Neurosurgical Emergency | Diagnostic Triad | Delayed Decompression = Irreversible Paralysis
- Classic triad present in only 10-30 percent at first presentation
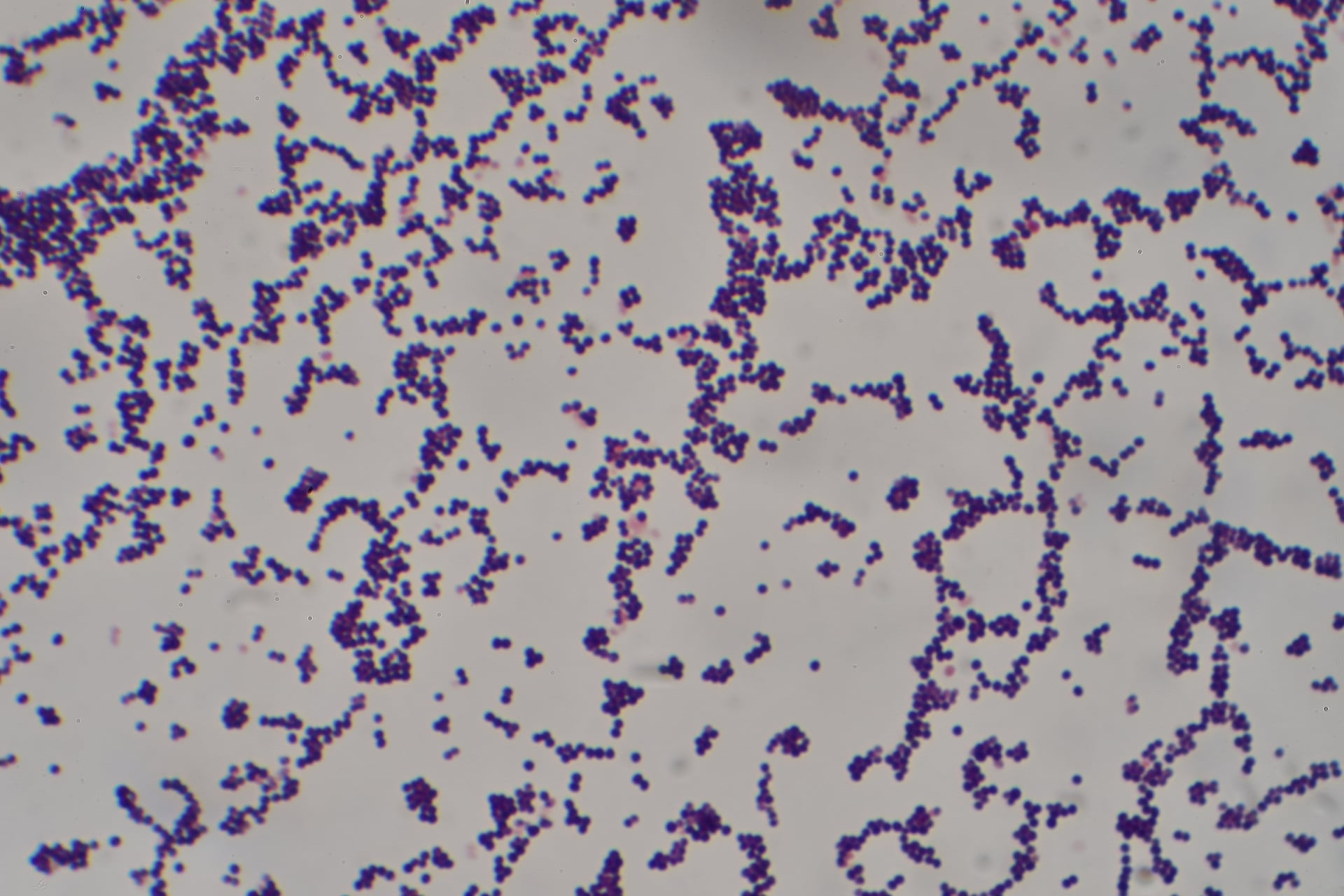
- S. aureus most common; gram-negatives and anaerobes in IVDU or post-op
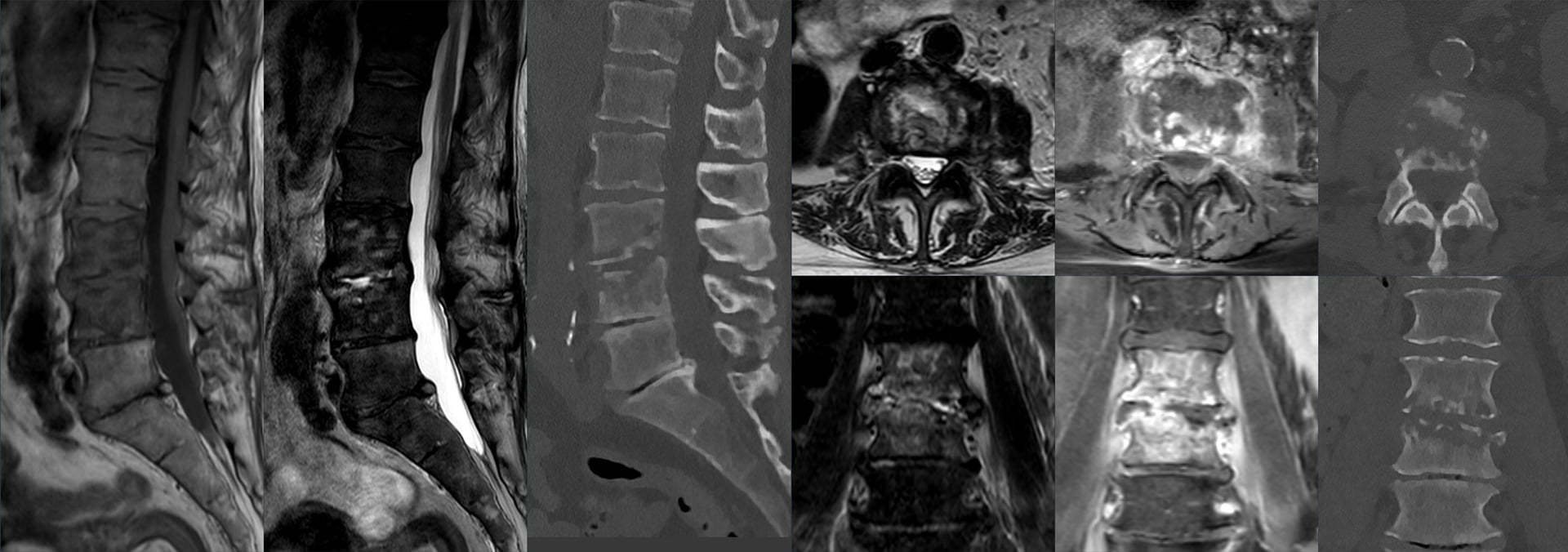
- MRI with gadolinium is investigation of choice; do not delay for CT
- Emergent surgical decompression plus IV antibiotics is standard of care
- Delay beyond 24 hours dramatically worsens neurologic outcome
- “Back pain + fever + any neuro sign = SEA until proven otherwise
- “IV drug use and diabetes are the strongest risk factors
- “White cell count and CRP can be normal early; do not rely on labs
- “Neurologic recovery is time-critical; document hourly neuro checks
Fever + spinal pain + neurologic deficit. The triad is classic but incomplete at presentation in over 70 percent of cases. Any two elements in a high-risk patient warrants urgent MRI.
IV drug use, diabetes, immunosuppression, recent spinal procedure, endocarditis. These patients develop SEA at higher rates and progress faster to paralysis.
