Acral Lentiginous Melanoma of the Nail Unit | Hutchinson Sign | ABCDEF Criteria
- Subungual melanoma is an acral lentiginous melanoma arising from the nail matrix melanocytes
- Hutchinson sign (pigmentation extending onto the proximal nail fold) is pathognomonic but not always present
- ABCDEF criteria for nail melanoma: Age, Band, Change, Digit, Extension, Family history
- Average diagnostic delay is 6-12 months due to confusion with subungual haematoma or fungal infection
- Nail-bed biopsy of the matrix is essential for diagnosis — never assume pigmentation is benign without histology
- “Hutchinson sign = pigmentation on proximal or lateral nail fold (highly suggestive of melanoma)
- “ABCDEF of nail melanoma: Age 50-70, Brown-Black Band, Change, Digit (thumb/great toe), Extension onto fold, Family history
- “Subungual haematoma grows out with the nail; melanoma does NOT migrate distally
- “Biopsy the nail MATRIX (not just the bed) — that is where melanoma arises
Pigmentation extending onto the proximal or lateral nail fold. This is the single most important clinical sign of subungual melanoma. It represents radial growth phase spreading beyond the nail matrix onto the periungual skin. If you see this, biopsy is mandatory.
Average diagnostic delay is 6-12 months. Subungual melanoma is frequently mistaken for subungual haematoma, onychomycosis, or benign melanonychia. Any pigmented nail band that is new, widening, or darkening in a fair-skinned adult must be biopsied.
Biopsy the nail MATRIX, not the nail bed. Subungual melanoma arises from melanocytes in the nail matrix. A punch or excisional biopsy of the matrix (exposed by reflecting the proximal nail fold) is required for definitive diagnosis.
In situ = wide matrix excision. Invasive = amputation at appropriate level. Sentinel lymph node biopsy is recommended for invasive melanoma with Breslow thickness greater than 1 mm. Do not attempt conservative excision for invasive disease.
- Diagnosis
- Hutchinson sign present, matrix biopsy
- Treatment
- If in situ: wide matrix excision. If invasive: amputation
- Key Pearl
- Biopsy early — delay worsens prognosis
- Diagnosis
- Subungual haematoma vs melanoma distinction critical
- Treatment
- If haematoma: observation. If uncertain: biopsy
- Key Pearl
- Haematoma grows out with nail; melanoma does not
- Diagnosis
- Likely thick invasive melanoma, biopsy confirms
- Treatment
- Amputation + sentinel lymph node biopsy
- Key Pearl
- Advanced at presentation, poor prognosis
ABCDEFABCDEF Criteria for Nail Melanoma
Hook:Use ABCDEF for every pigmented nail band — miss one letter and you may miss the melanoma!
GROWTHSubungual Haematoma vs Melanoma
Hook:Watch for GROWTH patterns — haematoma moves, melanoma stays and spreads!
MATRIXNail Matrix Biopsy Approach
Hook:Follow the MATRIX steps to biopsy the nail matrix, not the bed — that is where the melanoma lives!
Overview and Epidemiology
Subungual melanoma is a rare but aggressive variant of acral lentiginous melanoma that arises in the nail matrix. It is the most common type of melanoma in patients with darker skin tones (Fitzpatrick V-VI), where it accounts for a disproportionate share of melanoma diagnoses. The average diagnostic delay of 6-12 months means patients frequently present with thick, advanced lesions and consequently poorer prognosis compared with other cutaneous melanomas. A high index of suspicion and early biopsy are the most important tools for improving outcomes.
