rate |
| Type III - Fracture with Deformity | Full construct revision with realignment | Osteotomy if needed (PSO, VCR), complete revision | Dual rods, satellite rods, iliac screws | Maximum biological supplementation | Moderate, 60-75% success, higher complication rate |
| Type IV - Fracture with Neuro Deficit | Urgent revision with decompression | Neural decompression, stabilization, realignment | Robust fixation with dual rods | Autograft and BMP | Variable, neural recovery unpredictable |
Technical Considerations:
Rod Selection:
- Cobalt-chromium for high-stress constructs (better fatigue resistance)
- Diameter: minimum 6.0mm, preferably 6.35mm for long constructs
- Dual/accessory rods unload the primary rods and add redundancy (most protective when placed across an osteotomy site)
- Pre-contoured rods preferred to minimize cold working
Connector Strategy:
- Side-to-side connectors preferred over offset connectors
- Place connectors away from maximum stress points
- Cross-links at every 3-4 levels in long constructs
- Ensure connectors fully seated and tightened
Sacropelvic Fixation:
- Bilateral iliac screws for constructs extending to sacrum
- S2 alar-iliac screws as alternative to traditional iliac screws
- Sacral augmentation with cement in osteoporotic bone
- Four-rod technique (dual rods to S1, dual rods to ilium) for maximum rigidity
Bone Grafting:
- Autograft from iliac crest (gold standard for posterior fusion)
- Allograft for bulk (structural support)
- BMP-2 (off-label for posterior fusion, 1.5mg/mL concentration)
- Local bone graft from decompression or decortication
- Avoid anterior column support in revision (minimizes morbidity)
Postoperative Management
Immobilization:
- TLSO brace for 12 weeks in high-risk revisions
- No brace if robust construct and solid fixation
- Early mobilization with physical therapy
Activity Restrictions:
- No bending, lifting, or twisting for 12 weeks
- Gradual return to activities at 3-6 months
- High-impact activities avoided until fusion confirmed
Surveillance Protocol:
- 6 weeks: Radiographs, wound check, pain assessment
- 12 weeks: Radiographs, discontinue brace if appropriate, advance PT
- 6 months: Radiographs, CT if fusion unclear
- 1 year: Radiographs, CT to confirm fusion
Optimization:
- Vitamin D supplementation (target greater than 30 ng/mL)
- Calcium 1200mg daily
- Osteoporosis treatment (bisphosphonates or teriparatide)
- Smoking cessation permanently
- Optimize BMI and nutrition
Complications
Recurrent Rod Fracture
Incidence: 5-15% after revision surgery
Risk Factors:
- Persistent pseudarthrosis
- Inadequate construct augmentation
- Uncorrected sagittal imbalance
- Continued smoking
- Osteoporosis not treated
Management:
- Re-revision with maximum biological and mechanical augmentation
- Consider anterior column support (ALIF, LLIF)
- Dual rods mandatory
- Extended immobilization
Infection
Risk: 3-8% in revision spine surgery (higher than primary)
Prevention:
- Preoperative optimization (glycemic control, nutrition)
- Antibiotic prophylaxis (cefazolin 2g, vancomycin if MRSA risk)
- Meticulous surgical technique (minimize tissue trauma, dead space)
- Closed suction drainage
- Prophylactic negative pressure wound therapy in high-risk patients
Management:
- Early infection (less than 3 months): debridement, irrigation, retention of hardware
- Late infection (greater than 3 months): staged revision (removal, antibiotics, reconstruction)
- Biofilm-resistant antibiotics (rifampin for staphylococci)
Proximal Junctional Kyphosis (PJK)
Incidence: 20-40% in adult deformity surgery, increased in revisions
Risk Factors:
- Overcorrection of lumbar lordosis
- UIV at inflection point (T10-L1)
- Osteoporosis
- Rod fracture creating cantilever stress
Prevention:
- Gradual lordosis transition at UIV
- Prophylactic vertebroplasty at UIV and UIV+1
- Tether augmentation at UIV
- Avoid fusion to T10 (extend to T9 or stop at T11)
Management:
- Asymptomatic: observation
- Symptomatic or progressive (greater than 20 degrees): revision with cranial extension
Neurological Injury
Risk: 1-3% in revision surgery
Types:
