Stem Cells & Mesenchymal Stromal Cells (MSCs) in Orthopaedics
MSCs were thought to home to injury, engraft, and directly become large amounts of new bone or cartilage. In practice, long-term engraftment is limited.
MSCs act largely by paracrine and immunomodulatory signalling - secreting growth factors, cytokines and extracellular vesicles that recruit and activate host cells and dampen inflammation (hence the term "medicinal signalling cells").
MSC-79
Hook:MSC = adherent, CD73/90/105 positive, haematopoietic-marker negative, trilineage capable.
SIGNAL
Hook:MSCs SIGNAL more than they build - paracrine and immunomodulatory, not bulk engraftment.
Overview & Introduction
Regenerative medicine is a recurring basic-science viva theme, and "stem cells" is where candidates most often go wrong by overstating what the cells do. The disciplined way to hold this topic is three layers: the definitions (what a stem cell is, the potency hierarchy, and the precise ISCT criteria that make a cell an MSC), the mechanism (the modern paracrine/immunomodulatory model — "medicinal signalling cells" — rather than engraftment), and the honest clinical reality (minimally-manipulated BMAC versus tightly-regulated culture-expanded products, with heterogeneous, largely early-phase evidence). Get those three right and you can answer almost any examiner question — and avoid the trap of claiming MSCs regrow tissue by becoming it.
Concepts: The Stem-Cell Hierarchy
A stem cell has two defining properties: self-renewal (it can divide to make more of itself) and differentiation (it can become specialised cell types). Potency grades this capacity: totipotent (whole organism incl. placenta) → pluripotent (all three germ layers - embryonic stem cells, and induced pluripotent stem cells (iPSCs) reprogrammed from adult cells) → multipotent (restricted lineages, e.g. mesenchymal and haematopoietic stem cells) → unipotent (one lineage). Orthopaedic regenerative medicine works with adult multipotent MSCs, avoiding the ethical and tumorigenicity concerns of embryonic/pluripotent cells.