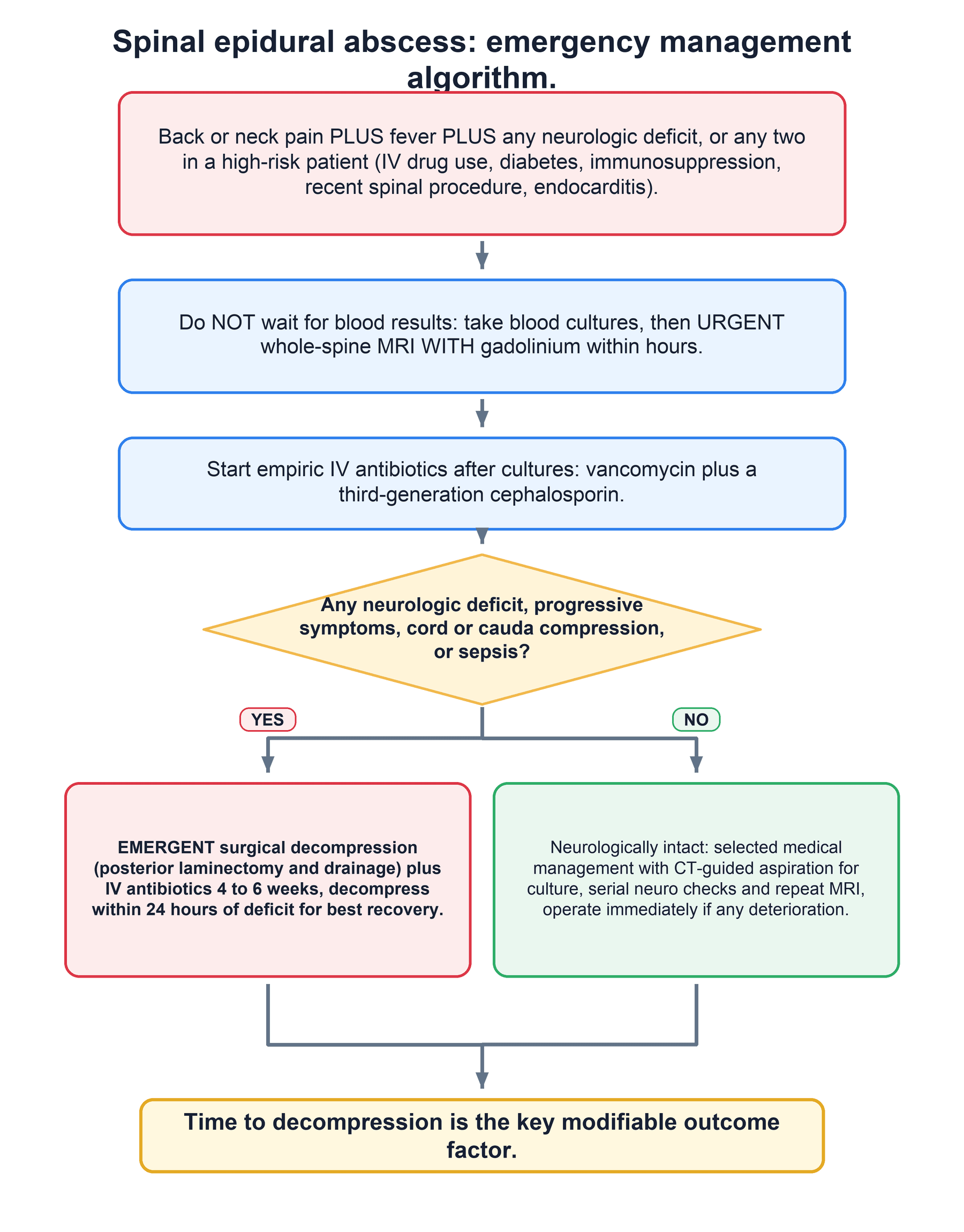
MRI with gadolinium contrast is mandatory. CT myelogram is alternative only if MRI contraindicated. Do not wait for blood cultures or inflammatory markers.
Emergent decompression + IV antibiotics. Do not delay surgery for medical optimisation once diagnosis confirmed. Neurologic deterioration can occur within hours.
- Risk Profile
- IVDU or diabetic
- Action
- Urgent MRI within 4 hours
- Key Pearl
- Triad incomplete but high suspicion
- Risk Profile
- Any risk factor present
- Action
- Emergent MRI + surgical consult
- Key Pearl
- Stage 2 disease; decompression now
- Risk Profile
- Delayed presentation
- Action
- Immediate OR decompression
- Key Pearl
- Less than 24 hours critical window
DICERisk Factor Categories
Hook:DICE the odds - screen every diabetic and IVDU with back pain for SEA!
Overview and Epidemiology
Spinal epidural abscess is a neurosurgical emergency with potentially devastating consequences. The classic diagnostic triad of fever, spinal pain and neurologic deficit is present in fewer than one-third of patients at first presentation. Delayed diagnosis leads to irreversible paralysis, and mortality remains 5-15 percent even with modern care. Early recognition in high-risk populations (IV drug users, diabetics) followed by immediate MRI and emergent decompression is the only way to preserve neurologic function.
