Benign & Malignant - An Overview
- The cardinal principle is that a foot or ankle mass is MALIGNANT UNTIL PROVEN OTHERWISE: malignant tumours here are rare and are frequently MISDIAGNOSED as benign (a 'ganglion', wart or callus), which leads to inadequate, unplanned excision and poor outcomes - so any soft-tissue mass that is solid, enlarging, deep to fascia, fixed, painful or recurrent must be properly worked up before any surgery. Note that SIZE IS NOT A SAFE FILTER HERE: the confined compartments of the foot make a sarcoma symptomatic while it is still small, and in the cited synovial sarcoma series tumour size was NOT a prognostic variable - so a small mass is not a reassured mass.
- Most foot lumps ARE benign - ganglion (the commonest), plantar fibroma (Ledderhose disease), giant-cell tumour of the tendon sheath, synovial chondromatosis, lipoma and nerve sheath tumours - but the benign label must be earned by appropriate assessment, not assumed from the location or a soft history.
- The commonest soft-tissue SARCOMA of the foot is SYNOVIAL SARCOMA; it can be small and relatively slow-growing, sits near joints/tendons, may calcify, and is a classic lesion to be mistaken for a ganglion and excised unplanned - the commonest primary bony malignancy of the foot is OSTEOSARCOMA, with Ewing sarcoma and chondrosarcoma also occurring.
- The correct PATHWAY is IMAGE then BIOPSY then REFER, all BEFORE definitive excision: plain radiographs for the bone, MRI for the soft tissue and local extent, staging where malignancy is suspected, and a properly PLANNED biopsy (placed so the tract can be excised en bloc with the tumour, ideally performed at or in discussion with the unit that will do the definitive surgery).
- An UNPLANNED ('whoops') EXCISION - removing a presumed-benign mass that turns out to be a sarcoma without margins - is a recognised catastrophe: Unplanned initial surgery of malignant foot/ankle tumours is associated with significantly HIGHER local RECURRENCE (about 50% vs about 22%) and worse outcomes than planned surgery, and reinforces referral to a specialist tumour centre.
- THE FOOT SYNOVIAL SARCOMA HAS A CHARACTERISTIC PROFILE that should raise suspicion rather than lower it: the patient is YOUNGER than other soft-tissue sarcoma patients (median 30 years), the mass has typically been present a long time - median 14 MONTHS of symptoms before diagnosis - and it is SMALL. In the cited series 10 of 14 patients ultimately required partial-foot or below-knee amputation and only 2 had an attempted limb salvage, while 8 of 14 developed pulmonary metastasis and EVERY patient who metastasised died. Biphasic histology fared better than monophasic.
- A COUNTER-INTUITIVE FINDING worth stating precisely so it is not misread: in that series patients with a LONGER symptom duration before diagnosis had BETTER outcomes. This is not evidence that delay is safe - the authors' interpretation is that tumours which sat for a long time without declaring themselves were biologically LESS AGGRESSIVE to begin with. It is a statement about tumour biology, not a licence to wait.
- MANAGEMENT therefore depends on the diagnosis: benign symptomatic lesions are treated on their own merits (e.g. excision of a symptomatic GCT of tendon sheath, marginal excision of a problematic plantar fibroma with its recurrence risk), whereas malignancy requires multidisciplinary care with wide excision (often demanding in the foot, sometimes amputation/ray amputation) plus chemotherapy/radiotherapy as indicated - the single most important orthopaedic responsibility is to NOT excise an unknown mass unplanned.
- “A foot/ankle mass is MALIGNANT UNTIL PROVEN OTHERWISE - solid, enlarging, deep, fixed, painful or recurrent = work it up before any surgery. Synovial sarcoma is the classic 'looks-like-a-ganglion' trap, and it presents SMALL, so do not use a size cut-off to decide.
- “Pathway = IMAGE (XR + MRI, stage) -> properly-PLANNED BIOPSY (excisable tract) -> REFER to a tumour unit -> definitive surgery. Never the unplanned 'whoops' excision.
- “Commonest soft-tissue sarcoma of foot = synovial sarcoma; commonest bony malignancy = osteosarcoma. Unplanned excision ~doubles local recurrence (~50% vs ~22%).