- Incidence: 0.7 to 3.5 percent of all cutaneous melanomas
- Age: Peak 50-70 years, but can occur at any age
- Sex: Slight male predominance in most series
- Race: Disproportionately affects darker-skinned individuals (most common melanoma subtype in Asian and Black populations)
- Site: Thumb (25-40 percent) and great toe (25-30 percent) most common
- Late presentation: Median Breslow thickness at diagnosis is 2.5-4.0 mm (thick)
- Diagnostic delay: Average 6-12 months from first symptom to diagnosis
- Misdiagnosis rate: 25-30 percent initially diagnosed as haematoma, fungal infection, or benign naevus
- Prognosis: 5-year survival 40-80 percent depending on stage at diagnosis
- Functional loss: Treatment often requires amputation of the affected digit
Pathophysiology
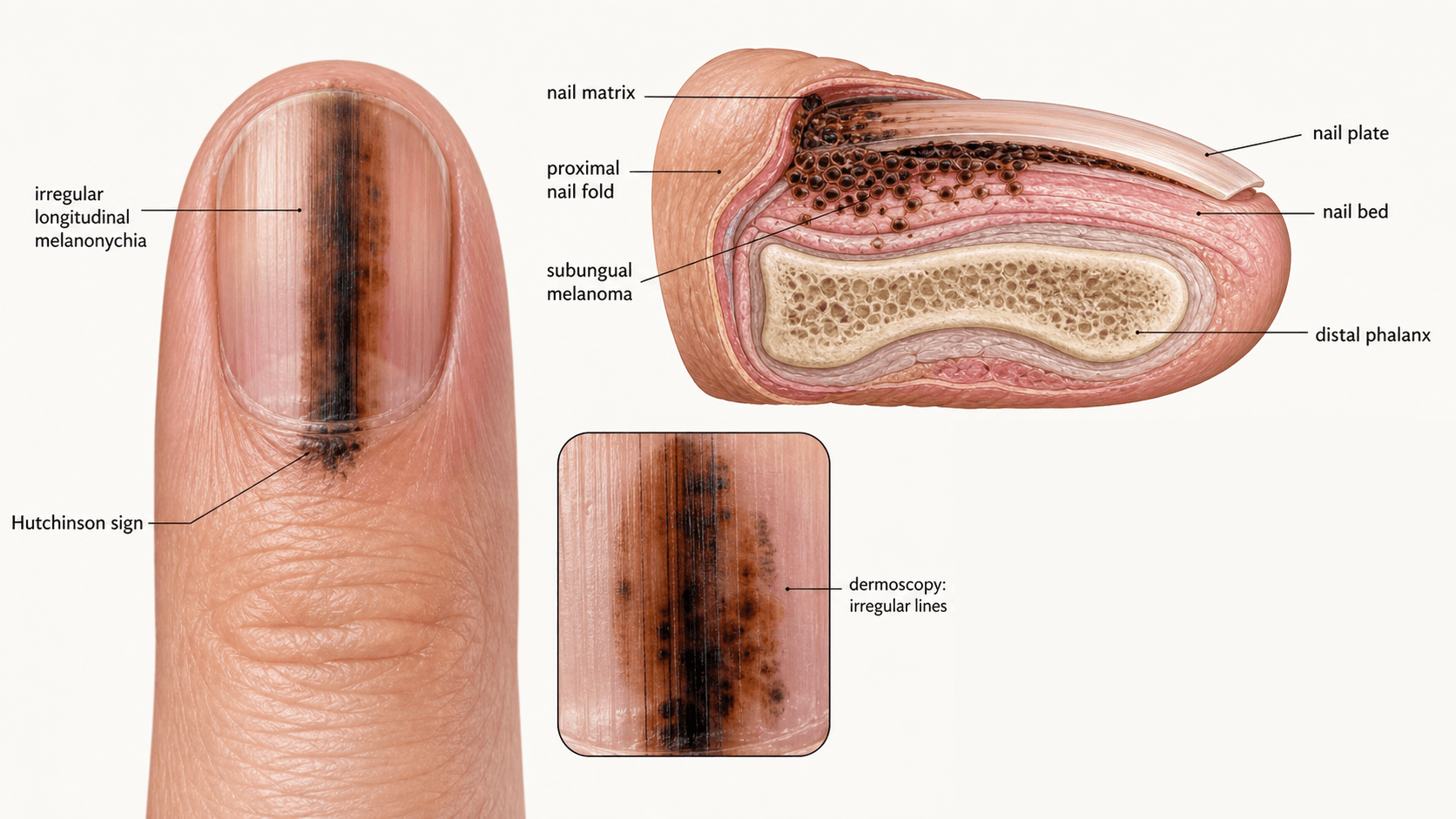
The nail unit comprises the nail matrix (germinal and sterile matrix), nail bed, nail plate, proximal nail fold, and lateral nail folds. The germinal matrix (proximal portion beneath the proximal nail fold) produces the nail plate and contains the melanocytes from which subungual melanoma arises. Melanocytes in the matrix transfer melanin to onychocytes (nail plate cells), producing a longitudinal pigmented band (melanonychia) when activated or neoplastic. Importantly, the nail matrix has no granular layer, and melanocytes are distributed singly among basal keratinocytes at a ratio of approximately 1:5 to 1:10 — similar to epidermal melanocytes elsewhere but with distinct patterns of pigmentation.