- Nerve root injury from screw misplacement
- Cauda equina from canal compromise
- Epidural hematoma
Prevention:
- Intraoperative neuromonitoring (SSEPs, MEPs)
- Triggered EMG for pedicle screw placement
- Meticulous technique during decompression
- Postoperative drain management
Management:
- Immediate recognition and intervention
- Revision decompression if hardware-related
- Steroids controversial (no proven benefit, potential harm)
Complications Table
Revision Surgery Complications
| category | incidence | riskFactors | prevention | management |
|---|---|---|---|---|
| Recurrent Rod Fracture | 5-15% | Persistent pseudarthrosis, inadequate augmentation | Robust construct, biologics, osteoporosis treatment | Re-revision with maximum augmentation |
| Deep Infection | 3-8% | Diabetes, obesity, revision surgery, prolonged OR time | Prophylactic antibiotics, negative pressure dressing | Early: I&D with retention; Late: staged revision |
| Proximal Junctional Kyphosis | 20-40% | Osteoporosis, overcorrection, UIV at inflection point | Prophylactic vertebroplasty, gradual lordosis transition | Observation vs cranial extension if symptomatic |
| Neurological Deficit | 1-3% | Revision surgery, deformity correction, epidural scarring | Neuromonitoring, triggered EMG, meticulous technique | Urgent exploration and decompression |
| Medical Complications | 10-20% | Age greater than 65, comorbidities, long OR time | Preoperative optimization, DVT prophylaxis | Multidisciplinary medical management |
Prognosis and Outcomes
Expected Outcomes
Successful Revision (Fusion Achieved):
- Pain Relief: 70-80% significant improvement in VAS scores
- Function: 60-70% return to baseline or improved function
- Fusion Rate: 75-90% depending on bone quality and technique
- Patient Satisfaction: 65-75% satisfied or very satisfied
Failed Revision (Persistent Pseudarthrosis):
- Recurrent rod fracture in 15-20%
- Chronic pain requiring ongoing management
- Potential need for re-revision
- Lower patient satisfaction (less than 40%)
Predictors of Success
Positive Predictors:
- Solid fusion achieved (most important)
- Correction of sagittal imbalance (SVA less than 50mm)
- Adequate rod augmentation (larger diameter, dual rods)
- Excellent bone quality or treated osteoporosis
- Non-smoker or successful cessation
Negative Predictors:
- Multiple prior revisions (greater than 2)
- Uncorrected positive sagittal balance
- Active infection
- Continued smoking
- Severe osteoporosis (T-score less than -3.0)
- Medical comorbidities (diabetes, obesity, renal failure)
Long-Term Considerations
5-Year Outcomes:
- Fusion rate: 85-95% if first revision, 70-80% if multiple revisions
- Adjacent segment disease: 15-25% (similar to primary fusion)
- Need for further revision: 10-20%
- Return to work: 50-60% in working-age patients
10-Year Outcomes:
- Hardware longevity: 80-90% without further issues if fusion solid
- Adjacent segment degeneration: cumulative 30-40%
- Patient satisfaction maintained: 60-70%
REVISIONREVISION Success Factors
| R | Rod upgrade Larger diameter (6.0mm+), dual rods |
| E | Extend fixation Proximal and distal |
| V | Vitamin D And bone health optimized |
| I | Iliac screws For sacropelvic fixation |
| S | Stop smoking Absolute requirement |
| I | Infection Ruled out and treated |
| O | Osteobiologics Autograft + BMP |
| N | No sagittal imbalance SVA less than 50mm |
| R | Rod upgrade Larger diameter (6.0mm+), dual rods | I | Iliac screws For sacropelvic fixation | O | Osteobiologics Autograft + BMP |
| E | Extend fixation Proximal and distal | S | Stop smoking Absolute requirement | N | No sagittal imbalance SVA less than 50mm |
| V | Vitamin D And bone health optimized | I | Infection Ruled out and treated |
Hook:Address all eight factors systematically during preoperative planning
Prevention Strategies
Preoperative Optimization
Bone Health:
- Screen all patients with DEXA scan if age greater than 50 or risk factors
- Vitamin D supplementation (target greater than 30 ng/mL)
- Calcium 1200-1500mg daily
- Osteoporosis treatment: bisphosphonates or teriparatide
- Consider preoperative teriparatide for 3 months (off-label but evidence-based)
