A Posteromedial-Corner Cause of Knee Pain
- SEMIMEMBRANOSUS TENDINOPATHY is an OVERUSE tendinopathy of the DISTAL SEMIMEMBRANOSUS at/near its insertion on the POSTEROMEDIAL TIBIA, and is a recognised - though under-recognised - cause of chronic POSTEROMEDIAL knee pain; the semimembranosus has a complex multi-armed distal insertion that also stabilises the posteromedial corner of the knee.
- It presents with chronic, localised POSTEROMEDIAL knee PAIN and TENDERNESS over the insertion, characteristically worse on RESISTED KNEE FLEXION and with activity, typically in running/cutting or repetitive knee-flexion athletes (an overuse aetiology).
- The DIFFERENTIAL is the posteromedial-corner/medial knee pain group: a POSTERIOR-HORN MEDIAL MENISCUS tear, PES ANSERINE bursitis/tendinopathy (usually more anteromedial), a POPLITEAL (Baker's) CYST, medial collateral/posteromedial-corner pathology, and referred medial-compartment osteoarthritis - localising the tenderness and correlating with imaging separates them.
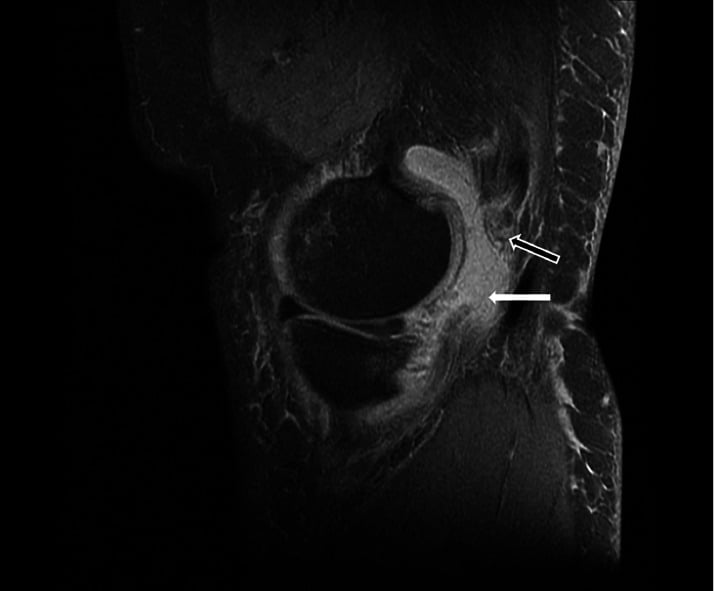
- DIAGNOSIS is clinical (localised posteromedial tenderness over the insertion, pain on resisted flexion) supported by IMAGING - ULTRASOUND is a useful alternative/adjunct to MRI for assessing posteromedial-corner pathologies including semimembranosus tendinopathy, and MRI characterises the tendon and excludes meniscal and other causes.
- MANAGEMENT is NON-OPERATIVE first: relative REST/activity modification, ECCENTRIC and progressive loading rehabilitation, and correction of training load and biomechanics. Biopsy studies of hamstring tendinopathy show TENDINOSIS - a degenerative, not inflammatory, process - which is the argument for load-based rehabilitation over anti-inflammatory-led treatment.
- BE CAUTIOUS WITH THE CORTICOSTEROID INJECTION. Across 41 randomised trials and 2,672 participants, corticosteroid reduced tendinopathy pain in the SHORT term but the effect was REVERSED at intermediate and long term - injected patients did worse by a year than those given no intervention. One of 991 injected participants (0.1%) sustained a TENDON RUPTURE. No trial has studied injection at the semimembranosus, and the authors warn against generalising between tendon sites. Use it to create a window for rehabilitation, not as the treatment.
- DISTINGUISH THE DIAGNOSTIC from the THERAPEUTIC injection: a local-anaesthetic block that abolishes the pain confirms the tendon as the source and is a valuable tie-breaker; that is a separate decision from injecting steroid.
- SURGERY is rarely required and is reserved for refractory cases, after a thorough non-operative programme and confirmation that the semimembranosus insertion is genuinely the pain source. No surgical series exists for the DISTAL insertion; in 103 cases of PROXIMAL hamstring tendinopathy, results were excellent or good in 92 and 80 of 90 returned to their previous sporting level, but it took a mean of 5 months (range 2-12) - counsel months, not weeks.
