Seven-stage (0–VI) MRI-informed staging of femoral head osteonecrosis with lesion-size modifiers
- Steinberg is a seven-stage system (0–VI) for femoral head osteonecrosis that adds MRI-based lesion quantification and a stage for advanced arthrosis to the older Ficat classification.
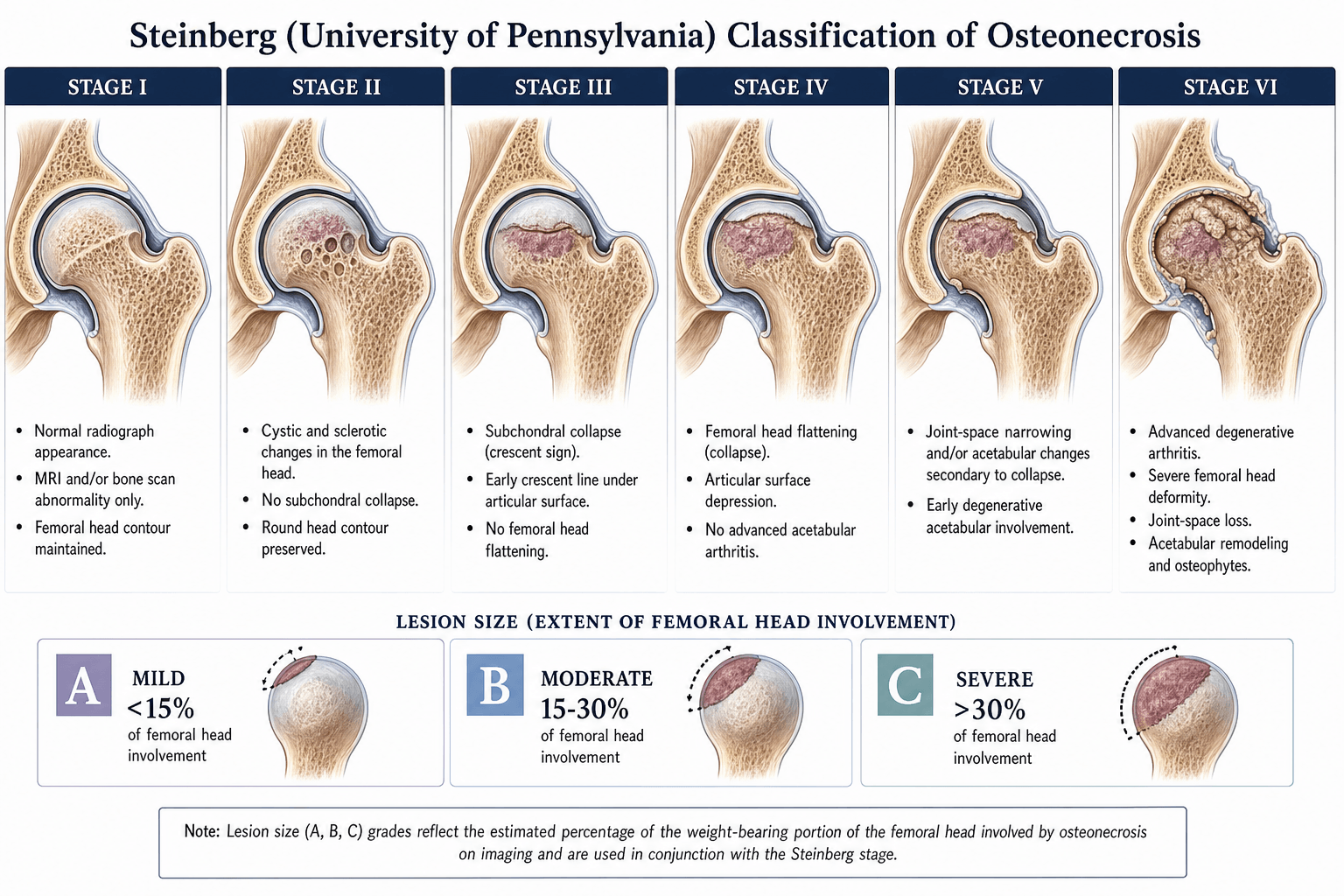
- Stages 0–II have no structural collapse — these are the stages where joint-preserving surgery (core decompression, osteotomy, bone grafting) has the best evidence. Stage III and beyond means the subchondral bone has failed and the prognosis for the native hip worsens sharply.