What Is an MSC? (ISCT Criteria)
Because "MSC" had been used loosely, the International Society for Cellular Therapy (ISCT) set minimal criteria for a multipotent mesenchymal stromal cell:
- Plastic adherence in standard culture.
- Surface marker profile - POSITIVE for CD73, CD90, CD105; and NEGATIVE for the haematopoietic/endothelial markers CD45, CD34, CD14 (or CD11b), CD79a (or CD19) and HLA-DR.
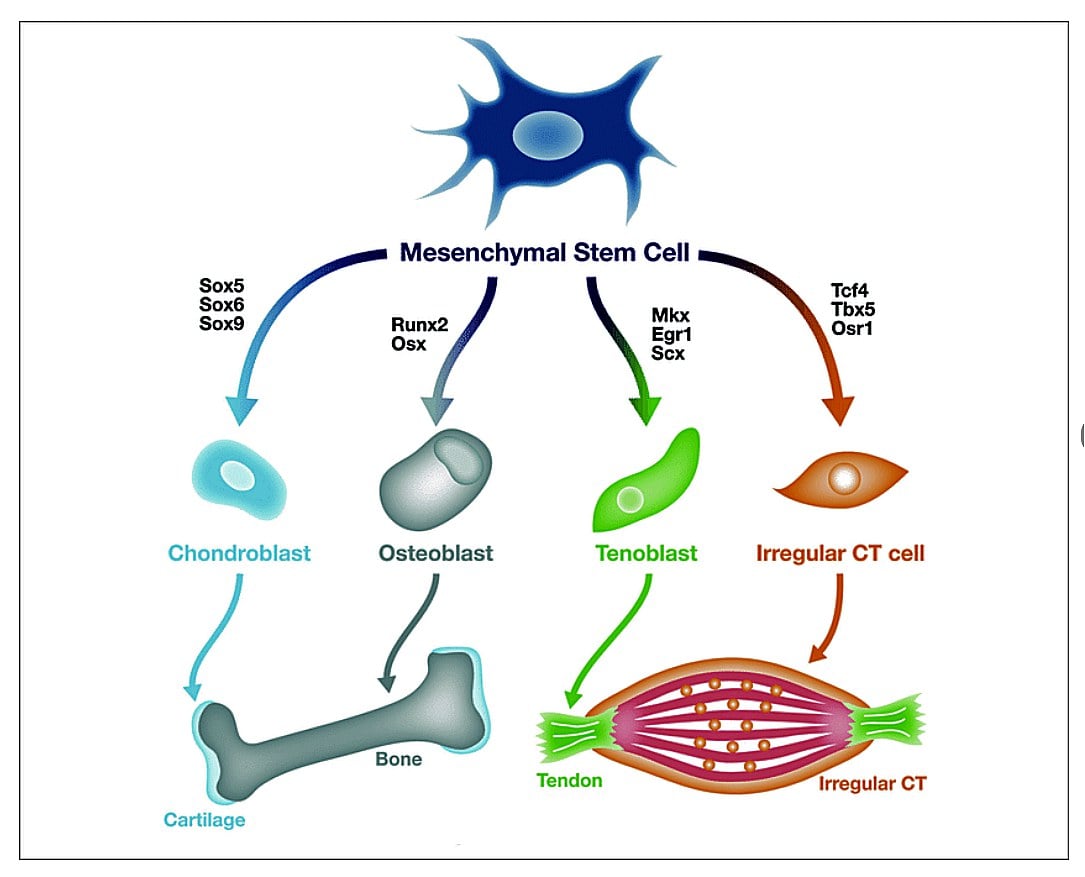
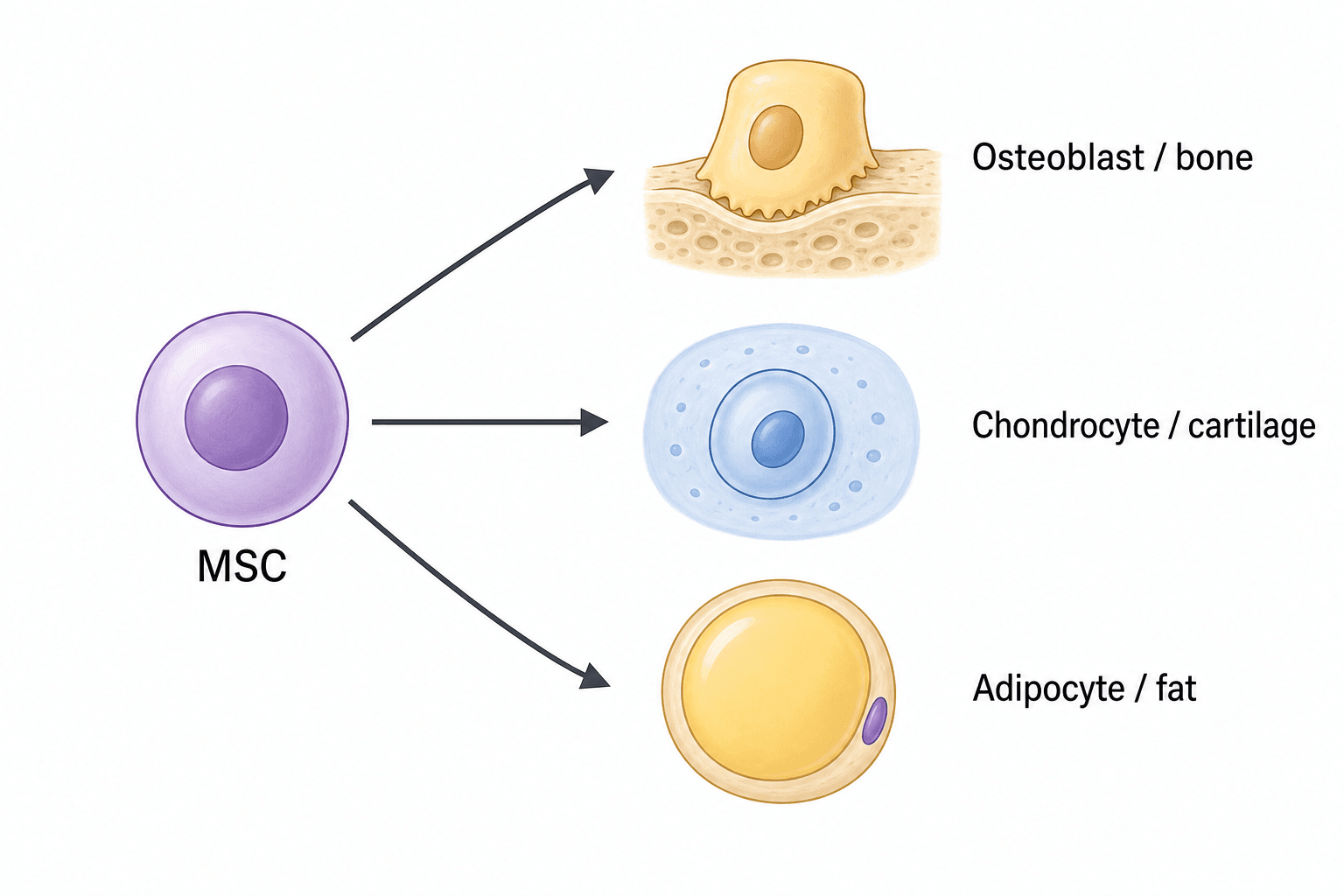
- Trilineage differentiation in vitro into osteoblasts, chondrocytes and adipocytes.
Sources & Mechanism of Action
- Bone marrow (BM-MSCs) - the classic source (iliac crest aspirate); well-characterised but MSCs are a small fraction of marrow cells.
- Adipose tissue (AD-MSCs) - abundant and easily harvested by lipoaspiration; high yield.
- Umbilical cord / Wharton's jelly and perinatal tissues - young, proliferative cells; a potential "off-the-shelf" allogeneic source, though differentiation is less consistent than BM-MSCs.
- Others: synovium, periosteum, dental pulp, muscle.
"A small fraction of marrow" is examinable as actual numbers and method:
- CFU-F assay (colony-forming unit-fibroblast): the standard functional quantification — marrow cells plated at low density, and each MSC forms a discrete adherent fibroblastic colony, so the colony count estimates MSC frequency and clonogenicity.
- MSCs are rare: roughly 1 in 10,000 to 100,000 marrow nucleated cells (about 0.001-0.01%), and their number and potency DECLINE with donor age and comorbidity — directly relevant because the typical BMAC/OA patient is older, so an autologous concentrate yields fewer, less potent cells.