- KNOW THE POST-ARTHROPLASTY PRESENTATION. Semimembranosus tendonitis belongs on the differential of the unexplained painful TOTAL KNEE REPLACEMENT: posteromedial pain within a year, worse on walking and especially on RISING FROM A CHAIR, with good motion and a well-aligned prosthesis and no evidence of infection. In 6 such patients from over 700 arthroplasties, excising the un-released REFLECTED arm of the tendon relieved the pain completely in 5.
- “Semimembranosus tendinopathy = overuse tendinopathy at the distal SM insertion (posteromedial tibia) = chronic POSTEROMEDIAL knee pain; tender over the insertion, worse on RESISTED KNEE FLEXION; running/cutting athletes.
- “Differential (posteromedial corner): posterior-horn medial meniscus tear, pes anserine bursitis (more anteromedial), popliteal/Baker's cyst, posteromedial-corner/MCL pathology, medial OA - localise + image.
- “Ultrasound (and MRI) characterise it and exclude meniscal pathology - though no accuracy figure exists at this insertion. Management NON-OPERATIVE first (rest, eccentric loading, correct training load); surgery rare.
- “STEROID CAVEAT: across 41 RCTs / 2,672 participants, corticosteroid helped short-term but the effect REVERSED at 26 and 52 weeks, with 0.1% tendon rupture. Use it to open a rehabilitation window, not as treatment. A diagnostic local-anaesthetic block is a different thing.
- “Don't forget the PAINFUL TKA: posteromedial pain within a year, worse rising from a chair, good alignment, no infection - excising the un-released reflected SM arm cured 5 of 6.
Chronic posteromedial knee pain, tender over the semimembranosus insertion, worse on resisted knee flexion, in a running/cutting athlete = semimembranosus tendinopathy.
Posterior-horn medial meniscus tear, pes anserine bursitis (more anteromedial), popliteal/Baker's cyst, posteromedial-corner/MCL pathology, medial OA. Ultrasound/MRI help.
Features, Differential & Management
Semimembranosus tendinopathy is an overuse tendinopathy of the distal semimembranosus at its posteromedial tibial insertion - a cause of chronic posteromedial knee pain, with localised tenderness over the insertion and pain on resisted knee flexion, typically in running/cutting athletes. The differential is the posteromedial-corner group: posterior-horn medial meniscus tear, pes anserine bursitis (more anteromedial), popliteal/Baker's cyst, posteromedial-corner/MCL pathology, and medial- compartment OA. Ultrasound (and MRI) characterise the tendinopathy and exclude meniscal/other pathology. Management is non-operative first - rest, eccentric/progressive loading, NSAIDs, image-guided injection, and correcting training load/biomechanics - with surgery rarely needed (refractory cases).
The clinical caution with semimembranosus tendinopathy is that posteromedial knee pain has several possible sources, and the semimembranosus insertion is only one. A posterior-horn medial meniscus tear in particular can present with very similar posteromedial pain, as can pes anserine bursitis (usually a little more anteromedial), a popliteal (Baker's) cyst, posteromedial-corner or medial collateral pathology, and referred medial-compartment osteoarthritis. So before attributing the pain to the tendon and committing to prolonged tendinopathy treatment, the source should be confirmed by precisely localising the tenderness to the semimembranosus insertion, provoking the pain with resisted knee flexion, and using imaging - ultrasound is a useful adjunct/alternative to MRI for the posteromedial corner, and MRI characterises the tendon and excludes a meniscal tear. Treatment is non-operative first, with rest, eccentric and progressive loading, NSAIDs and an image-guided injection for refractory cases, alongside correction of the overuse cause (training load, biomechanics); surgery is rarely necessary and is reserved for genuinely refractory cases once the diagnosis is secure.
The Corticosteroid Injection: Short-Term Gain, Long-Term Loss
An image-guided corticosteroid injection is a reasonable option for a refractory insertional tendinopathy, but it must be offered with the caveat that the best evidence in tendinopathy shows the benefit reverses over time.
- The landmark evidence. A systematic review of 41 randomised trials covering 2,672 participants found consistently across high-quality trials that corticosteroid injection reduced pain in the short term but that this effect was reversed at intermediate and long term. For lateral epicondylalgia the short-term effect was large (SMD 1.44, 95% CI 1.17-1.71), yet at 26 weeks and at 52 weeks no intervention was favoured over injection (SMD −0.40, 95% CI −0.67 to −0.14 at intermediate term; −0.31, −0.61 to −0.01 at long term). In other words, patients injected did worse by a year than those left alone.