- Each stage carries a modifier A, B, or C quantifying the percentage of the femoral head affected on MRI: A is less than 15 percent, B is 15 to 30 percent, C is greater than 30 percent. The C modifier within any stage is the strongest predictor of future collapse.
- The system is more granular than Ficat because it separates pre-collapse MRI disease (Stages 0–II) from collapse (III) and post-collapse degeneration (IV–VI) and adds lesion size to every stage — the two variables an examiner will expect you to discuss.
- “Always report the stage AND the modifier (for example, Stage IIC, not just Stage II) — the modifier changes prognosis and management
- “Stage II versus Stage III is the critical boundary: no collapse versus collapse — joint-preserving surgery drops sharply in effectiveness after collapse
- “A Stage IIC hip (no collapse, large lesion) often has a worse prognosis than a Stage IIIA hip (collapsed but small lesion) — size matters
In the viva, the examiner wants you to distinguish pre-collapse (Stages 0–II) from post-collapse (Stage III onward) and to explain how the A, B, C modifier changes prognosis within any stage. A patient with Stage IIC (normal radiographs but greater than 30 percent head involvement on MRI) has a worse prognosis than Stage IIIA (collapse but less than 15 percent involvement). If you only give the stage and omit the modifier, you are not using the classification as intended.
The Steinberg Staging System

Steinberg and colleagues at the University of Pennsylvania published their system in 1995 to address the limitations of the Ficat and Arlet classification — principally that Ficat grouped all pre-collapse MRI disease into a single stage and did not quantify lesion size. The Steinberg system therefore separates seven radiographic stages (0 through VI) and adds an alphabetic modifier (A, B, or C) based on the proportion of the femoral head involved on MRI.
- Radiographs
- Normal
- MRI
- Normal or non-specific
- Collapse
- None — pre-clinical, histological diagnosis only
- Radiographs
- Normal
- MRI
- Abnormal signal (diffuse or focal)
- Collapse
- None
- Radiographs
- Sclerotic or cystic changes; no flattening
- MRI
- Abnormal signal — lesion measurable
- Collapse
- None
- Radiographs
- Crescent sign and/or subchondral fracture; early flattening
- MRI
- Abnormal — lesion now collapsed
- Collapse
- Present — subchondral collapse, head remains spherical or minimally flattened
- Radiographs
- Flattened femoral head; joint space preserved or minimally narrowed
- MRI
- Collapsed head, loss of sphericity
- Collapse
- Established collapse with loss of roundness
- Radiographs
- Flattened head; acetabular involvement (cysts, sclerosis, marginal osteophytes)
- MRI
- Secondary arthritis changes in acetabulum
- Collapse
- Collapse with secondary acetabular changes
- Radiographs
- Advanced degenerative joint disease — destroyed joint
- MRI
- End-stage arthritis
- Collapse
- Total joint destruction
Stage 0 is a diagnosis of exclusion. The patient has osteonecrosis risk factors, normal imaging, but a confirmatory histological diagnosis (for example from the contralateral hip or from biopsy). In practice it is rarely encountered in the exam and almost never in clinic. Stage I is the earliest clinically meaningful stage — the patient has hip pain or is being screened, radiographs are normal, and MRI picks up the lesion.
0 I II III IV V VIThe seven stages
Hook:The critical hinge is between II and III: before III the head is intact, from III onward it has collapsed.
The crescent sign (Stage III) represents a subchondral fracture. It appears on lateral or frog-lateral radiographs as a radiolucent line parallel to the articular surface and signifies that the necrotic segment has lost structural support and is beginning to collapse. Once the crescent appears, the clock is ticking on joint-preserving options.
MRI Signs of Osteonecrosis
Steinberg staging relies on MRI from Stage I onward, so the examiner expects you to know the MRI signs that actually make the diagnosis. MRI is the most sensitive and specific modality (both around 99 percent) and detects disease long before radiographs change.
- Double-line sign (the characteristic sign): on T2-weighted images, an inner bright line (hypervascular granulation tissue at the repair interface) running parallel to an outer low-signal line (sclerotic reactive bone) at the margin of the necrotic segment. It is the single most characteristic MRI feature of osteonecrosis.