- Incidence 0.2-2 per 10,000 hospital admissions worldwide
- Male predominance (55-70 percent)
- Mean age 50-60 years but rising in younger IVDU populations
- Thoracic and lumbar spine most common (thoracic 50 percent, lumbar 35 percent)
- Cervical involvement carries highest morbidity
- Overall mortality 5-15 percent despite treatment
- Permanent paralysis in 15-30 percent of delayed cases
- Bowel/bladder dysfunction common sequela
- Recurrence rate 5-10 percent after treatment
- Poorer outcomes with cervical location and delayed surgery
Pathophysiology
Spinal epidural abscess forms via three main routes: (1) haematogenous spread from distant foci (skin, urinary tract, endocarditis) most common in IVDU and diabetics; (2) contiguous extension from adjacent discitis, vertebral osteomyelitis or paravertebral abscess; (3) direct inoculation after spinal procedures or trauma. Once in the epidural space the infection spreads longitudinally because the epidural space is a continuous compartment with loose areolar tissue and valveless venous plexus that facilitates rapid cephalad and caudad extension. The resulting mass effect plus inflammatory oedema and vascular compromise produce cord or cauda equina compression.
Staphylococcus aureus 50-70 percent of cases (MRSA rising) Gram-negative bacilli 15-20 percent (E. coli, Pseudomonas in IVDU) Streptococci and anaerobes in 5-10 percent Polymicrobial in post-operative and sacral abscesses Culture-negative in up to 30 percent after antibiotics started
Posterior epidural space wider (especially thoracic) hence posterior abscesses predominate Anterior abscesses often from vertebral osteomyelitis Cord ends at L1-L2; lumbar abscesses compress cauda equina Segmental arteries and radicular feeders vulnerable to thrombosis Epidural venous plexus allows bidirectional spread
Neurological injury in SEA is not purely mechanical — there are two mechanisms, and recognising the second explains why a deficit can be out of proportion to the visible compression and why some patients deteriorate despite a technically adequate decompression:
- Direct mechanical compression of the cord or cauda equina by the abscess and inflammatory mass — the component that surgery relieves.
- Vascular compromise — septic thrombophlebitis of the valveless epidural venous plexus, and thrombosis/arteritis of segmental and radicular feeding vessels, causing ischaemic (often venous) cord infarction. This component is largely irreversible. It is why rapid, profound neurological loss can occur with only modest compression, and why outcome correlates with the duration and severity of deficit before treatment rather than with abscess size alone.
Classification and Types
Classification by Location and Extent
- Frequency
- Most common (40-50 percent)
- Clinical Features
- Back pain, sensory level, paraparesis
- Surgical Approach
- Posterior laminectomy decompression
- Frequency
- 30-35 percent
- Clinical Features
- Radicular pain, leg weakness, retention
- Surgical Approach
- Decompression + possible fusion
- Frequency
- 10-15 percent
- Clinical Features
- Neck pain, quadriplegia risk highest
- Surgical Approach
- Anterior or posterior decompression
- Frequency
- Rare (less than 5 percent)
- Clinical Features
- Rapid multi-level deterioration
- Surgical Approach
- Multi-stage or skip laminectomies
Posterior abscesses are easier to drain via laminectomy; anterior abscesses often require corpectomy and reconstruction when associated with vertebral destruction.
Clinical Assessment
- Back or neck pain: Severe, localised, worse at night, not relieved by rest
- Fever or rigors: Present in majority but may be absent in immunocompromised
- Risk factors: IV drug use, diabetes, recent procedure, endocarditis, UTI
- Neurologic symptoms: Weakness, numbness, bowel or bladder change, gait disturbance
- Duration: Rapid progression over days is typical; chronic forms exist in TB
- Vital signs: Fever, tachycardia, possible hypotension if septic
- Spine: Localised tenderness, paraspinal spasm, limited ROM
- Neurologic: Sensory level, motor weakness, hyperreflexia or areflexia, upgoing plantars
- Sphincters: Urinary retention, reduced anal tone, saddle anaesthesia
- Source: Look for skin infection, injection sites, heart murmur
Perform urgent MRI if any of the following are present in a patient with back pain and fever:
- New or progressive lower-limb weakness
- Sensory level or dermatomal sensory loss
- Urinary retention or incontinence
- Saddle anaesthesia or reduced anal tone
- Hyperreflexia or Babinski sign suggesting cord compression
- Any new bowel or bladder dysfunction
- Distinguishing Features
- Triad + risk factors, rapid progression
- Investigation
- MRI with gadolinium
- Management
- Emergent decompression + antibiotics
- Distinguishing Features
- Insidious onset, no abscess on MRI
- Investigation
- MRI + blood cultures
- Management
- IV antibiotics, bracing, possible fusion
- Distinguishing Features
- Flank pain, positive urinalysis
- Investigation
- CT abdomen, urine culture
- Management
- IV antibiotics, drainage if needed
- Distinguishing Features
- Neck stiffness, photophobia, no focal deficit
- Investigation
- LP after imaging
- Management
- IV antibiotics, steroids
Investigations
Investigation Sequence
Full blood count, CRP, ESR, blood cultures x3 Inflammatory markers often elevated but can be normal early or in immunocompromised patients. Blood cultures positive in 50-70 percent and guide targeted therapy.