- Growth Pattern
- Radial growth along basal layer, then vertical
- Clinical Appearance
- Slowly widening pigmented band with Hutchinson sign
- Prognosis
- Variable — depends on Breslow at diagnosis
- Growth Pattern
- Rapid vertical growth phase with minimal radial
- Clinical Appearance
- Nodule, ulceration, rapid nail destruction
- Prognosis
- Poor — often thick at presentation
- Growth Pattern
- Spindle cells with dense stromal fibrosis
- Clinical Appearance
- May be amelanotic (non-pigmented), firm mass
- Prognosis
- Higher local recurrence, lower nodal metastasis
- Growth Pattern
- Confined to matrix epithelium, no invasion
- Clinical Appearance
- Pigmented band only, no mass or ulceration
- Prognosis
- Excellent with complete excision
Key mutations: KIT mutations and amplifications are more common in acral lentiginous melanomas (including subungual) than in other melanoma subtypes. BRAF V600E mutations are less frequent (15-20 percent) compared with non-acral cutaneous melanomas (40-50 percent). NRAS mutations are also uncommon. This molecular profile has therapeutic implications — KIT inhibitors (imatinib) may be considered for metastatic disease with KIT mutations.
Benign mimics: Subungual haematoma, onychomycosis, benign melanonychia, ethnic melanonychia, and subungual foreign body all mimic early melanoma
Low suspicion: Both patients and clinicians may attribute dark nail changes to trauma or fungal infection, especially in younger patients
Anatomical concealment: The nail plate obscures the underlying matrix lesion, making clinical assessment difficult
Access to biopsy: Nail matrix biopsy requires specific technique and referral to a specialist
Classification and Staging
AJCC 8th Edition Staging for Subungual Melanoma
Subungual melanoma is staged according to the AJCC melanoma staging system (8th edition), which applies the same T (tumour thickness), N (nodal), and M (metastasis) criteria as cutaneous melanoma elsewhere. Breslow thickness is the primary T-category determinant.
- Breslow Thickness
- No invasive component
- Ulceration
- N/A
- 5-Year Survival (approximate)
- Near 100 percent with complete excision
- Breslow Thickness
- Less than 0.8 mm (T1a) or 0.8-1.0 mm (T1b)
- Ulceration
- T1b = ulcerated or mitoses present
- 5-Year Survival (approximate)
- 85-95 percent
- Breslow Thickness
- 1.01-2.0 mm
- Ulceration
- T2a without ulceration, T2b with ulceration
- 5-Year Survival (approximate)
- 70-85 percent
- Breslow Thickness
- 2.01-4.0 mm
- Ulceration
- T3a without ulceration, T3b with ulceration
- 5-Year Survival (approximate)
- 50-70 percent
- Breslow Thickness
- Greater than 4.0 mm
- Ulceration
- T4a without ulceration, T4b with ulceration
- 5-Year Survival (approximate)
- 30-50 percent
Note: Most subungual melanomas present as T3 or T4 due to diagnostic delay.
Clinical Assessment
- Duration: When was the pigmented band first noticed? How rapidly has it changed?
- Trauma: Was there a preceding injury? (Does not exclude melanoma)
- Change: Has the band widened, darkened, or extended onto the skin?