- Serious harm is rare but real. Among 991 participants who received corticosteroid injections in trials reporting adverse events, one (0.1%) sustained a tendon rupture. Rare, but it is the complication to mention when consenting, particularly for a load-bearing insertional tendon.
- The honest caveat, which the same authors insist on. Effects varied by tendon site, and the authors explicitly warn that the response to injection should not be generalised across sites - short-term efficacy in rotator-cuff tendinopathy, for instance, was not clear. No trial has studied injection at the semimembranosus insertion at all, so the figures above are the best available guide, not site-specific evidence.
- What this changes in practice. Load-based rehabilitation remains the mainstay; the injection buys a window of analgesia in which to rehabilitate rather than being a treatment in itself, and repeated injections into an insertional tendon are not supported.
The local-anaesthetic injection used to confirm that the semimembranosus insertion is the pain source is a diagnostic test, and a valuable one - abolition of the pain identifies the tendon. That is a separate decision from injecting corticosteroid for treatment, which carries a reversal of benefit by six to twelve months and a small rupture risk. Do not let a positive diagnostic block automatically become a therapeutic steroid injection.
The Painful Posteromedial Knee After Total Knee Replacement
A presentation worth knowing for the fellowship exam, because it belongs on the differential of the unexplained painful total knee arthroplasty. In a series drawn from more than 700 total knee arthroplasties performed over eight years, 6 patients developed posteromedial knee pain within a year of surgery.
- The clinical picture was consistent. Pain increased on walking and especially on rising from a chair. All six were women, and all had good knee motion and well-aligned, well-fixed implants - so the pain was not explained by the arthroplasty itself. There were no signs of low-grade infection, which must still be excluded first in any painful replaced knee.
- A diagnostic block confirmed the source. Injection of local anaesthetic relieved the pain, briefly, in all six.
- The mechanism and the fix. The reflected portion of the semimembranosus tendon, which had not been released during the arthroplasty, was the culprit; excision relieved the pain completely in 5 of 6, with improvement in the sixth.
- Read the denominator honestly. Six cases from over 700 arthroplasties is roughly 1% - and since this is a retrospective single-centre series with no stated follow-up duration for the six, it establishes the entity and a plausible remedy rather than a reliable incidence or success rate.
The Semimembranosus's Multi-Armed (Five-Arm) Insertion
- Direct (tibial) arm - the main tendon, inserting into the tuberculum tendinis on the posteromedial tibia just below the joint line, deep and posterior to the superficial MCL. This is the arm at which the insertional tendinopathy characteristically occurs.
- Anterior (reflected) arm - turns anteriorly deep to the superficial MCL to insert on the medial tibia beneath it.
- Oblique popliteal ligament (OPL) arm - a broad capsular expansion running superolaterally across the posterior capsule to form the oblique popliteal ligament, reinforcing the posterior capsule against hyperextension.
- Posterior oblique ligament (POL) / capsular arm - an expansion blending into the posteromedial capsule and POL.
- Arm to the posterior horn of the medial meniscus (and popliteus fascia) - a slip attaching to the posterior horn of the medial meniscus.
Function. The semimembranosus flexes and internally rotates the knee and is the principal dynamic stabiliser of the posteromedial corner; through its meniscal arm it retracts the posterior horn of the medial meniscus during flexion, protecting it from impingement - which is precisely why posteromedial-corner pain from the tendon and from a posterior-horn meniscal tear can be so hard to separate.
Q: Describe the semimembranosus's distal insertion and its functional significance.
A: The distal semimembranosus fans into five arms - the direct (tibial) arm to the tuberculum tendinis on the posteromedial tibia (where the tendinopathy occurs), an anterior (reflected) arm deep to the MCL, the oblique popliteal ligament arm across the posterior capsule, a posterior oblique ligament/capsular arm, and an arm to the posterior horn of the medial meniscus. It flexes and internally rotates the knee, is the main dynamic stabiliser of the posteromedial corner, and via its meniscal arm retracts the posterior horn of the medial meniscus in flexion - which is why tendon pain and a posterior-horn meniscal tear are such close differentials.
