Extensor Hood Disruption | MCP Instability | Radial vs Ulnar Subluxation
Rayan-Murray Classification (1994)
Critical Must-Knows
- Sagittal bands stabilize EDC at MCP level - rupture causes subluxation into intermetacarpal valley
- Long finger most commonly affected (Rayan-Murray series: long greater than small greater than index greater than ring)
- Ulnar EDC subluxation is most common, and it is the RADIAL sagittal band that fails (Young & Rayan biomechanics)
- Rayan Type I-II often respond to extension splinting alone for 4-6 weeks
- Chronic cases (greater than 6 weeks) usually require surgical reconstruction
Clinical Pearls
- "Painful snapping at MCP with active extension = sagittal band injury until proven otherwise
- "Elson test positive (weak MCP extension) with normal PIP/DIP extension = differentiate from central slip
- "Surgical repair within 3 weeks has better outcomes than delayed reconstruction
- "Juncturae tendinum can mask single finger EDC injury - examine each finger independently
Critical Sagittal Band Exam Points
Anatomy and Pathomechanics
Sagittal bands are transverse fibers originating from volar plate that wrap around EDC to stabilize it dorsally over MCP. Rupture allows EDC to subluxate into intermetacarpal valley (usually ulnarly). Loss of MCP extension power.
Clinical Diagnosis
Classic triad: Pain over MCP with active extension, palpable/visible tendon subluxation (snap), weak active MCP extension. EDC tendon displaces ulnarly with MCP flexion and snaps back with extension.
Surgical Repair
Direct repair best for acute injuries (within 3 weeks). Techniques: Direct suture, juncturae transfer, free tendon graft. Goal: Restore EDC centralization and MCP extension strength.
Rehabilitation
Early diagnosis critical - Type I-II often heal with 4-6 weeks extension splinting. Chronic injuries (greater than 6 weeks) develop scarring and require reconstruction with worse outcomes.
Quick Decision Guide
| Rayan Type | Clinical Features | Primary Treatment | Key Pearl |
|---|---|---|---|
| Type I (Partial) | Pain, NO subluxation, maintains extension | Splint MCP extension 4-6 weeks | Conservative treatment successful in 80% |
| Type II (Complete, reducible) | Subluxation with flexion, reduces with extension | Splint vs early surgery if active | Surgery preferred for athletes, manual laborers |
| Type III (Irreducible) | Tendon locked in intermetacarpal valley | Surgical reduction and repair | Cannot extend MCP actively |
STEELSagittal Band Anatomy (Extensor Hood Components)
| S | Sagittal bands Transverse fibers from volar plate to EDC |
| T | Triangular ligament Connects lateral bands distally |
| E | EDC tendon Central slip and terminal extension |
| E | Extensor hood Covers dorsum of MCP joint |
| L | Lateral bands Intrinsic contributions (lumbricals, interossei) |
| S | Sagittal bands Transverse fibers from volar plate to EDC | E | Extensor hood Covers dorsum of MCP joint |
| T | Triangular ligament Connects lateral bands distally | L | Lateral bands Intrinsic contributions (lumbricals, interossei) |
| E | EDC tendon Central slip and terminal extension |
Hook:STEEL represents the strength of the extensor hood - Sagittal bands are the foundation that keep the mechanism centralized!
SNAPClinical Examination Findings
| S | Subluxation visible EDC displaces ulnarly with MCP flexion |
| N | No PIP/DIP deficit Distinguishes from central slip injury |
| A | Active extension weak Cannot fully extend MCP against resistance |
| P | Painful popping Snapping sensation with active extension |
| S | Subluxation visible EDC displaces ulnarly with MCP flexion | A | Active extension weak Cannot fully extend MCP against resistance |
| N | No PIP/DIP deficit Distinguishes from central slip injury | P | Painful popping Snapping sensation with active extension |
Hook:SNAP - you can feel and hear the tendon SNAP as it subluxates and reduces!
CRAFTSurgical Repair Options
| C | Centralize EDC Goal of all repair techniques |
| R | Repair directly Primary suture if tissue quality good |
| A | Augment with juncturae Transfer adjacent juncturae to reinforce |
| F | Free tendon graft Reconstruct sagittal band if tissue poor |
| T | Tension appropriate Not too tight (MCP stiffness) or loose (re-subluxation) |
| C | Centralize EDC Goal of all repair techniques | F | Free tendon graft Reconstruct sagittal band if tissue poor |
| R | Repair directly Primary suture if tissue quality good | T | Tension appropriate Not too tight (MCP stiffness) or loose (re-subluxation) |
| A | Augment with juncturae Transfer adjacent juncturae to reinforce |
Hook:CRAFT represents the surgical skill needed - multiple techniques available, goal is to CRAFT a stable centralized extensor mechanism!