- Symptoms: Pain, bleeding, nail splitting, or nail loss
- Systemic: Weight loss, lymphadenopathy, other skin lesions
- Family history: Melanoma, dysplastic naevus syndrome
- Inspect: All 20 nails — is this single or multiple digit involvement?
- Band characteristics: Width, colour (uniform or variegated), borders
- Hutchinson sign: Pigmentation on proximal or lateral nail fold
- Nail plate: Distortion, splitting, crumbling, or destruction
- Digit: Swelling, mass, ulceration, or bleeding
- Regional nodes: Epitrochlear, axillary (upper limb) or inguinal (lower limb)
Hutchinson sign refers to the extension of brown-black pigmentation from the nail matrix onto the proximal or lateral nail fold skin. It represents the radial growth phase of melanoma spreading beyond the confines of the nail unit onto the periungual epidermis.
Micro-Hutchinson sign (visible only with dermoscopy) may be an earlier indicator.
Important caveat: Hutchinson sign is not 100 percent sensitive — early melanomas confined to the matrix may not show periungual extension. Its absence does not exclude melanoma.
Conversely: Pseudo-Hutchinson sign can occur in benign conditions (Laugier-Hunziker syndrome, racial pigmentation). Biopsy is the definitive discriminator.
- Melanoma
- Greater than 3 mm, widening over time
- Benign Melanonychia
- Less than 3 mm, stable
- Melanoma
- Variegated (light and dark brown to black)
- Benign Melanonychia
- Uniform brown, homogeneous
- Melanoma
- Blurred, irregular
- Benign Melanonychia
- Sharp, well-defined
- Melanoma
- Present on dermoscopy
- Benign Melanonychia
- Absent
- Melanoma
- Absent (unless ulcerated)
- Benign Melanonychia
- May be present (haematoma)
- Melanoma
- May be present (advanced)
- Benign Melanonychia
- Usually intact
Dermoscopy (onychoscopy) of the nail is a valuable adjunct but never replaces biopsy. The most suspicious dermoscopic features for melanoma are: irregular pigmented bands of varying colour and width, micro-Hutchinson sign, and disruption of the nail plate. If dermoscopy is equivocal, proceed to biopsy regardless.
Up to about a quarter of subungual melanomas are amelanotic (little or no visible pigment), and this is the most dangerous diagnostic trap because the entire pigment-based framework - Hutchinson sign, ABCDEF bands, dermoscopy of melanonychia - simply fails.
The amelanotic lesion presents instead as a chronic, non-healing process: a friable nodule or granulation-tissue-like mass, a persistent ulcer, longitudinal nail dystrophy or splitting, or recurrent "paronychia" or "ingrowing nail" that does not settle. It is classically mistaken for a pyogenic granuloma, chronic paronychia, wart, onychomycosis, or a non-healing wound after nail surgery.
The rule: any solitary nail-unit lesion - pigmented or not - that fails to heal, recurs, bleeds, or is atypical in an adult must be biopsied (matrix and bed) with histology and immunohistochemistry (S-100, SOX10, Melan-A). Amelanotic melanoma will be missed if you only look for a dark band.
The adult rule of "biopsy any new, single, widening pigmented band" should not be applied unmodified to children. In childhood, longitudinal melanonychia is usually benign - most are nail matrix naevi or melanocytic activation/lentigines - and subungual melanoma is exceptionally rare before puberty.
Paediatric matrix naevi commonly show features that would mandate biopsy in an adult - a broad, variegated band, a pseudo-Hutchinson sign, even rapid change with growth - yet are benign. Management therefore leans toward careful clinical and dermoscopic monitoring with serial photography rather than reflexive biopsy, reserving matrix biopsy for genuinely atypical, rapidly destructive lesions, and weighing the real morbidity of biopsy (permanent nail dystrophy) against a very low melanoma risk.
The flip side - and the exam point - is that in an adult those same features demand biopsy. Knowing this age-dependent difference is a classic discriminator.