Gold-standard imaging. Shows enhancing epidural collection, cord or cauda compression, associated discitis or osteomyelitis. Sagittal and axial T1 post-contrast sequences essential. Do not delay for CT if MRI available.
Alternative when MRI impossible. Demonstrates block to contrast flow and epidural mass effect. Less sensitive for soft-tissue detail and associated vertebral infection.
Echocardiogram for endocarditis (high association with IVDU SEA). CT chest/abdomen/pelvis to identify distant source if not obvious.
MRI with gadolinium is the only imaging modality that reliably diagnoses spinal epidural abscess and defines the extent of cord compression. Plain radiographs are normal early and CT without contrast misses the abscess. Never delay MRI for laboratory results; the clinical triad plus risk factors is enough to order the scan.
FANClassic Diagnostic Triad
Hook:Remember FAN: Fever, Axial pain, Neurologic deficit - the SEA triad!
Management Algorithm
Emergent Surgical Decompression
Indications: Any neurologic deficit, progressive symptoms, large abscess with cord compression, failure of medical therapy, or sepsis.
Surgical Principles
Prone for posterior thoracic/lumbar abscesses on radiolucent table with Mayfield or Gardner-Wells traction if cervical. Lateral decubitus for anterior cervical approaches.
Posterior laminectomy over the length of the abscess (usually 3-5 levels) allows drainage and cord decompression. Preserve facet joints to avoid instability. Anterior cervical abscesses require anterior cervical decompression and fusion.
Evacuate all purulent material, send multiple cultures (aerobic, anaerobic, fungal, mycobacterial). Irrigate copiously. Avoid cord retraction. Intraoperative ultrasound confirms complete decompression.
Instrumented fusion indicated when extensive laminectomy, pre-existing spondylolisthesis, or vertebral destruction from osteomyelitis. Use titanium implants.
Layered closure over suction drains. Continue IV antibiotics for 4-6 weeks post-operatively, guided by cultures. Serial CRP monitoring.
The single most important modifiable factor affecting outcome is time to decompression. Patients operated within 24 hours of neurologic deficit onset have significantly better recovery than those delayed beyond 36-48 hours. Document the exact time of first neurologic symptom and time of skin incision.
A neurologically intact patient with SEA may occasionally be treated with antibiotics and close observation (often after CT-guided aspiration to obtain the organism) — but failure of medical management is common and can be sudden and catastrophic, so the examiner wants the predictors that argue against it. Independent risk factors for failure of non-operative treatment include diabetes mellitus, a high inflammatory burden (CRP greater than about 115 mg/L, white cell count greater than about 12.5), positive blood cultures / bacteraemia (especially MRSA), age over about 65, and any neurologic compromise. The more that are present, the lower the threshold for early surgery. A patient managed medically needs a confirmed organism, serial neurological checks and repeat MRI, with immediate decompression at the first sign of deterioration.
PINSSurgical Indications
Hook:PINS down the diagnosis and operate - progressive deficit is the trigger!
Complications
The dominant complication of spinal epidural abscess is permanent neurological deficit — the very outcome that urgent decompression aims to prevent.

- Permanent neurological deficit / paralysis — the major morbidity. Outcome is determined chiefly by the severity and duration of the deficit before decompression; a complete deficit present for more than 24–48 hours rarely recovers fully, whereas patients decompressed before or soon after deficit onset do far better.