- Geographic lesion with a reactive interface: a well-demarcated, usually anterosuperior subchondral segment ringed by a serpiginous low-signal rim on T1 (the interface between dead and living bone). The central necrotic marrow often retains fat signal early in the disease.
- Bone marrow oedema: diffuse low T1 / high T2 signal extending into the head and neck. It is non-specific, but in established osteonecrosis it correlates with pain and impending collapse and is a poor prognostic sign.
- Subchondral fracture line: a low-signal subchondral line, the MRI correlate of the radiographic crescent sign, marking the transition to Steinberg Stage III.
Quantification of Head Involvement (A, B, C)
The Steinberg system adds an alphabetic modifier to every stage (except 0 and VI, where quantification does not change management). The modifier is determined by measuring the proportion of the femoral head involved by the osteonecrotic lesion on MRI — specifically on the coronal T1-weighted images where the low-signal lesion is most clearly delineated against the bright fatty marrow.

- Head Involvement
- Less than 15 percent
- Prognostic Significance
- Best prognosis within any stage — lowest rate of collapse progression
- Head Involvement
- 15 to 30 percent
- Prognostic Significance
- Intermediate risk — meaningful proportion of the weight-bearing dome affected
- Head Involvement
- Greater than 30 percent
- Prognostic Significance
- Highest risk of collapse — the single most important negative prognostic factor
- Column 4
- danger
How to measure on MRI. On the mid-coronal T1-weighted image, identify the arc of low signal representing the necrotic segment. The proportion of the femoral head involved is estimated as a percentage of the head's cross-sectional area. The exact method varies (some use the necrotic angle method of Kerboul), but the principle is the same: the larger the necrotic segment relative to the weight-bearing dome, the worse the prognosis.
A B CThe A, B, C modifiers
Hook:The 15 and 30 percent thresholds split lesion size into three prognostic groups. Modifier C at any stage is the strongest single predictor of progression to collapse.
The Kerboul combined necrotic angle. This is an alternative quantitative method sometimes used alongside Steinberg. Two angles are measured on MRI: the angle of the necrotic arc on the coronal image and the angle on the sagittal image. The combined angle of 200 degrees or greater correlates strongly with collapse. A combined angle less than 200 degrees favours non-operative or joint-preserving surgical management.
Prognostic Implications and Clinical Decision-Making
The Steinberg classification guides treatment by combining the stage (structural integrity of the head) with the modifier (size of the necrotic lesion). Two variables matter: is the head still intact, and how much of it is dead?
- Modifier
- A
- Typical Approach
- Observation, protected weight-bearing, address risk factors
- Rationale
- Small lesion, intact head — some resolve spontaneously
- Modifier
- B–C
- Typical Approach
- Core decompression with or without bone grafting
- Rationale
- Head intact but large lesion — decompression reduces intraosseous pressure before collapse
- Modifier
- A
- Typical Approach
- Core decompression; consider vascularised fibular graft in young patients
- Rationale
- Sclerotic changes but no collapse; moderate lesion — surgery still has a window
- Modifier
- B–C
- Typical Approach
- Core decompression plus bone grafting or osteotomy; counsel that outcomes are guarded
- Rationale
- Large lesion approaching collapse — joint-preserving surgery is still possible but success rates fall
- Modifier
- Any
- Typical Approach
- Joint-preserving surgery in selected young patients (osteotomy, grafting); many proceed to arthroplasty
- Rationale
- Collapse has occurred — the hinge point. Young patients may still benefit from femoral head-preserving procedures, but most adults are heading toward replacement
- Column 5
- warning
- Modifier
- Any
- Typical Approach
- Total hip arthroplasty
- Rationale
- Established collapse or secondary arthritis — joint-preserving options have largely expired
- Column 5
- danger
- Modifier
- Any
- Typical Approach
- Total hip arthroplasty
- Rationale
- End-stage disease — the only realistic option
- Column 5
- danger
The distinction between Stage II (no collapse) and Stage III (subchondral collapse) is the single most important staging boundary in osteonecrosis. A patient with Stage II disease still has a realistic chance of joint-preserving surgery. Once the head collapses (Stage III), the probability of needing arthroplasty within two years rises steeply — some series report over 70 percent progression to arthroplasty even with intervention.
Pre-collapse: Preserve — Post-collapse: ReplaceTreatment by stage
Hook:Modifier C patients deteriorate faster within each pathway — urgency rises with lesion size.