Investigations
Diagnostic Pathway
Assess: All 20 nails, Hutchinson sign, regional lymph nodes
Dermoscopy: Evaluate band width, colour uniformity, borders, micro-Hutchinson sign
Clinical photography: Document current appearance for serial comparison
Decision: If any concerning features, proceed to biopsy without delay
Technique: Reflect proximal nail fold, remove overlying nail plate to expose matrix, punch biopsy (3 mm) or excisional biopsy of the pigmented area
Essential: Biopsy must include the nail MATRIX — the origin of the melanoma
Histopathology: Request dermatopathology review with immunohistochemistry (S-100, HMB-45, Melan-A, SOX10, Ki-67)
Breslow thickness: Must be measured from the granular layer (or matrix equivalent) to deepest point of invasion
Sentinel lymph node biopsy: Indicated for Breslow greater than 1 mm (as per AJCC guidelines for cutaneous melanoma)
MRI of digit: May assess depth of soft tissue and bone involvement in thick tumours
CT chest/abdomen/pelvis or PET-CT: For staging of thick melanomas (greater than 4 mm Breslow) or if nodal disease confirmed
Baseline LDH: Prognostic marker in metastatic disease
The nail matrix biopsy is technically demanding. Key points: use a digital tourniquet for a bloodless field, reflect the proximal nail fold via lateral incisions, remove the overlying nail plate to visualize the matrix directly, and take a 3 mm punch or elliptical excision of the pigmented area. The specimen must include the full thickness of the matrix epithelium and underlying dermis. Send for dermatopathology with clinical context.
Management Algorithm
Melanoma In Situ of the Nail Matrix
Goal: Complete excision with clear margins while preserving digit function
Treatment Protocol
Histology: Confirm in situ disease with no invasive component
Margins: Clinical assessment of the extent of pigmentation (dermoscopy-assisted)
Consent: Risk of recurrence, nail deformity, need for wider excision if pathology upgrades
Approach: Reflect proximal nail fold, excise the involved area of the nail matrix with 5-10 mm margins
Reconstruction: Primary closure if possible; split-thickness skin graft or local flap if defect is large
Nail loss: Expected if the entire germinal matrix is excised — counsel patient pre-operatively
Monitoring: Regular clinical review every 3-6 months for at least 5 years
Recurrence: If margins were close or positive, re-excision is mandatory
Skin check: Full-body skin examination at each visit (risk of second primary melanoma)
In situ disease has an excellent prognosis with complete excision. However, achieving clear margins in the nail unit can be challenging due to anatomical constraints.
Complications
- Incidence
- 10-20 percent after conservative excision
- Risk Factors
- Positive margins, in situ disease at margins
- Management
- Re-excision or amputation if not already performed
- Incidence
- 20-40 percent in tumours greater than 2 mm Breslow
- Risk Factors
- Thick tumours, ulceration, high mitotic rate
- Management
- SLNB + completion lymphadenectomy or adjuvant therapy
- Incidence
- 15-30 percent in Stage III disease
- Risk Factors
- Thick primary, positive nodes, high mitotic rate
- Management
- Systemic immunotherapy or targeted therapy
- Incidence
- Universal — depends on digit and level
- Risk Factors
- Amputation level, dominant hand involvement
- Management
- Rehabilitation, prosthetics, occupational therapy
- Incidence
- Near 100 percent after matrix excision
- Risk Factors
- Extent of matrix resected
- Management
- Counsel pre-operatively; cosmetic prosthetic nail
The single most important prognostic factor is Breslow thickness at diagnosis — which directly reflects the duration of diagnostic delay. Subungual melanomas are frequently thick at presentation (median Breslow 2.5-4.0 mm) because early lesions are hidden under the nail plate and often attributed to benign causes. The key to improving outcomes is early biopsy of any suspicious nail pigmentation. There is no role for observation of a new, widening, or darkening pigmented nail band in an adult.