- Harvest technique determines yield: aspirate small volumes (~2 mL per site) and reposition the needle to multiple sites on the iliac crest, because a large single-site aspiration dilutes the sample with peripheral blood and lowers the MSC concentration — the practical reason BMAC counts are so variable.
Clinical Applications & Caveats
- Form used
- BMAC, AD-MSCs (+/- scaffold)
- Evidence status
- Promising, mostly early-phase/heterogeneous
- Form used
- BMAC, adipose-derived
- Evidence status
- Symptomatic benefit in some trials; not standardised
- Form used
- BMAC, MSC + graft/scaffold
- Evidence status
- Adjunct; supportive but variable evidence
- Form used
- Core decompression + BMAC
- Evidence status
- Some benefit in early (pre-collapse) disease
- Form used
- MSC-based
- Evidence status
- Investigational

A crucial distinction is minimal manipulation versus culture expansion. Point-of-care BMAC (concentrated, same-procedure, minimally manipulated) is regulated more permissively, whereas culture-EXPANDED MSCs are classified as advanced-therapy medicinal products / cell-therapy products and are tightly regulated (e.g. by the FDA and EMA). The overall evidence is heterogeneous and largely early-phase, products and dosing are not standardised, and direct-to-consumer "stem-cell clinics" frequently make claims that outstrip the evidence (with safety concerns). The mature position is cautious, evidence-guided use with honest counselling about the investigational status of most indications.
For the nonunion/bone-defect application, examiners want MSCs placed within graft biology — the three properties of a bone graft:
- Osteogenesis — living cells (osteoblasts/MSCs) that directly form bone: this is precisely what MSCs/BMAC supply (autograft and marrow are osteogenic; allograft and synthetics are not).