Medical Optimization:
- Smoking cessation minimum 6 weeks (ideally 3 months)
- Glycemic control (HbA1c less than 7.0%)
- Nutritional assessment (albumin greater than 3.5 g/dL)
- Weight optimization (BMI less than 35 if elective)
Intraoperative Strategies
Construct Design:
- Use larger diameter rods (6.35mm for long constructs)
- Dual rods reduce stress and provide redundancy
- Adequate cross-linking (every 3-4 levels)
- Avoid offset connectors when possible
- Minimize rod contouring (use pre-contoured rods)
Fixation Optimization:
- Bicortical screw purchase in osteoporotic bone
- Cement augmentation in severe osteoporosis (T-score less than -3.0)
- Iliac screws for lumbosacral constructs greater than 3 levels
- S2-alar-iliac screws as alternative to traditional iliac fixation
Biological Enhancement:
- Generous autograft from iliac crest or local bone
- BMP-2 for high-risk patients (off-label, 1.5mg/mL)
- Allograft for structural support
- Thorough decortication of fusion bed
Postoperative Strategies
Activity Modification:
- TLSO bracing for 12 weeks in high-risk patients
- Avoid BLT (bending, lifting, twisting) for 3 months
- Gradual return to activities over 6 months
- Permanent restrictions for heavy labor
Surveillance:
- Serial radiographs to detect early pseudarthrosis
- CT at 12 months to confirm fusion
- Early intervention if concerning findings
Medical Management:
- Continue osteoporosis treatment for minimum 2 years
- Permanent smoking cessation
- Weight management
- Optimize chronic conditions (diabetes, nutrition)
PREVENTPREVENT Rod Fracture Strategy
| P | Plan construct With adequate rod size (6.0mm minimum) |
| R | Redundancy With dual rods in high-risk cases |
| E | Enhance biology Autograft, BMP, osteoporosis treatment |
| V | Verify Sagittal balance correction (SVA less than 50mm) |
| E | Extend To ilium for lumbosacral constructs |
| N | No smoking Strict cessation |
| T | Treat Osteoporosis preoperatively |
| P | Plan construct With adequate rod size (6.0mm minimum) | V | Verify Sagittal balance correction (SVA less than 50mm) | T | Treat Osteoporosis preoperatively |
| R | Redundancy With dual rods in high-risk cases | E | Extend To ilium for lumbosacral constructs | ||
| E | Enhance biology Autograft, BMP, osteoporosis treatment | N | No smoking Strict cessation |
Hook:Prevention is best treatment - proactive risk mitigation for any long construct
Controversies & Areas of Uncertainty
Note
Examiners reward candidates who can hold nuance. Rod fracture prevention is not a solved problem, and several "obvious" interventions have softer evidence than commonly assumed.
- Does adding rods always help? Accessory rods across an osteotomy reduce fracture and pseudarthrosis (Buell 2018, Lee 2021). However, a multicentre European cohort found multiple-rod constructs around the PSO did not reduce mechanical complications versus 2-rod constructs, though they improved quality of life and coronal alignment (Bourghli 2021). Rod number is not a substitute for biology and alignment.
- Cobalt-chrome versus titanium. Pooled data favour cobalt-chrome for lower rod fracture and better kyphosis restoration, but at the price of higher proximal junctional kyphosis (Shega 2020). Material choice trades one failure mode for another.
- Can alignment scores predict failure? The GAP score did not reliably predict mechanical complications on external validation in complex deformity (Kwan 2021). Alignment proportion matters but does not capture bone quality, material, or construct redundancy.
- Observation versus revision for an "incidental" rod fracture. A genuinely asymptomatic fracture with CT-confirmed solid fusion can be observed, but distinguishing solid fusion from early pseudarthrosis is imperfect even with metal-artifact-reduction CT, so surveillance must be active.
- Anabolic agents (teriparatide/abaloparatide) and BMP. Biologically attractive for high-risk hosts, but high-quality randomised evidence specifically for rod-fracture endpoints is limited; use is extrapolated from fusion and bone-density data and remains off-label in many jurisdictions.