Outcomes and Prognosis
- Breslow
- No invasion
- 5-Year Survival
- Near 100 percent
- Key Prognostic Feature
- Complete excision is curative
- Breslow
- Less than 2.0 mm, no ulceration
- 5-Year Survival
- 80-95 percent
- Key Prognostic Feature
- Thin tumours do well with adequate surgery
- Breslow
- Greater than 1 mm with ulceration or greater than 2 mm
- 5-Year Survival
- 50-80 percent
- Key Prognostic Feature
- Thick tumours carry worse prognosis
- Breslow
- Any Breslow with nodal metastasis
- 5-Year Survival
- 40-70 percent (depends on nodal burden)
- Key Prognostic Feature
- Number of positive nodes is the key determinant
- Breslow
- Any Breslow with distant spread
- 5-Year Survival
- 15-30 percent (improving with immunotherapy)
- Key Prognostic Feature
- LDH level, sites of metastasis, treatment response
Best prognosis: In situ or thin melanoma (less than 1 mm Breslow) with clear margins, no ulceration, negative sentinel node
Poor prognosis: Thick melanoma (greater than 4 mm Breslow), ulceration, high mitotic rate, sentinel node positive, elevated LDH
Key message: The most important prognostic factor is early diagnosis. Any pigmented nail band in an adult that is new, single-digit, widening, or associated with Hutchinson sign warrants immediate biopsy. The exam question trap is always the patient with a "dark nail attributed to trauma" that turns out to be melanoma.
Guidelines, Registries & Global Practice
- Subungual melanoma accounts for 0.7-3.5 percent of all cutaneous melanomas worldwide
- Most common melanoma subtype in darker-skinned populations (Asian, African, Hispanic)
- Thumb and great toe are the most commonly affected sites across all populations
- Diagnostic delay is a universal problem, averaging 6-12 months globally
- High-resource: Dermoscopy, specialist nail matrix biopsy, sentinel node biopsy, immunotherapy for adjuvant and metastatic treatment
- Limited-resource: Clinical diagnosis supplemented by punch biopsy, standard amputation, limited access to SLNB and immunotherapy
- Universal principle: Outcome depends on early biopsy and adequate surgical margins more than on technology
- Education gap: Raising awareness among primary care physicians about Hutchinson sign and the need for biopsy is the most impactful intervention worldwide
- Diagnosis Emphasis
- Biopsy any suspicious nail pigmentation; dermoscopy adjunctive
- Surgical Treatment
- Amputation for invasive disease; margin guidelines per Breslow thickness
- Adjuvant Therapy
- Immune checkpoint inhibitors or BRAF/MEK inhibitors for Stage III-IV
- Diagnosis Emphasis
- Urgent referral for any new nail band with Hutchinson sign
- Surgical Treatment
- Excision or amputation based on Breslow; SLNB for greater than 1 mm
- Adjuvant Therapy
- NICE-approved immunotherapy regimens for adjuvant and metastatic use
- Diagnosis Emphasis
- Early biopsy emphasised; avoid prolonged antifungal trial without response
- Surgical Treatment
- Amputation standard for invasive; functional surgery for in situ
- Adjuvant Therapy
- Adjuvant immunotherapy or targeted therapy per molecular profile
- Diagnosis Emphasis
- High awareness due to acral lentiginous predominance in Asian populations
- Surgical Treatment
- Amputation with level determined by tumour extent; SLNB increasingly adopted
- Adjuvant Therapy
- KIT testing recommended; imatinib for KIT-mutated metastatic disease
There is no dedicated registry for subungual melanoma specifically. Melanoma registries (national cancer registries, AJCC melanoma database) include subungual cases but do not separate them for analysis in most instances. The evidence base consists predominantly of retrospective case series and literature reviews, with no randomized controlled trials specific to subungual melanoma management. Treatment recommendations are therefore extrapolated from general melanoma guidelines (NCCN, ESMO, BAD) with anatomical modifications for the nail unit.
Record in every patient with pigmented nail lesion:
- Presence or absence of Hutchinson sign
- Number of digits affected, band width, colour characteristics
- Duration of pigmentation and any documented change
- Dermoscopy findings if available
- Biopsy performed — site (matrix vs bed), technique, and histopathology result
- If biopsy not performed, documented reason and plan for follow-up with timeline
A missed or delayed diagnosis of subungual melanoma is a recurring source of medicolegal claims worldwide. Any pigmented nail lesion in an adult that is new, single-digit, widening, or associated with Hutchinson sign must be biopsied — never observe without histological exclusion.