Distinguishing It from a Posterior-Horn Medial Meniscus Tear
- Site of tenderness. Precisely over the semimembranosus insertion (posteromedial tibia, at and just below/behind the joint line) versus along the posteromedial joint line for a meniscal tear.
- Provocation. Reproduced by resisted knee flexion (loading the tendon) versus by joint-line rotation tests - McMurray (deep flexion with external rotation and extension), Thessaly (weight-bearing rotation) and Apley grind - for the meniscus.
- Mechanical symptoms. None with the tendinopathy versus catching, locking, giving-way and an effusion with a meniscal tear.
- Onset. Gradual overuse (running/cutting) versus a twisting/loading event (or an insidious degenerate tear in older patients).
- Imaging. Ultrasound/MRI show a thickened, hypoechoic or high-signal degenerate tendon at the insertion versus MRI showing a meniscal signal that reaches the articular surface.
A diagnostic image-guided local-anaesthetic injection to the semimembranosus insertion (pain relief confirms the tendon as the source) is a useful tie-breaker before committing to prolonged tendinopathy treatment.
Q: How do you clinically distinguish semimembranosus tendinopathy from a posterior-horn medial meniscus tear?
A: The tendinopathy gives point tenderness over the SM insertion and pain on resisted knee flexion, with no mechanical symptoms and a gradual overuse onset. A posterior-horn meniscal tear gives posteromedial joint-line tenderness, positive rotation tests (McMurray/Thessaly/Apley), mechanical catching/locking and an effusion, often after a twisting event. MRI shows tendon degeneration versus a surface-reaching meniscal signal, and a diagnostic local-anaesthetic injection to the SM insertion that relieves the pain confirms the tendon as the source.
Mnemonics & Memory Aids
POSTEROMEDIAL
Hook:Posteromedial pain, Resisted flexion, Overuse, Meniscus differential, Exclude neighbours, Diagnose (US/MRI) + non-op first.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A runner has chronic posteromedial knee pain, tender over the semimembranosus insertion and worse on resisted flexion. How do you approach it?”
What it is
- Overuse tendinopathy of the distal semimembranosus (posteromedial tibial insertion)
- Cause of chronic posteromedial-corner knee pain
- Running/cutting/repetitive-flexion athletes
Presentation & differential
- Localised posteromedial tenderness; worse on resisted knee flexion
- Differential: posterior-horn medial meniscus, pes anserine bursitis (more anteromedial)
- Popliteal/Baker's cyst; posteromedial corner/MCL; medial OA
Diagnosis & management
- Ultrasound (and MRI) characterise the tendon + exclude meniscal pathology (no accuracy figure published)
- Non-operative first: rest, eccentric/progressive loading; correct training load/biomechanics
- Steroid injection: 41 RCTs / 2,672 participants - short-term gain REVERSED at 26 and 52 weeks; 0.1% rupture
- Diagnostic local-anaesthetic block confirms the source; that is not the same decision as a steroid injection
- Surgery rare; proximal hamstring series - 80 of 90 back to sport, but mean 5 months (range 2-12)
The painful TKA scenario
- Posteromedial pain within a year of arthroplasty, worse walking and especially RISING FROM A CHAIR
- Good motion, well-aligned prosthesis, no evidence of infection (still exclude it first)
- Local-anaesthetic block relieves it; culprit is the un-released REFLECTED arm
- Excision relieved pain completely in 5 of 6 patients (from over 700 arthroplasties)
Evidence & Key Studies
Ultrasonography for posteromedial-corner pathologies including semimembranosus tendinopathy
- A NARRATIVE REVIEW, not a diagnostic-accuracy study - it recommends ultrasound but reports no sensitivity, specificity or yield figure for detecting semimembranosus tendinopathy, and none has been published.
- The posteromedial corner (PMC) is a common location for knee pain, with frequent causes including posterior medial meniscus pathology, articular cartilage damage, popliteal cysts and semimembranosus tendinopathy.
- While MRI is the gold standard, ultrasonography is a useful alternative for assessing the posteromedial corner, with particular value in evaluating semimembranosus tendinopathy.
- Accurate localisation and imaging assessment of the posteromedial corner are essential for appropriate treatment.
Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials
- 3,824 trials screened, 41 randomised trials meeting quality criteria included, providing data on 2,672 participants across tendinopathy sites - by far the strongest evidence bearing on injection therapy for an insertional tendinopathy.