- Cauda equina syndrome — bladder/bowel dysfunction and saddle anaesthesia from lumbosacral thecal sac compression, as shown above.
- Sepsis and septic shock — Staphylococcus aureus (including MRSA) is the commonest organism; bacteraemia and metastatic infection (endocarditis, septic arthritis) may coexist.
- Associated vertebral osteomyelitis / discitis — contiguous bone and disc infection frequently accompanies the abscess and may cause later deformity or instability.
- Recurrence / treatment failure — incomplete drainage, inadequate or premature cessation of antibiotics, or failure of non-operative management (which carries a real risk of sudden, irreversible deterioration) can lead to recurrence requiring further surgery.
- Mortality — historically very high; with modern MRI, surgery and antibiotics, contemporary mortality is roughly 5–15%, driven by sepsis and comorbidity in older, diabetic or immunocompromised patients.
Guidelines, Registries & Global Practice
- Rising incidence linked to opioid epidemic and increasing IV drug use worldwide
- Higher rates reported in Eastern Europe, North America and Australia in IVDU populations
- TB-related SEA more common in endemic regions (India, sub-Saharan Africa)
- Post-operative SEA incidence 0.5-2 percent after spinal surgery globally
- High-resource centres: immediate MRI, 24/7 spine on-call, ICU monitoring
- Resource-limited settings: rely on clinical diagnosis and transfer for MRI/surgery
- Antibiotic stewardship varies; culture-directed therapy universal principle
- Multidisciplinary input (infectious disease, spine surgery, rehabilitation) standard in developed systems
- Diagnosis
- MRI with gadolinium; blood cultures before antibiotics
- Antibiotics
- Vancomycin + 3rd-gen cephalosporin empiric
- Surgery Timing
- Emergent decompression for any deficit
- Diagnosis
- Urgent MRI within 4 hours if red flags
- Antibiotics
- Broad-spectrum IV within 1 hour of diagnosis
- Surgery Timing
- Same-day surgery for progressive deficit
- Diagnosis
- Whole-spine MRI to exclude skip lesions
- Antibiotics
- Culture-guided therapy 4-6 weeks minimum
- Surgery Timing
- Decompression within 24 hours of deficit
There is no dedicated international registry for spinal epidural abscess outcomes. Data derive from institutional series and administrative databases. Neurologic recovery is best tracked with ASIA or Frankel grading at presentation, post-operatively, and at 3-6 months. Documentation of exact time from symptom onset to decompression is essential for audit and research.
Controversies & Areas of Uncertainty
Patients with SEA but no neurologic deficit may be managed with antibiotics and close observation in selected cases. However, any new deficit mandates immediate surgery. The threshold for operating on purely pain-and-fever presentations remains debated.
Four to six weeks of IV therapy is conventional, but no high-quality trial defines the minimum effective duration. Longer courses are used when vertebral osteomyelitis coexists. Oral step-down regimens are increasingly explored.
Some surgeons advocate limited laminectomy over the maximal abscess diameter; others perform wide decompression to ensure complete evacuation. Intraoperative ultrasound helps confirm adequacy regardless of extent.
When laminectomy risks instability or when osteomyelitis has destroyed the vertebral body, instrumented fusion is added. The decision balances infection risk against mechanical stability; titanium implants are preferred.
MCQ Practice Points
Q: Where does the spinal cord end and what does this mean for lumbar epidural abscess? A: The spinal cord terminates at the L1-L2 disc level. Lumbar epidural abscess therefore compresses the cauda equina rather than the cord itself. This produces lower-motor-neuron signs (flaccid weakness, areflexia, urinary retention) rather than the upper-motor-neuron pattern seen with thoracic or cervical abscesses.
Q: What is the imaging modality of choice for suspected spinal epidural abscess and why? A: MRI with gadolinium contrast is the gold standard. It demonstrates the enhancing epidural collection, the degree of cord or cauda compression, and any associated discitis or osteomyelitis. CT without contrast or plain radiographs are inadequate; CT myelography is reserved for patients with MRI contraindications.
Q: Which patient populations are at highest risk for spinal epidural abscess? A: Intravenous drug users (haematogenous spread from skin flora), diabetics (immune dysfunction and microvascular disease), immunocompromised patients (steroids, HIV, chemotherapy), and those with recent spinal procedures or endocarditis. Up to 70 percent of cases occur in patients with one or more of these risk factors.