Controversies & Areas of Uncertainty
For thin invasive melanomas (less than 2 mm Breslow), some centres advocate wide local excision of the nail unit rather than amputation, citing comparable local control rates. However, evidence is limited to small retrospective series, and amputation remains the standard of care in most guidelines for any invasive subungual melanoma.
The optimal level of amputation is debated. Some advocate amputation one joint proximal to the tumour, while others argue for the minimum level achieving clear margins. There is no Level I evidence comparing functional outcomes and oncological control between different amputation levels.
Sentinel lymph node biopsy is recommended for invasive melanomas greater than 1 mm Breslow, extrapolated from cutaneous melanoma guidelines. However, specific data on SLNB outcomes in subungual melanoma are limited. Lymphatic drainage from the nail unit may be variable, and false-negative rates have not been specifically studied.
Immunotherapy and targeted therapy indications are extrapolated from general melanoma trials (which include few subungual cases). Whether the distinct molecular profile of acral melanomas (more KIT, less BRAF) translates to different treatment responses is an area of active research.
MCQ Practice Points
Q: What is Hutchinson sign and what does it indicate? A: Pigmentation extending onto the proximal or lateral nail fold. It indicates radial growth of melanoma beyond the nail matrix onto the periungual skin. It is the most clinically important sign of subungual melanoma, though its absence does not exclude early disease.
Q: Where should a biopsy be taken from to diagnose subungual melanoma? A: The nail matrix (germinal matrix), not the nail bed. Subungual melanoma arises from melanocytes in the nail matrix. The biopsy technique involves reflecting the proximal nail fold, removing the overlying nail plate, and taking a punch or elliptical biopsy of the pigmented area of the matrix.
Q: How do you distinguish subungual haematoma from subungual melanoma? A: Haematoma migrates distally with nail growth; melanoma does not. Haematoma follows identifiable trauma, has uniform colour, and resolves over 2-3 months as the nail grows out. Melanoma is a progressive, widening, darkening band without a clear trauma history. Hutchinson sign is present only in melanoma. If in doubt, biopsy.
Q: What is the standard surgical treatment for invasive subungual melanoma with Breslow greater than 2 mm? A: Amputation of the affected digit at an appropriate level for clear margins, combined with sentinel lymph node biopsy. The amputation level is determined by the extent of the tumour — typically at the interphalangeal or metacarpophalangeal/metatarsophalangeal joint. Conservative excision is not recommended for thick invasive melanomas due to high local recurrence rates.
Q: What molecular mutations are more common in acral lentiginous melanoma (including subungual) compared with other cutaneous melanomas? A: KIT mutations and amplifications are significantly more common in acral lentiginous melanomas, while BRAF V600E mutations are less frequent (15-20 percent vs 40-50 percent in non-acral cutaneous melanomas). This has therapeutic implications — KIT inhibitors (imatinib) may be effective in metastatic disease with KIT mutations.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman presents with a 4-month history of a gradually widening dark brown band on her right thumbnail. She initially attributed it to trauma from gardening but it has continued to widen and darken. On examination, there is a 5 mm wide pigmented band extending the full length of the nail plate, with faint brown pigmentation visible on the proximal nail fold. No palpable lymphadenopathy. What is your diagnosis and management?”
“A 65-year-old man presents with a 12-month history of progressive dark discolouration and destruction of his left great toe nail. He was treated with oral antifungal medication by his general practitioner for 8 months with no improvement. On examination, the nail plate is completely destroyed with a darkly pigmented, ulcerated nodular lesion replacing the nail bed and matrix, extending 5 mm onto the dorsal skin of the toe. There is a 2 cm firm, palpable lymph node in the left inguinal region. Biopsy confirms acral lentiginous melanoma, Breslow 6.5 mm, ulcerated, mitotic rate 8 per mm squared. What is your staging and management plan?”