A small foot mass excised as a 'ganglion' that proves to be a synovial sarcoma - now there is tumour in the wound, contaminated planes, and a far harder, often mutilating, re-resection.
Malignant until proven otherwise. Image (XR + MRI), then a planned biopsy with an excisable tract, then refer to a tumour unit - all before any excision. Earn the benign label.
The Spectrum - Benign vs Malignant
- Examples
- Ganglion, plantar fibroma (Ledderhose), GCT of tendon sheath, synovial chondromatosis, lipoma, schwannoma
- Notes
- Common; ganglion is commonest; plantar fibroma recurs after marginal excision
- Examples
- Simple/aneurysmal bone cyst, osteochondroma, enchondroma, osteoid osteoma, subungual exostosis
- Notes
- Calcaneus a common cyst site; treat on own merits
- Examples
- Synovial sarcoma (commonest), other sarcomas; SCC, melanoma (acral/subungual)
- Notes
- Synovial sarcoma small/near joints/may calcify - classic 'ganglion' mimic
- Examples
- Osteosarcoma (commonest), Ewing sarcoma, chondrosarcoma
- Notes
- Rare; acrometastasis (metastasis to foot) very rare
Re-think a 'benign' label if the mass is: solid (not transilluminating), deep to fascia, fixed, enlarging, painful, recurs after a previous 'ganglion' excision, or shows calcification/bone destruction on imaging. Any of these mandates MRI and a planned biopsy before surgery.
A large mass is concerning, but a small one is not reassuring. Size thresholds borrowed from thigh or shoulder referral criteria do not transfer to the foot, where the confined compartments make a sarcoma symptomatic while it is still small - and where, in the cited series, tumour size carried no prognostic weight. Treat size as one feature among several, never as the filter that decides whether to investigate.
Don't Miss Skin Malignancy: Acral and Subungual Melanoma
The "foot mass" trap is not only the subcutaneous sarcoma - the foot is the classic site for acral lentiginous melanoma and subungual melanoma, repeatedly mistaken for benign skin or nail problems.
- Acral lentiginous melanoma (sole, heel, web spaces) is mistaken for a wart, callus, chronic ulcer or blood blister; it is the melanoma subtype least related to sun exposure and tends to present late.
- Subungual melanoma is mistaken for a subungual haematoma, fungal nail (onychomycosis) or paronychia - a pigmented nail streak that is new, widening or changing, especially with Hutchinson's sign (pigment spreading onto the nail fold/periungual skin), is melanoma until proven otherwise.
- Amelanotic (non-pigmented) variants are especially deceptive.
- Biopsy any non-healing acral ulcer, atypical pigmented lesion, or suspicious nail-unit pigmentation rather than treating it repeatedly as a wart or fungal nail.
- Use the ABCDE features for skin lesions and the nail "ABCDEF" (Age/race, Band, Change, Digit, Extension [Hutchinson], Family history) for the nail unit.
- A non-healing wound or sinus can also harbour a squamous cell carcinoma (Marjolin's ulcer). Refer suspicious lesions for biopsy/excision by the appropriate skin-cancer or sarcoma service.