Overview and Epidemiology
Sagittal band injuries are an uncommon but functionally significant hand injury that disrupts the balance of the extensor mechanism at the MCP joint. The long finger (third ray) is the most commonly affected digit, attributed to its greater excursion and central position; biomechanically, instability after sagittal band division is most pronounced in the long finger and least in the small finger.
Why Sagittal Bands Matter
Sagittal bands act as the dorsal stabilizers of the extensor tendon at the MCP joint, preventing subluxation into the intermetacarpal valleys during finger flexion and extension. Without intact sagittal bands, the mechanical advantage of the extensor digitorum communis is lost, resulting in weak MCP extension despite intact tendon continuity.
Demographics
- Age: Typically young to middle-aged active adults (athletic and occupational injuries)
- Mechanism: Forced MCP flexion/extension or direct blow (punching = boxer knuckle), laceration, or spontaneous attenuation in rheumatoid arthritis
- Digit frequency (Rayan-Murray series): long, then small, then index, then ring
- Note: "Long finger" and "middle finger" are the same digit (the third ray) - it is the single most commonly injured
Clinical Impact
- Function: Weak grasp and release due to loss of effective MCP extension
- Pain: Painful snapping with gripping and active extension
- Population: Boxers, martial artists and manual workers over-represented (forced-flexion mechanism)
- Prognosis driver: Time to treatment - non-operative success is best when started within 3 weeks of injury
Anatomy and Pathomechanics
Extensor Hood Complexity at MCP Joint
The sagittal band is NOT a simple ligament but rather a complex confluence of transverse fibers from the volar plate, longitudinal fibers from the interosseous fascia, and contributions from the juncturae tendinum. This creates a dynamic stabilization system that centralizes the EDC during the full arc of MCP motion.
Sagittal Band Anatomy
Structure
Origin: Volar plate of MCP joint, interosseous fascia
Course: Wrap around radial and ulnar sides of EDC tendon
Insertion: Merge with extensor hood dorsally, anchoring EDC to metacarpal
Clinical correlate: Disruption of the RADIAL band produces ulnar tendon instability; proximal radial fibers are the critical restraint (Young & Rayan)
Function
Stabilization: Prevent EDC subluxation into intermetacarpal valley
Force transmission: Transfer intrinsic muscle forces to extensor mechanism
MCP extension: Act as direct MCP extensors (independent of EDC)
Dynamic centering: Maintain EDC position through full ROM
Biomechanics of Subluxation
| Phase of Motion | Normal Mechanism | After RADIAL Band Rupture (common) | After ULNAR Band Rupture (rare) |
|---|---|---|---|
| MCP extension (rest) | EDC centralized dorsally | EDC tends to displace ULNARLY | EDC tends to displace radially (minimal in cadaver models) |
| MCP flexion (gripping) | EDC maintained dorsal by sagittal bands | EDC subluxates ULNARLY into the intermetacarpal valley (typical pattern) | EDC subluxates radially over the metacarpal head (uncommon) |
| Active extension | Smooth EDC excursion, strong extension | Painful snap as tendon reduces from the ulnar valley, weak extension | Painful snap as tendon reduces radially |
Why Ulnar Subluxation Predominates
Ulnar EDC subluxation is the most common pattern. The counter-intuitive key point (Young & Rayan, cadaveric biomechanics): it is disruption of the RADIAL sagittal band that allows the tendon to slip ulnarly. Dividing the ulnar band alone produced NO instability, whereas partial proximal radial-band division caused subluxation and complete radial division caused dislocation. Contributing factors include the natural ulnar resting drift of the EDC and ulnarly directed forces during pinch/grip.
Relationship to Other Structures
The sagittal band is intimately related to the juncturae tendinum (interconnections between adjacent EDC tendons). Juncturae can partially compensate for sagittal band disruption in some cases, explaining why index and small fingers (with strongest juncturae) are less commonly symptomatic.