- Corticosteroid injection consistently reduced pain in the SHORT term but the effect was REVERSED at intermediate and long term. For lateral epicondylalgia: short-term SMD 1.44 (95% CI 1.17-1.71, p less than 0.0001) favouring injection, but no intervention favoured at intermediate term (SMD −0.40, 95% CI −0.67 to −0.14, p less than 0.003) and long term (−0.31, −0.61 to −0.01, p = 0.05).
- SAFETY: of 991 participants receiving corticosteroid injections in trials that reported adverse events, one (0.1%) sustained a serious adverse event - tendon rupture.
- Short-term efficacy for rotator-cuff tendinopathy was NOT clear, and the authors state explicitly that response to injection should not be generalised because effects vary between tendinopathy sites.
- Limitations for our purposes: NO included trial studied the semimembranosus insertion. The strongest data are from lateral epicondylalgia, so applying these figures to the semimembranosus is an extrapolation the authors themselves caution against - but it is the best guidance available, and there is nothing site-specific to replace it.
Semimembranosus tendonitis after total knee arthroplasty: good outcome after surgery in 6 patients
- Six patients out of more than 700 total knee arthroplasties performed 1992-2000 developed posteromedial knee pain within a year of surgery - roughly 1%, though as a retrospective single-centre series this is an approximate frequency rather than a measured incidence.
- The pain increased on walking and especially on RISING FROM A CHAIR. All six were women, all had good knee motion and well-aligned prostheses, and there were no signs of low-grade infection.
- Injection of local anaesthetic relieved the pain temporarily in all six, confirming the tendon as the source before any surgery.
- Excision of the REFLECTED PORTION of the semimembranosus tendon - which had not been divided during the arthroplasty - relieved pain completely in 5 and improved it in 1.
- Limitations: six patients, no stated follow-up duration, no comparison group and no validated outcome score. It establishes the entity and a plausible remedy, not a success rate.
Proximal hamstring tendinopathy: results of surgical management and histopathologic findings
- IMPORTANT CAVEAT ON SITE: this is PROXIMAL hamstring tendinopathy treated by semimembranosus tenotomy at the ischial origin, not distal insertional disease at the knee. It is included because no comparable surgical series exists for the distal semimembranosus, and because the same authors' warning about site-specific variation applies.
- Case series of 103 operated cases in athletes (58 men, 32 women, 13 bilateral), retrospectively analysed, with an average follow-up of 49 months (range 12-156).
- Results were excellent in 62, good in 30, fair in 5 and poor in 6. Of 90 patients, 80 returned to their pre-symptom level of sport, taking a mean of 5 months (range 2-12 months) - so counsel a months-long, not weeks-long, recovery after surgery.
- Biopsy of 15 operated tendons showed typical morphological features of tendinosis in every specimen, confirming a degenerative rather than inflammatory process - which is the pathological argument against anti-inflammatory-led treatment.
- Limitations: retrospective case series with a non-validated 4-category rating system, no control group, and surgeon-assessed outcomes; the denominator for return to sport (90) differs from the number of cases (103), so the figures are not directly comparable.
Semimembranosus tendinopathy as a recognised cause of posteromedial-corner knee pain and the value of ultrasonography alongside MRI come from the Pobozy review (DOI) - a narrative review reporting no accuracy figures. The injection data - the short-term benefit reversing at intermediate and long term, the effect sizes and confidence intervals, and the 0.1% tendon-rupture rate among 991 injected participants - come from Coombes (DOI), 41 randomised trials and 2,672 participants, none of them at the semimembranosus. The post-arthroplasty presentation and the outcome of excising the reflected arm come from Hendel (DOI), 6 patients. The surgical outcome figures and the tendinosis histology come from Lempainen (DOI), 103 cases of PROXIMAL hamstring tendinopathy - a different site. The five-arm anatomy, the overuse aetiology, the clinical presentation and the posteromedial differential are standard, well-established teaching.
What does not exist: there is no cohort study of distal semimembranosus tendinopathy, and therefore no published prevalence, no recovery time, no success rate for eccentric loading or injection, and no return-to-sport criterion specific to this tendon. No diagnostic-accuracy figure for ultrasound or MRI at this insertion has been reported, so "ultrasound is useful" is expert recommendation rather than measured performance. Any percentage quoted for the outcome of treating this specific tendinopathy would be an extrapolation from other sites, and the Coombes authors caution explicitly against exactly that generalisation.