The Safe Pathway: Image -> Biopsy -> Refer
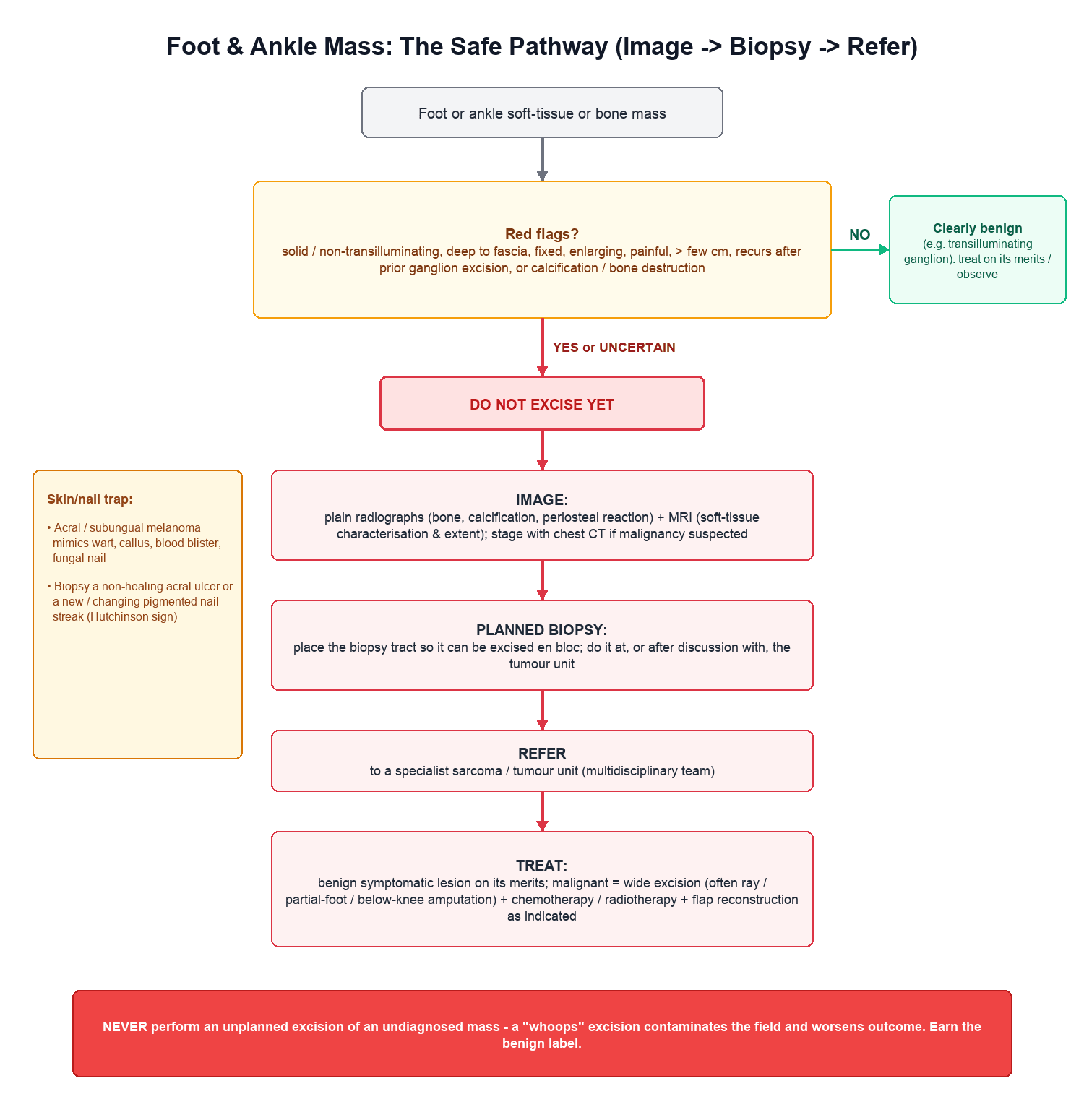
- Image: plain radiographs (bone, calcification, periosteal reaction) and MRI (soft-tissue characterisation and local extent); stage (chest CT, etc.) when malignancy is suspected.
- Biopsy - properly planned: the biopsy tract must be placed so it can be excised en bloc with the tumour at definitive surgery; ideally performed at, or after discussion with, the tumour unit that will do the definitive resection - a poorly placed biopsy can compromise limb salvage.
- Refer: suspected malignancy goes to a specialist sarcoma/tumour unit for multidisciplinary management.
- Then treat: benign symptomatic lesions on their merits; malignancy with wide excision (technically demanding in the foot; sometimes ray amputation/amputation) plus chemotherapy/radiotherapy as indicated.
The single most important orthopaedic responsibility with a foot or ankle mass is to NOT perform an unplanned excision of an undiagnosed lesion. Malignant foot tumours are rare and easily mistaken for benign lumps, and removing one without a diagnosis and without margins contaminates the surgical field, mandates a far more extensive re-resection, and - as shown in published series - is associated with a markedly higher local recurrence rate and worse outcome than a planned, margin-controlled operation. If you are not certain a mass is benign, image it, biopsy it properly (or refer for biopsy), and involve a tumour unit before any definitive surgery. Earn the benign label; do not assume it.