The 2019 Revised ARCO Classification
The ARCO system in the comparison table above is the original 1993 version. An up-to-date examiner may ask about the 2019 revised ARCO classification, which was simplified for reproducibility and is now widely used in research:
- Findings
- Radiograph normal; MRI (or bone scan) positive — the only abnormality is on advanced imaging
- Findings
- Radiograph abnormal (sclerosis, osteolysis or focal osteoporosis) but NO subchondral fracture or flattening — still pre-collapse
- Findings
- Subchondral fracture / collapse: IIIA early (femoral-head depression 2 mm or less), IIIB late (depression greater than 2 mm)
- Findings
- Secondary osteoarthritis — joint-space narrowing, acetabular changes, head destruction
The key changes from 1993 were: Stage 0 was removed (a normal-imaging stage is unverifiable and clinically unused), each stage was tied to a clear radiograph/MRI step, and Stage III was subdivided by the degree of collapse using a 2 mm femoral-head-depression threshold that carries prognostic and surgical weight. The 2019 consensus deliberately kept the staging simple and recommended that lesion size and location be reported separately rather than embedded as sub-stages, because the older quantitative sub-classes had poor inter-observer reproducibility — the modern counterpoint to Steinberg's embedded A, B, C size modifiers.
Limitations and Modern Context
- MRI quantification is operator-dependent. Estimating the percentage of head involvement from two-dimensional slices has moderate inter-observer variability, particularly for irregular or multifocal lesions. Three-dimensional volumetric MRI measurements are more reproducible but not yet part of routine staging.
- The A, B, C thresholds (15 percent and 30 percent) are somewhat arbitrary. They were chosen to create three roughly equal prognostic groups, but the real relationship between lesion size and collapse risk is continuous — a lesion at 29 percent is not meaningfully different from one at 31 percent, yet they fall into different modifier groups.
- The system does not incorporate the lesion location. A small lateral lesion (poor prognosis) and a large medial lesion (better prognosis) may receive the same modifier. This is why some centres combine Steinberg with the JIC location-based typing for the most complete assessment.
- Stage 0 is almost never used clinically. It requires histological confirmation in a patient with normal imaging, which is rare outside research or contralateral hip biopsy during surgery for the other side. Do not expect to encounter it in practice.
- The post-collapse stages (IV–VI) are less useful than the pre-collapse stages. Once the head has collapsed, the classification refines how badly it is destroyed, but the treatment decision (arthroplasty) is largely the same. The real value of Steinberg lies in Stages 0–III, where it guides whether to operate, what to do, and how urgently.
- Bisphosphonates, extracorporeal shockwave therapy, and newer biological adjuncts may alter the natural history at any given stage. The classification does not account for treatment received when assigning prognosis.
Relationship to Ficat, ARCO, and Japanese Investigation Committee Systems
Multiple classification systems exist for osteonecrosis. The examiner may ask you to compare them. The key differences are whether MRI is incorporated, whether lesion size is quantified, and whether the post-collapse stages are subdivided.
- Ficat and Arlet (1980)
- 4 (I–IV)
- Steinberg (1995)
- 7 (0–VI)
- ARCO (1993)
- 4 (0–III with sub-stages)
- Japanese Investigation Committee (JIC)
- 4 (Type 1–4)
- Ficat and Arlet (1980)
- No — Stages I and II are radiograph-based only
- Steinberg (1995)
- Yes — stages refined by MRI findings
- ARCO (1993)
- Yes — Stage 0 and I defined on MRI
- Japanese Investigation Committee (JIC)
- Yes — lesion location mapped on MRI
- Ficat and Arlet (1980)
- No
- Steinberg (1995)
- Yes — A, B, C modifiers
- ARCO (1993)
- Yes — less than 30 percent, 30–60 percent, greater than 60 percent
- Japanese Investigation Committee (JIC)
- Yes — by lesion location (Type A, B, C1, C2)
- Ficat and Arlet (1980)
- Collapse appears at Stage III only
- Steinberg (1995)
- Stages III (crescent/early collapse), IV (flattened head), V (acetabular involvement) — more granular
- ARCO (1993)
- Stage III includes collapse
- Japanese Investigation Committee (JIC)
- Not explicitly staged — collapse inferred from radiographic changes
- Ficat and Arlet (1980)
- No — absorbed into Stage IV
- Steinberg (1995)
- Yes — Stage VI (advanced degenerative joint disease)
- ARCO (1993)
- No
- Japanese Investigation Committee (JIC)
- No
- Ficat and Arlet (1980)
- Quick bedside staging on radiographs
- Steinberg (1995)
- Comprehensive staging with MRI quantification and post-collapse detail
- ARCO (1993)
- International research consistency
- Japanese Investigation Committee (JIC)
- Lesion location-based prognosis (medial, central, lateral)
The JIC classification uses the location of the necrotic lesion on MRI rather than its percentage size. Type C2 (lateral lesion involving more than one-third of the lateral weight-bearing surface) has the worst prognosis, roughly equivalent to Steinberg modifier C. An examiner may ask you about the JIC system specifically — know that it focuses on where the dead bone is, not just how much of it there is. A lateral lesion is worse than a medial one of the same size because the lateral dome bears the most load.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 34-year-old man presents with a three-month history of deep left groin pain. He takes oral corticosteroids for inflammatory bowel disease. Radiographs are normal. MRI shows a focal area of low signal in the anterosuperior femoral head involving approximately 25 percent of the head on the mid-coronal slice, with a surrounding rim of high signal on T2. How do you stage this and what do you recommend?”