Classification Systems
Rayan Classification of Sagittal Band Injuries
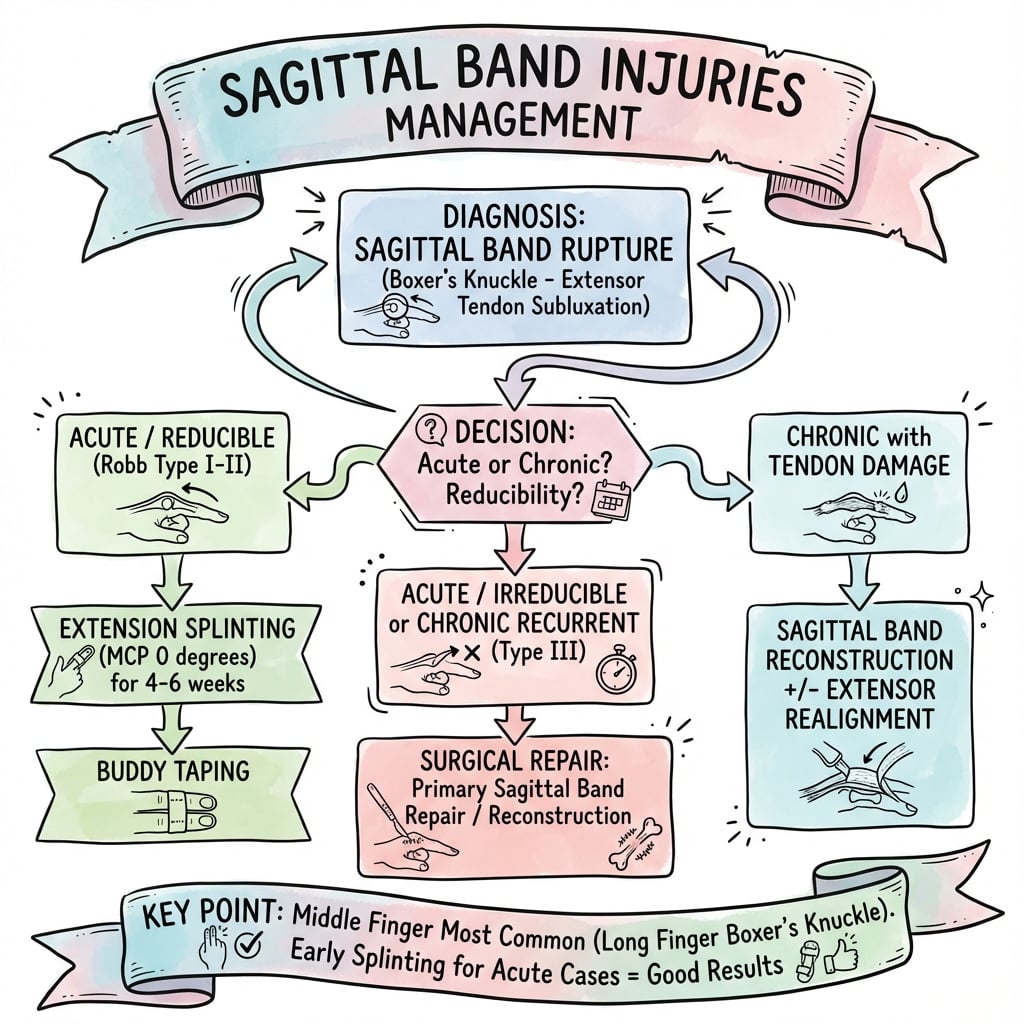
The Rayan classification (most widely used) is based on severity and reducibility of EDC subluxation. This guides treatment decisions.
| Type | Pathology | Clinical Findings | Treatment | Prognosis |
|---|---|---|---|---|
| Type I | Partial tear or attenuated sagittal band | Pain, mild swelling, NO visible subluxation, active extension maintained | Splint MCP extension 4-6 weeks, NSAIDS | 85-90% excellent outcomes |
| Type II | Complete tear, tendon subluxates but reducible | Visible/palpable subluxation with MCP flexion, painful snap with extension, weak active extension | Splinting vs surgery (consider surgery for athletes, manual workers) | 80% good with splinting, 90% with surgery |
| Type III | Complete tear with frank tendon dislocation into the intermetacarpal valley | Tendon displaced, weak or absent active MCP extension, painful snap | Acute closed: trial relative-motion splint (can succeed). Irreducible/chronic/lacerated: surgical reduction and repair | Good with early treatment; worse if chronic (greater than 6 weeks) |
Type II vs Type III Distinction
The key distinction is reducibility. Type II subluxates with MCP flexion but reduces with extension (dynamic instability). Type III is locked in subluxated position (static deformity). Type III CANNOT achieve active MCP extension and requires surgery.
Clinical Assessment
History
- Mechanism: Forced MCP flexion (punching, ball sports), direct trauma, spontaneous (RA)
- Symptoms: Painful snapping at MCP, weakness extending finger, swelling over MCP
- Timing: Acute (days), subacute (weeks), chronic (months)
- Hand dominance: Affects treatment urgency
- Occupation: Manual labor vs desk work
- Red flags: Rheumatoid arthritis (pathologic rupture), multiple finger involvement
Examination
- Look: Swelling over MCP, finger posture at rest
- Feel: Tenderness over radial or ulnar sagittal band, palpable snap with motion
- Move: Active MCP extension (weak), observe for tendon subluxation, check PIP/DIP extension (normal)
- Special tests: Dynamic subluxation test, resisted MCP extension
- Neurovascular: Intact (not a feature of isolated sagittal band injury)
Special Tests
Clinical Examination Maneuvers
Technique: Ask patient to make a fist (flex all MCPs), then actively extend fingers.