Evidence Base
- Overall rod fracture rate 26% after deformity correction for lumbar degenerative kyphosis
- Pedicle subtraction osteotomy (PSO) drove fracture (42%) versus LLIF with posterior column osteotomy (7%)
- Titanium rods fractured in 49% vs 18% for cobalt-chrome; accessory rod technique fractured in only 6% vs 32% for 2-rod constructs
- Greater preoperative PI-LL mismatch was the crucial independent risk factor
- Rod fracture at the extended-PSO site occurred in 18.2% and pseudarthrosis in 14.5%
- Accessory supplemental rods across the osteotomy significantly reduced rod fracture or pseudarthrosis (multivariable OR 0.062, p=0.013)
- Interbody cage at the osteotomy improved focal lordosis without changing fracture rate
- Multiple-rod constructs across the PSO did NOT lower rod fracture or pseudarthrosis versus 2-rod constructs (p=0.95)
- Multiple-rod groups showed better coronal alignment and health-related quality of life (SRS-22, SF-36, ODI)
- Tempers the assumption that simply adding rods guarantees mechanical durability
- Distal junctional failure occurred in 40.2%, with rod fracture the most common sign (20.0%); mean time to failure 32.4 months
- PSO (OR 27.3), postoperative SVA, and degree of lumbar lordosis correction were independent risk factors on multivariable analysis
- External validation of the Global Alignment and Proportion (GAP) score in complex deformity (76% had three-column osteotomy)
- A higher GAP score was NOT associated with mechanical complications including rod fracture (AUC 0.60) in this cohort
- More disproportioned alignment was associated with worse ODI/SRS-22/SF-36 outcomes
- Incidence of rod fracture was significantly higher with titanium than cobalt-chrome rods (p=0.0001)
- Cobalt-chrome better restored thoracic kyphosis (p=0.009) but was associated with more proximal junctional kyphosis (p=0.0009)
- No difference in correction rate, lumbar lordosis, fatigue life, or bending stiffness on pooled analysis
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Recurrent Pain After Long Fusion
"A 62-year-old woman presents 18 months after T10-pelvis fusion for adult degenerative scoliosis. She reports excellent pain relief for the first 12 months, but now has severe lower back pain (VAS 8/10) worse with activity. She denies radicular symptoms or neurological changes. Standing radiographs show bilateral rod fractures at L4-L5 level with loss of lumbar lordosis."
Early Rod Fracture Decision-Making
"A 58-year-old man undergoes L2-S1 PSF for degenerative scoliosis with stenosis. At his 3-month follow-up, he reports mild improvement in leg pain but persistent back pain (VAS 6/10). Radiographs show a unilateral rod fracture at L5-S1 on the right side. CT demonstrates less than 25% bridging bone at L5-S1 and normal appearance at other levels. He is an active smoker."
Incidental Rod Fracture in an Asymptomatic Patient
"A 70-year-old man is seen at routine 2-year follow-up after a T10-pelvis fusion with an L3 pedicle subtraction osteotomy for fixed sagittal imbalance. He is delighted with his outcome, walks 5 km daily, and has no back pain. Routine standing radiographs incidentally show a unilateral rod fracture just below the osteotomy. He asks whether he needs another operation."
Exam Day Cheat Sheet
MCQ Practice Points
Clinical Pearl
Q: What are the common causes of spinal rod fractures?
A: Patient factors: Pseudarthrosis/nonunion (the dominant association - without solid fusion the rod bears load and fatigues), positive sagittal imbalance (increased stress on rods), long fusions, osteoporosis, obesity, smoking. Surgical factors: Rod undersizing, inadequate rod contouring, stress risers (notching during contouring), short fusion segments, failure to extend fusion to sacrum/pelvis in long constructs. Mechanical factors: Fatigue failure from cyclic loading before solid fusion; single rod constructs higher risk than dual rods. Most failures occur at lumbosacral junction or at the apex of corrected deformity.
Clinical Pearl
Q: What is the relationship between pseudarthrosis and rod fracture?
A: Pseudarthrosis precedes rod fracture in most cases - without solid fusion, rods bear all load, leading to fatigue failure. Sequence: Nonunion develops (inadequate bone healing), rods subjected to cyclic loading without load-sharing, metal fatigue develops at stress concentration points, eventual fracture. Clinical presentation: Progressive pain, loss of correction, palpable hardware prominence. Radiographic signs: Lucency around screws, loss of lordosis/correction, visible rod discontinuity. Treatment: Address pseudarthrosis with revision fusion, bone grafting, and new instrumentation.