Why the Foot Is Hard: Margins, Amputation and Reconstruction
The principle of "wide excision" is far harder to deliver in the foot than elsewhere, which is exactly why preventing the unplanned excision matters so much.
- Minimal soft-tissue envelope and dense anatomy: the foot has little subcutaneous cover, tightly packed compartments, and tendons and neurovascular bundles close to the skin, so a true wide margin around a sarcoma often cannot be achieved without sacrificing essential structures.
- Weight-bearing and function: the plantar weight-bearing surface tolerates resection and grafting poorly, further constraining limb salvage.
- Amputation is more often required: achieving adequate margins frequently means ray amputation, partial-foot (transmetatarsal or midfoot) amputation, or below-knee amputation rather than marginal local excision - and a prior unplanned ('whoops') excision, by contaminating the planes, makes amputation or a much larger salvage resection more likely.
- Adjuncts to enable salvage: neoadjuvant or adjuvant radiotherapy (for high-grade soft-tissue sarcoma) and chemotherapy (osteosarcoma, Ewing sarcoma) are used as indicated, and soft-tissue flap reconstruction may be needed to close a limb-salvage defect.
- Margins and staging are defined and applied within the multidisciplinary team (the Enneking surgical-staging system and the intralesional/marginal/wide/radical margin definitions are developed in Enneking Staging).
Why Size Is the Wrong Filter in the Foot
Referral criteria for soft-tissue masses elsewhere in the limb lean heavily on size, and applying that habit to the foot is dangerous, because the lesion that most often kills here does not obey it.
In a series of 14 patients with synovial sarcoma of the foot and ankle, tumour size was not a prognostic variable. The foot's confined compartments mean a sarcoma becomes symptomatic, and is noticed, while still small - so a mass that fails a size threshold has not been reassured, it has merely been measured. The red flags that matter here are the qualitative ones: solid rather than transilluminating, deep to fascia, fixed, enlarging, painful, recurrent after a previous "ganglion" excision, or calcified.
- Figure
- Median 30 years - younger than other soft-tissue sarcomas
- What it means at the bedside
- A firm foot lump in a young adult is not reassuring because of their age; it is more concerning
- Figure
- Median 14 months
- What it means at the bedside
- This quantifies the misdiagnosis problem - patients are typically carrying the lesion for over a year while it is treated as something benign
- Figure
- Not prognostic in this series
- What it means at the bedside
- Do not use a size cut-off to decide whether a foot mass needs imaging and biopsy
- Figure
- 10 of 14 had partial-foot or below-knee amputation; only 2 had attempted limb salvage by wide resection
- What it means at the bedside
- Wide margins in the foot usually mean losing part of it - which is the real cost of a delayed or contaminated diagnosis
- Figure
- 8 of 14 developed it, and every patient who did died of their disease
- What it means at the bedside
- The stakes of getting the first operation wrong
- Figure
- Biphasic did better than monophasic
- What it means at the bedside
- Subtype, not size, carried prognostic weight
One finding in that series is easy to misread and worth stating carefully: patients with a longer duration of symptoms before diagnosis had better outcomes. That is not an argument that delay is harmless. The authors' interpretation is that tumours which had been present for a long time without declaring themselves were biologically less aggressive in the first place - the indolent lesions are the ones that survive long enough to be diagnosed late. It is a statement about tumour biology, not about the safety of waiting.
Size thresholds used for thigh or shoulder masses do not transfer to the foot. Synovial sarcoma here presents small, in a young patient, with a median 14 months of symptoms before anyone makes the diagnosis - and in the cited series size carried no prognostic weight at all. Decide on the qualitative red flags and on uncertainty, never on a centimetre count.
Mnemonics & Memory Aids
WHOOPS
Hook:WHOOPS - the unplanned excision is what you must avoid: Watch red flags, Hold the knife, Obtain imaging, Organise a planned biopsy, Pass to a unit, remember Synovial sarcoma.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient is referred with a 3 cm firm lump on the dorsum of the foot that the GP thinks is a ganglion. How do you approach it?”