Q: What is the definitive treatment for a patient with spinal epidural abscess and neurologic deficit? A: Emergent surgical decompression (usually posterior laminectomy) plus intravenous antibiotics. Antibiotics alone are insufficient once neurologic deficit is present. Surgery must be performed within 24 hours of deficit onset for optimal recovery; delay beyond this window significantly worsens outcome.
Q: What is the most common causative organism and what empiric antibiotic regimen is appropriate? A: Staphylococcus aureus (including MRSA) accounts for 50-70 percent of cases. Empiric therapy is vancomycin plus a third-generation cephalosporin (ceftriaxone) pending culture results. Add metronidazole if anaerobic coverage is required. Duration is typically 4-6 weeks IV.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 34-year-old man with known intravenous heroin use presents with 4 days of severe mid-thoracic back pain and fever. He now reports numbness below the umbilicus and difficulty walking. On examination he has a sensory level at T10, 3/5 bilateral leg weakness and urinary retention. What is your diagnosis and immediate management?”
“A 58-year-old diabetic woman is transferred from another hospital with 10 days of lumbar back pain and progressive bilateral leg weakness. She is now unable to walk and has been catheterised for urinary retention for 48 hours. MRI performed today shows a large posterior lumbar epidural abscess from L2 to L5 with cauda equina compression. She had been treated with oral antibiotics for presumed discitis. How do you manage her?”
Diagnostic Triad and Red Flags
- Fever + severe spinal pain + any neurologic deficit = SEA until proven otherwise
- IV drug use and diabetes are the strongest risk factors worldwide
- Triad complete in only 10-30 percent at first presentation
- Urinary retention, sensory level or progressive weakness demand immediate MRI
Investigation Sequence
- Blood cultures x3 before antibiotics; CRP/ESR supportive but not diagnostic
- MRI with gadolinium contrast is mandatory within 4 hours of suspicion
- Image the entire spine to exclude skip lesions or pan-spinal disease
- CT myelogram only if MRI contraindicated
Microbiology and Antibiotics
- S. aureus (including MRSA) causes 50-70 percent of cases
- Empiric regimen: vancomycin plus ceftriaxone (add metronidazole if needed)
- Culture all operative specimens (aerobic, anaerobic, mycobacterial, fungal)
- IV antibiotics for minimum 4-6 weeks; longer with osteomyelitis
Surgical Indications and Timing
- Any new or progressive motor deficit, cauda equina signs, or uncontrolled sepsis
- Decompression within 24 hours of neurologic deficit onset optimises recovery
- Posterior laminectomy for most posterior abscesses; anterior approach for cervical
- Intraoperative cultures and copious irrigation; consider fusion if instability
Prognosis and Monitoring
- Mortality 5-15 percent; permanent paralysis in 15-30 percent of delayed cases
- Hourly neurologic observations pre- and post-operatively
- Serial CRP to monitor response; repeat MRI if deterioration
- Multidisciplinary rehabilitation essential for residual deficit
Evidence Base and Key Trials
Nontuberculous spinal epidural infections
- Classic description of 20 cases establishing the diagnostic triad of fever, spinal pain and neurologic deficit
- Highlighted rapid progression from back pain to paralysis within days
- Emphasised importance of early diagnosis before irreversible cord damage
Bacterial spinal epidural abscess. Review of 43 cases and literature survey
- Retrospective review of 43 patients confirming S. aureus as dominant pathogen
- Demonstrated that neurologic outcome correlates directly with time to surgery
- Identified IV drug use and diabetes as major risk factors
Spinal epidural abscess: a meta-analysis of 915 patients
- Meta-analysis of 915 patients (1954-1997) confirming S. aureus predominance and that outcome is largely determined by the severity and duration of neurologic deficit before treatment
- Laminectomy plus antibiotics was the treatment of choice; mortality fell from 34% (1954-1960) to 15% (1991-1997)
- Most common risk factor was diabetes mellitus, followed by trauma, IV drug abuse and alcoholism; MRI is the diagnostic method of first choice
Spinal epidural abscess in clinical practice
- Review of clinical presentation, microbiology and management emphasising MRI diagnosis
- Highlighted that only minority present with classic triad; high index of suspicion required
- Advocated early surgical consultation and culture-directed antibiotics for 4-6 weeks