Clinical Pearl
Q: What factors help prevent rod fracture in spinal deformity surgery?
A: Surgical technique: Use dual rods (load sharing), proper rod contouring (avoid notching), adequate rod diameter for patient size, avoid sharp bends (stress risers), ensure solid fixation at both ends of construct. Fusion optimization: Adequate decortication, appropriate bone graft (autograft, BMP), optimize fusion environment (no smoking, proper nutrition). Construct design: Extend to appropriate endpoints, consider interbody support (ALIF, TLIF, XLIF) for anterior column load sharing, address sagittal balance. Rod material: Cobalt-chrome has higher fatigue resistance than titanium but less MRI compatible.
Clinical Pearl
Q: How should symptomatic rod fractures be managed?
A: Workup: Full-length standing radiographs, CT for pseudarthrosis assessment, consider bone scan or SPECT-CT if uncertain. Treatment: Almost always requires revision surgery - rod fracture indicates failed fusion. Surgical strategy: 1) Remove broken rods; 2) Explore fusion mass, identify nonunion; 3) Decorticate and bone graft nonunion sites; 4) Consider interbody fusion for anterior support; 5) New instrumentation with attention to rod size and contour; 6) Consider extending fusion if short segment. Address sagittal balance - persistent malalignment leads to recurrent failure.
Clinical Pearl
Q: What is the role of different rod materials in preventing rod fracture?
A: Titanium alloys: More flexible (lower modulus), better bone-implant interface, MRI compatible, but lower fatigue strength - higher fracture risk in long constructs. Cobalt-chrome (CoCr): Higher modulus (stiffer), superior fatigue resistance - preferred for long constructs, deformity surgery; less MRI compatible. Stainless steel: Rarely used now; intermediate properties. Practical application: Use CoCr for adult deformity, long fusions, high-stress reconstructions; titanium acceptable for shorter fusions. Larger diameter rods (5.5-6.0mm) have greater fatigue resistance than smaller rods. Dual rod constructs distribute load.
Guidelines, Registries & Global Practice
Global Epidemiology
- Rod fracture is a mechanical complication of instrumented fusion worldwide, not a single-population phenomenon; reported rates cluster between roughly 2% (short fusions) and over 25% (long deformity constructs with three-column osteotomy)
- The pedicle subtraction osteotomy site is consistently the dominant location across North American, European, and Asian series
- Time to failure typically spans 1-3 years (mean to distal junctional failure ~32 months)
- Aging populations are increasing the volume of long-construct deformity surgery, so absolute numbers of rod fractures are rising even where rates are stable
Side-by-Side Guidance and Consensus
| Body / Source | Position relevant to rod fracture |
|---|---|
| AO Spine / Scoliosis Research Society | Emphasise restoring proportional sagittal alignment (PI-LL match) and protecting three-column osteotomies with supplemental rods to reduce mechanical failure |
| NICE / BOA (UK) | Optimise modifiable risk before elective fusion: smoking cessation, bone health, glycaemic control; treat symptomatic non-union with revision |
| AAOS / North American practice | Cobalt-chrome favoured for long high-stress constructs; routine sacropelvic (iliac / S2-alar-iliac) fixation for lumbosacral deformity |
| International Spine Study Group / European Spine Study Group | Multicentre data underpin alignment-based prediction (e.g. GAP score) while cautioning that no single score fully predicts mechanical failure |
There is broad agreement that rod fracture is best prevented by simultaneously addressing biology (fusion, bone quality) and biomechanics (alignment, rod material, supplemental fixation) rather than by any single intervention.