Positive test: Visible or palpable EDC tendon subluxation (usually ulnarly) with MCP flexion, followed by painful snap as tendon reduces with active extension.
Observer: Place finger over dorsal MCP to feel tendon displacement.
Interpretation: Confirms sagittal band disruption allowing dynamic instability.
Technique: Stabilize proximal phalanx in slight flexion, ask patient to extend MCP against examiner resistance.
Positive test: Weak extension with pain at MCP (compares to normal adjacent fingers).
Note: PIP and DIP extension should be NORMAL (rules out central slip injury).
Interpretation: Loss of mechanical advantage due to EDC eccentric position.
Standard Elson: Flex PIP over table edge, ask patient to extend PIP against resistance.
In sagittal band injury: PIP extends normally (central slip intact), but MCP extension weak.
Contrast: Central slip injury shows weak PIP extension with rigid DIP extension.
Interpretation: Helps differentiate MCP-level pathology from PIP-level central slip rupture.
Differential Diagnosis
Key differentials to exclude:
- Central slip rupture (Zone III): Weak PIP extension, positive Elson test, risk of boutonniere
- EDC laceration (Zone V): Complete loss of MCP extension, visible wound
- MCP joint arthritis: Stiffness, limited ROM, radiographic changes
- Extensor tendon rupture in RA: Multiple fingers, systemic disease, atraumatic
Distinguishing feature: Sagittal band injury has DYNAMIC subluxation with painful snap, normal PIP/DIP extension, and weak but present MCP extension.
Differential Diagnosis Comparison
Differentiating Sagittal Band Injury from Mimics
| Condition | Level / Site | Active Extension Pattern | Key Discriminator | Confirmatory Test |
|---|---|---|---|---|
| Sagittal band injury | MCP joint (extensor hood) | Weak but present MCP extension; normal PIP/DIP | Dynamic EDC subluxation with painful snap on clenched fist | Dynamic clenched-fist ultrasound |
| Central slip (Zone III) rupture | PIP joint | Weak PIP extension; MCP normal | Positive Elson test, evolving boutonniere | Elson test; lateral PIP radiograph |
| EDC laceration (Zone V) | Over the metacarpal/MCP | Complete loss of MCP extension | Open wound, no dynamic snap, fixed deficit | Wound exploration |
| Rheumatoid extensor subluxation/rupture | MCP joint, often multiple digits | Progressive loss of MCP extension | Atraumatic, multi-digit, synovitis, ulnar drift | Tenodesis test, inflammatory markers, US |
| MCP locking / osteoarthritis or loose body | MCP joint | Mechanical block, not weakness | Catching/locking without tendon snap | Radiographs |
Investigations
Imaging Protocol
Views: PA, lateral, oblique of affected digit
Purpose: Exclude bony pathology, assess MCP joint
Findings: Usually NORMAL (soft tissue injury), may show MCP joint space narrowing if chronic arthritis
Stress views: Dynamic lateral with active MCP flexion may show tendon subluxation (rarely needed)
Advantages: Dynamic real-time assessment of EDC subluxation, assess sagittal band integrity
Technique: Dorsal longitudinal view over MCP, ask patient to flex/extend MCP, observe EDC movement
Positive findings: EDC displacement into intermetacarpal valley with MCP flexion, discontinuity of sagittal band fibers
Availability: Operator-dependent, not widely used but increasing
Indications: Chronic cases, atypical presentation, pre-operative planning
Findings: Disruption of sagittal band fibers, fluid in MCP joint, EDC tendon position
Utility: Can assess tissue quality for surgical planning (acute vs chronic scarring)
Cost: Expensive, rarely necessary if clinical diagnosis clear
Clinical Diagnosis is Key
Sagittal band injuries are clinical diagnoses. Imaging is primarily to exclude other pathology (fracture, arthritis) rather than to confirm sagittal band rupture. The dynamic subluxation test is more sensitive and specific than any imaging modality.