Principle
- A foot/ankle mass is MALIGNANT until proven otherwise
- Malignant lesions are rare and frequently misdiagnosed as benign
- Earn the benign label by proper assessment - don't assume it
Commonest lesions
- Benign: ganglion (commonest), plantar fibroma, GCT of tendon sheath, cysts, osteochondroma
- Malignant soft tissue: synovial sarcoma (commonest) - the classic ganglion mimic
- Malignant bone: osteosarcoma (commonest), Ewing, chondrosarcoma
Safe pathway
- Image: radiograph + MRI; stage if malignancy suspected
- Planned biopsy: tract excisable en bloc; do/discuss at the tumour unit
- Refer to a specialist sarcoma centre before definitive surgery
Why it matters
- Unplanned 'whoops' excision ~doubles local recurrence (50% vs 22%) and worsens mortality (10% vs 6%)
- Definitive malignant care = wide excision +/- chemo/radiotherapy (MDT)
Foot synovial sarcoma profile
- Younger than other STS patients (median 30 years)
- Median 14 months of symptoms BEFORE diagnosis - the misdiagnosis problem, quantified
- Tumour size NOT prognostic - a small foot mass is not a safe foot mass
- 10 of 14 needed partial-foot or below-knee amputation; only 2 limb salvage
- 8 of 14 developed lung metastases and all of those died
- Longer symptom duration correlated with BETTER outcome = less aggressive biology, NOT safe delay
Evidence & Key Studies
Malignant bone and soft-tissue lesions of the foot
- Malignant tumours of the foot are rare and, because of their rarity, are often misdiagnosed - resulting in inadequate (unplanned) excision and poor outcomes.
- A correct approach with careful clinical examination and radiological study, followed by a properly performed biopsy, is mandatory to avoid these pitfalls.
- The review covers the clinicopathological presentation, imaging features and current treatment of the common malignant bone and soft-tissue lesions of the foot, including synovial sarcoma.
Malignant tumors of the foot and ankle - unplanned surgery worsens outcome
- In 80 malignant foot/ankle tumours, synovial sarcoma was the most common soft-tissue tumour and osteosarcoma the most common osseous tumour; most arose from soft tissue (78%).
- Unplanned initial surgery (excision without prior biopsy at an outside institution) was associated with a higher local recurrence rate (50% vs 22%) and higher mortality (10% vs 6%) than planned surgery.
- The authors reinforce that these patients should be referred for treatment at a centre with specialised expertise in tumour management.
Synovial sarcoma of the foot and ankle
- Fourteen patients with synovial sarcoma of the foot and ankle; patients were younger than those with other soft-tissue sarcomas (median 30 years) and had a median symptom duration of 14 months before diagnosis.
- Tumour size was not a prognostic variable; biphasic histology did better than monophasic, and patients with a longer symptom duration fared better - which the authors attribute to those tumours being biologically less aggressive rather than to delay being harmless.
- Ten of the 14 underwent partial-foot or below-knee amputation and only two an attempted limb salvage by wide resection; 8 of 14 developed pulmonary metastasis and every patient who did died of their disease.
The rarity and frequent misdiagnosis of malignant foot tumours and the mandatory exam-imaging-biopsy approach come from the cited Angelini review, and the worse outcomes of unplanned ('whoops') excision (50% versus 22% local recurrence and 10% versus 6% mortality, in 80 malignant foot and ankle tumours of which 78% arose from soft tissue) with the recommendation to refer to a specialist tumour centre from the cited Karaca series. The synovial sarcoma figures - median age 30, median 14 months to diagnosis, size not prognostic, 10 of 14 amputated, 8 of 14 with pulmonary metastasis all of whom died - are Scully, a single-centre series of only 14 patients from 1999, so the proportions should be read as the experience of one unit rather than as population rates; the direction of those findings is nonetheless the basis for treating a small foot mass as unreassured.
No verified figure was identified for what proportion of foot masses are malignant, which is why malignancy is described as rare and most lumps as benign without a rate attached. The benign versus malignant spectrum, the red flags and the principle that a foot mass is malignant until proven otherwise are standard, well-established teaching. (See also Synovial Sarcoma, Plantar Fibromatosis, Aneurysmal Bone Cyst, Osteochondroma, Subungual Exostosis, Biopsy Principles & Techniques, Enneking Staging and Marjolin's Ulcer.)