Registry and Implant Surveillance
- National implant registries and device regulators (e.g. medical-device vigilance schemes in the EU, UK, US, Australia) conduct post-market surveillance; clusters of rod failure are reportable as adverse events
- Registry signals have reinforced material choice (cobalt-chrome lower fracture rate) and construct-design trends (supplemental rods across osteotomies)
High- versus Limited-Resource Practice Variation
- Well-resourced settings: routine standing full-length imaging, metal-artifact-reduction CT for fusion assessment, intraoperative navigation/neuromonitoring, cobalt-chrome and multi-rod constructs, and pharmacological bone-health optimisation (bisphosphonates, denosumab, anabolic agents)
- Limited-resource settings: rod material and supplemental implants may be constrained by cost and availability; emphasis shifts to meticulous alignment correction, generous autograft, rigorous smoking cessation, and clinical/plain-radiograph surveillance where CT access is limited
- Universal, low-cost levers applicable everywhere: smoking cessation, nutrition and vitamin D optimisation, achieving solid fusion, and correcting sagittal balance
Management Algorithm
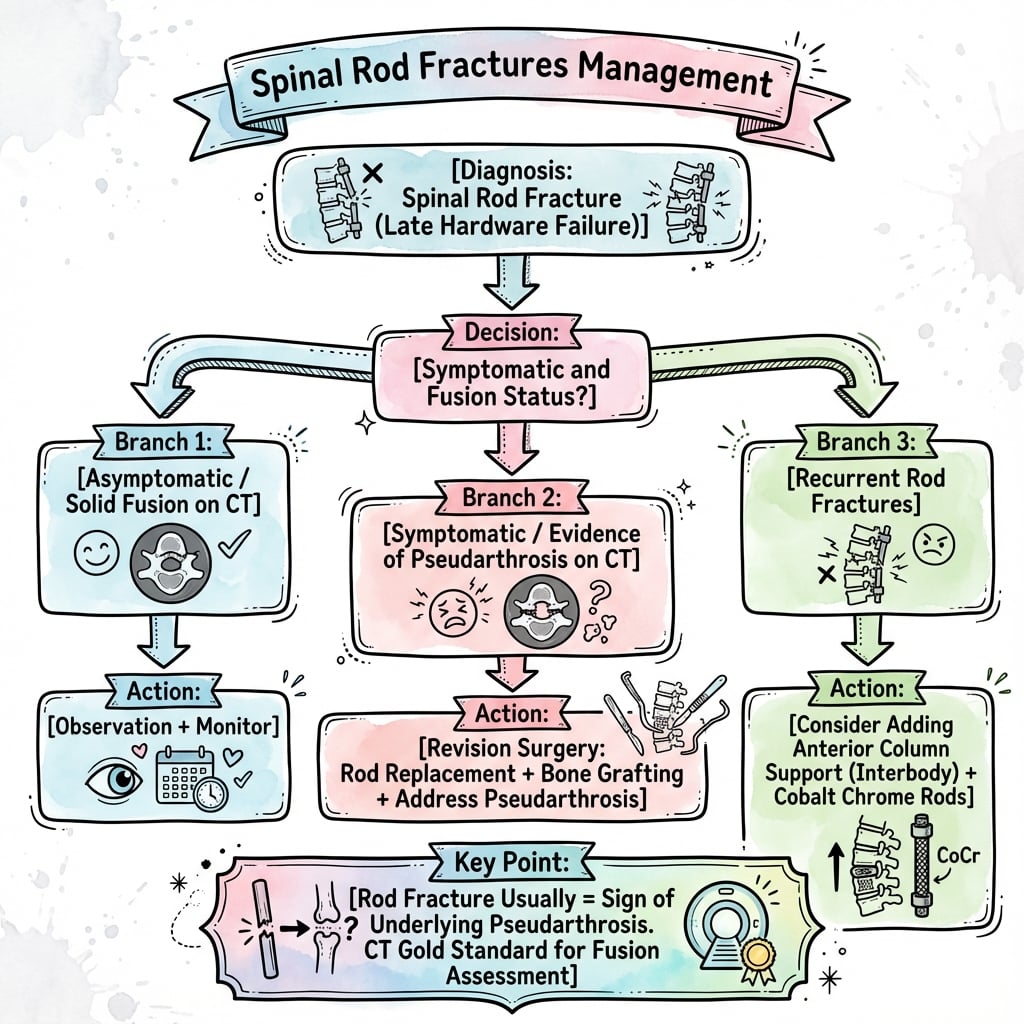
Clinical summary
Rod Fracture Essentials
- •Rod fracture = biomechanical failure indicating construct overload
- •Most common cause is pseudarthrosis (rod bears 100% load without biological support)
- •Typically presents as recurrent pain after pain-free interval
- •Diagnosis confirmed with standing radiographs; CT scan assesses fusion status
- •Management depends on fusion status: solid fusion may observe if asymptomatic, pseudarthrosis requires revision
Classification Quick Reference
- •Type I (isolated fracture, solid fusion) - observe if asymptomatic
- •Type II (fracture with pseudarthrosis) - revision mandatory
- •Type III (fracture with deformity progression) - urgent revision with realignment
- •Type IV (fracture with neurological compromise) - emergent revision with decompression
- •Location matters: proximal junction (extend cranially), mid-construct (connector issue), distal junction (add iliac screws)
Risk Factors - FRACTURE Mnemonic
- •F - Fusion length greater than 5 levels
- •R - Rod diameter reduced (5.5mm)
- •A - Alignment not corrected (positive SVA)
- •C - Connectors offset
- •T - Titanium in long construct
- •U - Under-fixed sacrum
- •R - Revision surgery
- •E - Elderly with osteoporosis
- •Three or more factors = very high risk requiring preventive strategies
Revision Principles - REVISION Mnemonic
- •R - Rod upgrade (6.0mm or 6.35mm, dual rods)
- •E - Extend fixation proximally and distally
- •V - Vitamin D optimized (greater than 30 ng/mL)
- •I - Iliac screws for sacropelvic constructs
- •S - Stop smoking (absolute)
- •I - Infection ruled out
- •O - Osteobiologics (autograft + BMP)