Management Algorithm
Conservative Treatment Indications
Ideal Candidates
- Rayan Type I: Partial tear, no subluxation
- Rayan Type II: Reducible subluxation, low-demand patient
- Acute presentation: Within 2-3 weeks of injury
- Patient factors: Non-manual occupation, older age, medical comorbidities
Contraindications
- Rayan Type III: Irreducible subluxation
- Chronic injury: Greater than 6 weeks
- High-demand patients: Athletes, manual laborers who need reliable grip strength
- Failed splinting: Recurrent subluxation after adequate trial
Splinting Protocol
Splint type: Custom thermoplastic dorsal blocking splint OR aluminum foam commercial splint
Position: MCP in FULL extension (0 degrees), PIP and DIP joints free to move
Wear schedule: Continuous 24 hours/day (remove only for hygiene)
Activities: No gripping, lifting, or forceful hand use
Monitoring: Weekly follow-up to assess compliance, skin integrity, adjust splint
Daytime: Remove for light activities if no pain or subluxation
Nighttime: Continue splinting during sleep
Exercises: Gentle active ROM, blocked MCP extension (protect repair)
Avoid: Forceful gripping, weight-bearing on hand
Splint: Discontinue if MCP stable and no pain
Therapy: Progressive grip strengthening with putty, therapy balls
Monitor: Any recurrence of snapping or subluxation
Return to activity: Gradual, based on symptom tolerance
Goal: 80% grip strength, no pain, no subluxation
Work: Return to manual labor if criteria met
Sports: Protective taping for contact sports for additional 4 weeks
Follow-up: If symptoms recur, consider surgical reconstruction
Success Rates for Conservative Treatment
Rayan Type I: 85-90% success with splinting. Rayan Type II: 70-80% success (higher failure in manual laborers and athletes). Rayan Type III: Splinting contraindicated - requires surgery. Overall, early presentation (within 3 weeks) has best non-operative outcomes.
Surgical Technique
Patient Positioning
Setup Checklist
Supine on operating table with hand table.
- Shoulder abducted 80-90 degrees
- Elbow extended on arm board
- Forearm pronated (dorsal hand up)
- Wrist neutral to slight extension
Forearm tourniquet preferred for better visualization.
- Pressure: 200-225 mmHg
- Exsanguination: Elevation 2 minutes OR Esmarch bandage
- Limit: 90 minutes (most cases completed in 30-45 minutes)
- Prep from fingertips to mid-forearm with betadine or chlorhexidine
- Transparent hand drape allows visualization of finger motion intraoperatively
- Expose all digits to assess juncturae and EDC continuity
Consent Points
- Recurrence: 10-15% (higher in chronic cases)
- Stiffness: 10% (especially if immobilized prolonged)
- Infection: 2-5% (low risk)
- MCP joint stiffness: 5-10% if overly tight repair
- Need for revision: 10% (juncturae transfer or reconstruction)
- Incomplete return of strength: 15-20%
Equipment Checklist
- Instruments: Hand surgery set, fine scissors, forceps
- Sutures: 3-0 or 4-0 braided non-absorbable (sagittal band repair), 5-0 nylon (skin)
- Magnification: Loupe 2.5-3.5x (not mandatory but helpful)
- Tendon graft: Palmaris longus harvested if reconstruction needed
- Splint materials: Thermoplastic for postoperative extension splint
Complications
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Recurrent subluxation | 10-15% | Chronic injury, inadequate repair tension, early mobilization, heavy manual labor | Revision repair with juncturae augmentation or tendon graft reconstruction |
| MCP stiffness (extension contracture) | 10% | Over-tight repair, prolonged immobilization greater than 6 weeks | Hand therapy with passive flexion stretching, rarely requires surgical release |
| Loss of MCP flexion | 5-10% | Excessive scar formation, adhesions | Aggressive hand therapy, tenolysis if persistent at 6 months |
| Infection | 2-5% | Open injury, diabetes, immunosuppression | Antibiotics, irrigation and debridement if deep, delayed repair |
| Dorsal sensory nerve injury | 3-5% | Iatrogenic during dissection | Neuroma excision and burial if symptomatic painful neuroma |
| Incomplete return of grip strength | 15-20% | Chronic injury, muscle atrophy, patient factors | Prolonged hand therapy (up to 6 months), accept functional outcome |
Preventing Recurrence
The most common complication is recurrent EDC subluxation (10-15%). Prevention strategies: 1) Adequate tissue tension at repair (EDC centralized with MCP extended), 2) Augmentation with juncturae transfer in subacute/chronic cases, 3) Strict compliance with 4-6 week immobilization, 4) Gradual return to heavy activity over 12 weeks.
Postoperative Care and Rehabilitation
Postoperative Rehabilitation Timeline
Splint: MCP extension splint worn continuously (24/7).
Remove only: For wound care by therapist (suture removal at 10-14 days).
PIP/DIP ROM: Encouraged to prevent stiffness in adjacent joints.
Activity: No gripping, no weight-bearing on hand.
Follow-up: Wound check at 10-14 days, therapy initiation at 2 weeks.
Splint: Remove for supervised therapy sessions only.
Exercises: Gentle active MCP flexion and extension within pain-free range.
Blocked exercises: Isolate MCP ROM (stabilize proximal phalanx).
Splint between exercises: Maintain extension between sessions and at night.
Goal: Achieve 60-70 degrees MCP flexion without pain or subluxation.
Wean splint: Discontinue daytime splinting, continue nighttime.