Key Clinical Features
- Acral lentiginous melanoma arising from nail matrix melanocytes
- Most common melanoma in darker-skinned populations (Fitzpatrick V-VI)
- Thumb and great toe are the most common sites
- Average diagnostic delay of 6-12 months due to misdiagnosis as haematoma or fungal infection
Diagnosis
- Hutchinson sign = pigmentation on proximal or lateral nail fold (pathognomonic but not always present)
- ABCDEF criteria: Age, Band (greater than 3 mm, widening), Change, Digit (thumb/great toe), Extension, Family
- Subungual haematoma grows out with nail; melanoma does NOT migrate distally
- Biopsy the nail MATRIX (not bed) — 3 mm punch or elliptical under tourniquet with fold reflected
Treatment Algorithm
- In situ: wide excision of the involved matrix with 5-10 mm margins
- Invasive less than 2 mm: wide excision or amputation; SLNB for greater than 1 mm
- Invasive greater than 2 mm: amputation at appropriate level + SLNB
- Node-positive: therapeutic lymph node dissection + adjuvant immunotherapy
Staging and Prognosis
- AJCC 8th edition staging (same as cutaneous melanoma elsewhere)
- Breslow thickness is the most important prognostic factor
- Most present thick (median 2.5-4.0 mm) — hence prognosis is worse than other cutaneous melanomas
- 5-year survival: in situ near 100 percent, Stage II 50-80 percent, Stage IV 15-30 percent
Molecular and Therapeutic Points
- KIT mutations more common; BRAF V600E less common (15-20 percent) than in non-acral melanoma
- KIT testing is essential — opens targeted therapy with imatinib for metastatic disease
- Adjuvant immunotherapy (nivolumab, pembrolizumab) for Stage III disease
- Multidisciplinary management: surgical oncology, medical oncology, dermatopathology
Evidence Base and Key Trials
'Functional' surgery in subungual melanoma
- Retrospective comparison of wide local excision versus amputation for subungual melanoma
- No significant difference in local recurrence or survival between wide excision and amputation for thin melanomas
- Amputation remains the standard for thick (greater than 2 mm) invasive subungual melanoma
- Sentinel lymph node biopsy should be considered for invasive disease greater than 1 mm Breslow
Distinct sets of genetic alterations in melanoma
- Acral melanomas (including subungual) and mucosal melanomas have low BRAF/NRAS mutation rates but frequent KIT mutations and copy number gains
- BRAF and NRAS mutations are uncommon in acral lentiginous melanomas compared with non-acral cutaneous melanomas
- KIT mutations and amplifications are significantly more common in acral lentiginous melanomas
- Copy number variations (amplifications of CCND1, CDK4) are more prevalent than point mutations in acral melanomas
Nail matrix melanoma in situ: conservative surgical management
- Conservative surgical excision of nail matrix melanoma in situ can achieve local control while preserving the digit
- Total or partial nail matrix excision with appropriate reconstruction is the cornerstone of in situ management
- Wide local excision of the matrix with clear margins is curative for in situ disease
- Biopsy location must target the most proximal pigmented area of the matrix for accurate histological diagnosis
Imatinib for melanomas harboring mutationally activated or amplified KIT arising on mucosal, acral, and chronically sun-damaged skin
- Multicentre phase II trial of imatinib in KIT-mutated or KIT-amplified metastatic melanoma, including acral lentiginous subtype
- Overall response rate of approximately 20-30 percent with durable responses in KIT-positive metastatic melanoma
- Acral lentiginous melanomas (which include subungual) were specifically represented in the KIT-positive cohort
- Established imatinib as a viable targeted-therapy option for KIT-driven metastatic acral melanoma
Malignant melanoma in the hand: current evidence and recommendations
- Comprehensive current-evidence review of melanoma presenting in the hand, including subungual and acral lentiginous variants
- Subungual melanoma continues to present with diagnostic delay and at advanced Breslow thickness, with poorer outcomes than non-acral cutaneous melanoma
- Nail matrix biopsy and sentinel lymph node biopsy for greater than 1 mm Breslow remain the diagnostic and staging standards
- Amputation is indicated for invasive subungual disease; functional surgery is reserved for in situ or selected thin lesions