“A 46-year-old woman with sickle cell disease has bilateral hip pain. On the right, radiographs show a crescent sign with early flattening; MRI shows 18 percent head involvement. On the left, radiographs show sclerotic changes but the head is round; MRI shows 35 percent involvement. How do you stage each hip, what is the prognosis, and how would you manage her?”
The seven stages
- Stage 0: normal radiographs, normal MRI — histological diagnosis only
- Stage I: normal radiographs, abnormal MRI — no collapse
- Stage II: sclerotic/cystic radiographic changes, NO flattening or crescent — no collapse
- Stage III: crescent sign and/or subchondral fracture — COLLAPSE HAS OCCURRED
- Stage IV: flattened head, joint space preserved or minimally narrowed
- Stage V: flattened head WITH acetabular involvement
- Stage VI: advanced degenerative joint disease — destroyed joint
A, B, C modifiers (head involvement on MRI)
- A: less than 15 percent — best prognosis within any stage
- B: 15 to 30 percent — intermediate risk
- C: greater than 30 percent — highest collapse risk, the single most important negative prognostic factor
- Measure on mid-coronal T1-weighted images where the low-signal lesion is clearest
Pre-collapse versus post-collapse — the treatment hinge
- Pre-collapse (Stages 0–II): joint-preserving surgery — core decompression with or without bone grafting, osteotomy, vascularised fibular graft in young patients
- Post-collapse (Stage III onward): arthroplasty is the dominant pathway; joint-preserving options exist but with lower success rates
- Stage IIC (no collapse but greater than 30 percent involvement) has a worse prognosis than Stage IIIA (collapse but less than 15 percent involvement) — size matters
- Core decompression is for pre-collapse disease only — it does not reverse collapse
Comparing classification systems
- Ficat: four stages, no MRI quantification, no post-collapse subdivision — simplest but least granular
- Steinberg: seven stages plus A/B/C — most detailed for pre-collapse and early-collapse disease
- ARCO: four stages with sub-stages, incorporates MRI, used for international research consistency
- JIC: classifies by lesion location (medial, central, lateral) on MRI — lateral lesions carry the worst prognosis regardless of size
Key landmark studies
- Steinberg, Hayken, Steinberg (1995) — original seven-stage classification with A/B/C modifiers (JBJS Br)
- Steinberg and Steinberg (2004) — overview of all classification systems (Orthop Clin North Am)
- Mont et al. (2006) — systematic analysis comparing Ficat, ARCO, JIC, and Steinberg systems (JBJS Am)
- Choi, Steinberg, Cheng (2015) — diagnosis and classification systems review (Curr Rev Musculoskelet Med)
- Steinberg et al. (2018) — 3D volumetric versus 2D percentage MRI measurement of lesion size (Int Orthop)
Viva traps to avoid
- Giving the stage without the modifier — always report both (for example, Stage IIC)
- Calling a large pre-collapse lesion Stage III — Stage III requires structural collapse, not just a big lesion
- Recommending core decompression for a collapsed head (Stage III onward) — the bone has already failed
- Ignoring lesion location — a lateral lesion of any size is worse than a medial lesion of the same size