Exercises: Full active ROM, composite fist, intrinsic stretching.
Light resistance: Putty exercises, soft therapy balls.
Monitor: Any recurrence of snapping or subluxation (if occurs, return to splinting).
Discontinue splint: If full ROM and no subluxation.
Progressive resistance: Grip strengthening with graded resistance.
Work simulation: Activity-specific exercises for return to work.
Goal: 80% grip strength compared to contralateral hand.
Work: Return to manual labor if strength criteria met.
Sports: Gradual return, protective taping for contact sports for additional 4 weeks.
Final outcome: Expect 85-90% of baseline function.
Importance of Compliance
Patient compliance with the 4-6 week immobilization is CRITICAL. Early mobilization (before 4 weeks) significantly increases risk of recurrent subluxation. Therapist-supervised progression ensures safe return to activity without overstressing repair.
Outcomes and Prognosis
| Treatment | Patient Group | Expected Outcomes | Predictors of Poor Outcome |
|---|---|---|---|
| Splinting (Type I-II acute) | Low-demand, office workers | 80-85% good, minimal recurrence | Manual labor, poor compliance, presentation greater than 3 weeks |
| Direct repair (Type II-III acute) | Athletes, manual workers | 90% return to sport/work at pre-injury level | Delayed surgery greater than 6 weeks, inadequate tension at repair |
| Reconstruction (chronic greater than 6 weeks) | All patients | 60-70% good, higher stiffness and recurrence | Greater than 6 months delay, multiple previous failed repairs, rheumatoid arthritis |
Factors Predicting Success
Best outcomes: Acute presentation (within 3 weeks), Rayan Type I-II, surgical repair with adequate tension, patient compliance with immobilization, experienced hand surgeon and therapist. Worst outcomes: Chronic injury (greater than 6 weeks), failed prior repair, rheumatoid arthritis, manual laborer who returns to heavy work too early.
Controversies and Areas of Uncertainty
The evidence base is almost entirely small retrospective series, case reports and cadaveric work - there are no randomised trials. The following genuine areas of debate are high-yield for discussion vivas.
Splinting: rigid vs relative-motion
Traditional teaching used continuous full MCP-extension immobilisation for 4-6 weeks. Catalano's "sagittal band bridge" and subsequent relative-motion (yoke) splints hold the injured MCP in relative hyperextension while permitting early active motion, and even acute Type III injuries have healed this way. The optimal splint design and duration remain unsettled.
Can acute Type III be treated closed?
Classic doctrine made tendon dislocation (Type III) an operative indication. Catalano showed many acute closed Type III injuries succeed with relative-motion splinting if treated early. Whether to operate primarily or trial a splint in an acute Type III is a genuine decision point.
Which reconstruction is best?
Direct repair, junctura-tendinum transfer, distally based EDC tendon flaps and free tendon grafts all have advocates with no comparative data. The anchor point (deep transverse metacarpal ligament vs adjacent volar plate) is debated, with biomechanical modelling suggesting volar-plate anchoring lowers repair tension in flexion.
The radial-vs-ulnar mechanism
Cadaveric work (Young & Rayan) is clear that radial-band disruption drives ulnar instability, yet many texts still teach the inverted explanation (that a "thicker radial band" protects against ulnar slip). Examiners may probe this - quote the biomechanics, not the folklore.
Evidence Base and Key Studies
Classification and Treatment of Closed Sagittal Band Injuries
- Retrospective series of 28 nonrheumatoid patients with sagittal band injuries
- Defined the three clinical types still used today: Type I (no extensor tendon instability), Type II (tendon subluxation), Type III (tendon dislocation)
- Digit frequency in this cohort: long, then small, then index, then ring
- 8 of 9 small-finger injuries involved the RADIAL sagittal band, 4 with small-finger abduction deformity
- Satisfactory results with non-operative (splint) treatment when started within 3 weeks of injury; 10 patients required surgery (extensor centralization or tendon transfer)
The Sagittal Band: Anatomic and Biomechanical Study
- Cadaveric study of 48 digits defining sagittal band anatomy and the mechanism of injury
- Extensor instability after sagittal band division was most common in the long finger and least common in the small finger
- Ulnar extensor instability results from RADIAL sagittal band disruption; serial division of the ulnar band alone produced no instability
- Partial proximal (not distal) radial band division caused subluxation; complete radial division caused dislocation
- Greatest forces on the sagittal band occurred at full MCP extension (and full flexion); wrist flexion worsened instability
Closed Treatment of Nonrheumatoid Extensor Tendon Dislocations (Sagittal Band Bridge Splint)
- Retrospective review of 10 patients (11 digits) with ACUTE complete EDC dislocation (Rayan-Murray Type III)