- •N - No sagittal imbalance (SVA less than 50mm)
- •Address all eight factors for success
Investigation Protocol
- •Standing full-spine radiographs (assess global alignment, identify fracture location, measure SVA and coronal balance)
- •CT with metal artifact reduction (gold standard for fusion assessment - less than 50% bridging = pseudarthrosis)
- •Labs: CRP/ESR (infection screening), vitamin D, calcium, bone health markers
- •MRI if infection suspected or new radiculopathy
- •SPECT-CT for equivocal fusion assessment
Surgical Strategy by Type
- •Type I: Focal revision, exchange rod, upgrade size, retain screws if well-fixed
- •Type II: Comprehensive revision, decorticate pseudarthrosis, autograft + BMP, extend fixation 1 level each direction, larger rods
- •Type III: Full revision with osteotomy if needed, dual rods, satellite rods, maximum biological augmentation
- •Type IV: Urgent decompression, stabilization, robust fixation
- •All types: address root cause (fusion, alignment, biomechanics)
Construct Enhancement Options
- •Rod diameter: upgrade 5.5mm to 6.0mm minimum, 6.35mm for long constructs
- •Dual/accessory rods: unload primary rods and add redundancy (most protective across osteotomy sites)
- •Cross-links: every 3-4 levels, side-to-side preferred
- •Iliac screws: mandatory for lumbosacral constructs greater than 3 levels
- •Four-rod technique: dual rods to S1, dual rods to ilium (maximum rigidity)
- •Material: cobalt-chrome for high stress (better fatigue resistance than titanium)
Complications and Rates
- •Recurrent rod fracture: 5-15% (persistent pseudarthrosis main cause)
- •Infection: 3-8% (higher in revision than primary)
- •PJK: 20-40% (overcorrection, UIV at inflection point)
- •Neurological injury: 1-3% (epidural scarring, deformity correction)
- •Medical complications: 10-20% (age, comorbidities, long OR time)
- •Prevention: preop optimization, meticulous technique, neuromonitoring
Expected Outcomes
- •Successful revision (fusion achieved): 70-80% pain relief, 75-90% fusion rate, 65-75% patient satisfaction
- •Failed revision: 15-20% recurrent fracture, chronic pain, need for re-revision
- •Positive predictors: solid fusion, SVA less than 50mm, dual rods, non-smoker, good bone quality
- •Negative predictors: multiple prior revisions, smoking, uncorrected imbalance, osteoporosis, infection
Examiner Expectations
- •Demonstrate systematic approach: diagnosis with appropriate imaging, differentiate from pseudarthrosis (often coexist), identify root cause
- •Comprehensive revision plan addressing biomechanics AND biology
- •Discuss biomechanical principles (stress concentration, fatigue failure, load-sharing)
- •Quote evidence (PSO is the highest-risk site; cobalt-chrome fractures less than titanium; accessory rods across an osteotomy reduce failure)
- •Emphasize prevention strategies
- •Show judgment in observation versus revision decisions