- Osteoinduction — signals (notably BMPs, plus TGF-β/IGF) that recruit and drive host MSCs down the osteoblastic line.
- Osteoconduction — a passive scaffold (cancellous autograft, allograft, ceramics) for vascular and cellular ingrowth.
These map onto the Diamond Concept of fracture/nonunion healing — osteogenic cells + osteoconductive scaffold + osteoinductive growth factors + mechanical stability (+ adequate vascularity) — all of which must be present. MSCs/BMAC are the cellular (osteogenic) arm, which is why they are used as an adjunct combined with a graft/scaffold and stable fixation in nonunion, not as a stand-alone cure.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is a mesenchymal stromal cell, how is it defined, and how does it differ from a pluripotent stem cell?”
“A patient asks for a 'stem-cell injection' for knee osteoarthritis. How do MSCs actually work, what would you offer, and what caveats would you give?”
Hierarchy
- Toti- → pluri- (ESC/iPSC) → multi- (MSC, haematopoietic) → unipotent
- Stem cell = self-renewal + differentiation
- Orthopaedics uses adult multipotent MSCs
ISCT MSC definition
- Plastic adherence
- CD73+/CD90+/CD105+; CD45-/CD34-/CD14(11b)-/CD79a(19)-/HLA-DR-
- Trilineage: osteoblast, chondrocyte, adipocyte
Sources & mechanism
- Bone marrow (classic), adipose (abundant), umbilical cord/Wharton's jelly
- Mechanism mainly paracrine/immunomodulatory ('medicinal signalling cells')
- Limited long-term engraftment
Clinical & caveats
- BMAC/adipose for cartilage/OA/nonunion/early osteonecrosis (with core decompression)
- Minimally-manipulated (BMAC) vs culture-expanded (advanced-therapy, regulated)
- Evidence heterogeneous/early-phase; not standardised; beware unregulated clinics
Evidence & Key Studies
The two cited reviews are deliberately chosen to make two examiner points rather than to oversell efficacy. Klontzas shows that the source matters — umbilical-cord MSCs share the MSC phenotype but differentiate less consistently than bone-marrow MSCs, so "MSC" is not one standardised product. Li shows that the joint inflammatory microenvironment governs the result — in an inflamed milieu MSCs differentiate aberrantly and chondrocytes dedifferentiate to fibroblast-like cells, yielding mechanically poor fibrocartilage — which is exactly why the modern model is immunomodulatory rather than structural. The honest synthesis (consistent across the wider literature): the basic science is solid, but clinical efficacy data are heterogeneous and largely early-phase, with no standardised product — quote MSC therapy as promising but investigational for most orthopaedic indications.
Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement
- ISCT position statement establishing the three minimal criteria that define a human MSC
- (1) plastic adherence in standard culture; (2) CD105/CD73/CD90 positive and CD45/CD34/CD14 or CD11b/CD79a or CD19/HLA-DR negative; (3) trilineage differentiation to osteoblasts, adipocytes and chondroblasts
- Created to standardise characterisation so that studies using different isolation/expansion methods could be compared
Bone and cartilage regeneration with the use of umbilical cord mesenchymal stem cells
- MSCs can be isolated from umbilical cord (Wharton's jelly, perivascular tissue, blood) and share phenotypic features with bone-marrow-derived MSCs.
- Their osteogenic and chondrogenic differentiation is less consistent than that of bone-marrow MSCs across studies.
- Further work with scaffolds, growth factors and culture technology is needed before they can replace BM-MSCs clinically - illustrating that source matters and standardisation is lacking.
The immune microenvironment in cartilage injury and repair
- The inflammatory microenvironment after cartilage injury drives chondrocyte death/hypertrophy and matrix breakdown, and progression to osteoarthritis.
- In an inflammatory milieu MSCs undergo aberrant differentiation and chondrocytes dedifferentiate to fibroblast-like cells, yielding mechanically poor fibrocartilage.
- Successful cartilage regeneration requires managing the joint inflammatory/immune microenvironment - underscoring the immunomodulatory rather than purely structural role of cell therapy.