- Treated with a relative-motion splint holding the injured MCP in 25-35 degrees of hyperextension relative to adjacent MCPs (the sagittal band bridge)
- Immediate active PIP/DIP motion; mean follow-up 14 months
- All patients regained full flexion-extension range; 8 of 10 pain-free; 3 treatment failures (moderate residual subluxation, 1 needed reconstruction)
- Shows that even acute Type III injuries can often be managed non-operatively with relative-motion splinting
MCP Joint Extensor Tendon Subluxation: A Reconstructive Stabilization Technique
- Describes a junctura-tendinum-based reconstruction that lengthens an EDC slip to recreate a sagittal-band sling and centralize the extensor tendon
- Designed to reproduce native anatomy with minimal local soft-tissue disruption
- Aims for a strong repair without the MCP stiffness associated with tighter techniques
- Reported as simple and effective in the illustrated case
Ultrasound Follow-up of Conservatively Treated Sagittal Band (Dorsal Hood) Injuries
- Three cases of partial sagittal band tear (two index, one long finger) diagnosed with dynamic ultrasound
- Dynamic US identified the torn sagittal band and confirmed (sub)luxation of the extensor tendon
- All treated conservatively; pain resolved at 3, 6 and 9 months respectively
- One-year dynamic US confirmed painless full range of motion with no residual subluxation
Boxer Knuckle: Extensor Hood Injury with Tendon Subluxation Diagnosed by Dynamic US
- Dynamic ultrasound of the clenched fist in three subjects with extensor tendon dislocation
- Traumatic cases showed dislocated but grossly intact tendons with surrounding soft-tissue oedema; sagittal band rupture confirmed at surgery
- MRI in one case corroborated the US findings
- Highlights the boxer-knuckle mechanism (forced MCP flexion, e.g. punching) and the diagnostic value of clenched-fist dynamic US
Extensor Tendon Ruptures in Rheumatoid Arthritis
- Review of rheumatoid extensor tendon dysfunction, including sagittal band attenuation and progressive ulnar EDC subluxation
- Best treatment is prevention - medical control and tenosynovectomy before rupture occurs
- Emphasises treating single-finger extension loss before progression to multiple-finger loss
- Once ruptured, tendon transfer or free tendon grafting restores extension; rheumatologist communication is essential
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Sagittal Band Injury (~2-3 min)
"A 35-year-old manual laborer presents 5 days after punching a wall in anger. He has pain over the dorsum of his right long finger MCP joint and complains of a snapping sensation when he makes a fist. On examination, you observe the EDC tendon subluxating ulnarly with MCP flexion and snapping back with extension. He has weak but present active MCP extension. What is your assessment and management?"
Scenario 2: Failed Conservative Management (~3-4 min)
"A 42-year-old female was treated with MCP extension splinting for 6 weeks for a Rayan Type II sagittal band injury of her index finger. She was initially compliant but now, 2 weeks after discontinuing the splint, she has recurrent painful snapping and visible EDC subluxation with gripping. She is frustrated and wants definitive treatment. How would you manage this case?"
Scenario 3: Chronic Sagittal Band Injury (~2-3 min)
"A 55-year-old patient with rheumatoid arthritis presents with progressive ulnar subluxation of the EDC tendons of her long and ring fingers over the past 6 months. She has difficulty extending her MCPs and reports that the tendons slip off the side of the knuckles when she tries to grip. Examination shows fixed ulnar subluxation of EDC with inability to actively extend the MCPs. How would you manage this?"
MCQ Practice Points
Rayan Classification Question
Q: A patient has visible EDC tendon subluxation with MCP flexion that reduces with extension, and weak but present active MCP extension. What is the Rayan classification and recommended treatment? A: Rayan Type II (complete tear with reducible subluxation). Treatment depends on patient factors: splinting for low-demand patients (70-80% success), surgical repair for high-demand patients/athletes/manual laborers (90% success).
Anatomy Question
Q: Why is ulnar subluxation of the EDC more common than radial subluxation in sagittal band injuries? A: The high-yield answer is the cadaveric biomechanics of Young & Rayan: it is the RADIAL sagittal band whose disruption permits the tendon to slide ulnarly. Dividing the ulnar band alone produced no instability; partial proximal radial-band division caused subluxation and complete radial division caused dislocation. The natural ulnar resting drift of the EDC and ulnarly directed grip/pinch forces reinforce this. Hence ulnar subluxation is the typical pattern.
Surgical Timing Question
Q: What is the optimal timing for treatment of sagittal band injuries and why? A: Treatment (operative or non-operative) is best started within 3 weeks of injury, when tissue quality is good and direct repair or splinting is most likely to succeed (Rayan-Murray). Beyond 6 weeks, scarring and attenuation make direct repair difficult, often requiring reconstruction with inferior outcomes.
Guidelines, Registries & Global Practice
Sagittal band injury is a clinical (not registry-tracked) diagnosis, so there is no implant or arthroplasty registry data and no formal Level-1 society guideline. Practice is governed by classic case series and consensus expert opinion, which is broadly consistent worldwide.
Global Epidemiology and Setting
- Distribution: Worldwide; no geographic predilection. Over-represented in combat-sport athletes (boxing, MMA, "boxer knuckle") and manual workers
- Long finger (third ray) is the most frequently injured digit across published series
- Rheumatoid presentation is declining globally as early DMARD/biologic therapy and tenosynovectomy reduce tendon-centred deformity
- Limited-resource settings: Reliance on clinical diagnosis and relative-motion/extension splinting is an advantage - no advanced imaging required
Consensus Across Practice
- Shared principles (AAOS, BSSH/BOA, federation of European hand societies, ASSH teaching): trial of splinting first for closed acute injuries presenting within ~3 weeks; surgery for irreducible, chronic, lacerated, or failed-conservative cases
- Relative-motion (yoke / sagittal band bridge) splinting increasingly favoured over rigid MCP immobilisation, allowing early controlled motion
- Rheumatoid disease: multidisciplinary rheumatology co-management and disease control before elective reconstruction
- Prognosis counselling: acute repair outcomes good; chronic reconstruction and RA cases more guarded
Global Exam Framing
Because there is no registry or graded guideline, examiners (FRCS, FRACS, EBOT, ABOS, DNB/MS) expect you to anchor decisions on the Rayan-Murray classification (1994), the 3-week window for non-operative success, and the biomechanical principle that the radial band fails to allow ulnar subluxation. Relative-motion splinting is the modern, resource-light first-line approach worldwide.
Documentation and Pitfalls (Global)
Key documentation: mechanism (sport/assault/occupational/spontaneous in RA), Rayan-Murray type, reducibility, time since injury, and a clear record of the operative vs non-operative discussion with realistic outcome expectations and consent for recurrence, stiffness and incomplete return of strength.
Common pitfalls:
- Missing the diagnosis as a "simple contusion" so the patient presents late with fixed subluxation
- Failing to differentiate from central slip injury (always check PIP/DIP extension)
- Over-tight repair causing an MCP extension contracture
- Inadequate splint education leading to non-operative failure
SAGITTAL BAND INJURIES
Clinical summary
Key Anatomy
- •Sagittal bands = transverse fibers from volar plate wrapping around EDC to stabilize at MCP level
- •RADIAL band disruption causes ULNAR EDC instability (the common pattern); proximal radial fibers are the key restraint
- •Long finger (third ray) most commonly affected; greatest instability after division (least in small finger)
- •Function: Centralize EDC, prevent subluxation into intermetacarpal valley, transmit intrinsic forces
Rayan Classification
- •Type I = Partial tear, NO subluxation, active extension maintained → Splint 4-6 weeks
- •Type II = Complete tear, REDUCIBLE subluxation → Splint (low-demand) vs Surgery (high-demand)
- •Type III = Complete tear, IRREDUCIBLE subluxation → Surgery required
- •Dynamic subluxation test: EDC displaces ulnarly with MCP flexion, snaps back with extension
Treatment Algorithm
- •Type I: Splint MCP extension 4-6 weeks (85-90% success)
- •Type II: Surgery for athletes/manual workers, splinting for office workers
- •Type III: Surgical reduction and repair (cannot extend MCP actively)
- •Chronic (greater than 6 weeks): Reconstruction with tendon graft (worse outcomes 60-70%)
- •Optimal surgical timing: 1-3 weeks (90% good outcomes)
Surgical Pearls
- •Direct repair: Horizontal mattress sutures with 3-0 non-absorbable, tension with MCP extended
- •Juncturae transfer: Augment weak tissue by transferring adjacent juncturae
- •Tendon graft: Palmaris longus reconstruction for chronic/RA cases
- •Critical: Appropriate tensioning (too loose = re-subluxation, too tight = extension contracture)
- •Test repair: Passive MCP flexion to 90 degrees should not cause subluxation
Rehabilitation
- •Immobilization: MCP extension splint 4-6 weeks CONTINUOUSLY (PIP/DIP free)
- •Early mobilization before 4 weeks increases recurrence risk 20-30%
- •Weeks 4-6: Protected supervised ROM
- •Weeks 6-12: Progressive strengthening
- •Return to manual work: 10-12 weeks
Outcomes and Complications
- •Acute repair: 85-90% good outcomes
- •Chronic reconstruction: 60-70% good outcomes
- •Recurrence: 10-15% (higher in chronic cases, inadequate repair tension)
- •MCP stiffness: 10% (over-tight repair)
- •Predictors of poor outcome: Chronic injury greater than 6 weeks, RA, failed previous repair, manual labor with early return to work