Safe Dislocation | Trochanteric Flip Osteotomy | MFCA Preservation | Retinacular Vessels | FAI | Intra-articular Access | AVN Prevention
- The entire premise of the Ganz technique is that the deep branch of the medial femoral circumflex artery (MFCA) is preserved by keeping it within the retinacular flap attached to the trochanteric fragment - this is why AVN is rare when the technique is performed correctly
- The trochanteric osteotomy must be performed anterior to the trochanteric fossa and must NOT extend into the piriformis fossa - the MFCA runs along the posterosuperior femoral neck within the retinacular flap and is at its most vulnerable during osteotomy and dislocation
- Surgical dislocation gives 360-degree visualisation of the femoral head and entire acetabulum - no other approach provides equivalent access while preserving femoral head vascularity
- Indications include femoroacetabular impingement (FAI) treatment, intra-articular loose body removal, acetabular labral repair, femoral head osteochondral lesions, Pipkin fractures, and early AVN staging
- The approach is performed in the lateral decubitus position with the leg draped free, allowing controlled anterior dislocation of the hip by flexion, adduction and external rotation
- “Examiners want you to demonstrate understanding of the vascular anatomy - the MFCA and its retinacular branches are the KEY to why this approach works safely
- “The trochanteric osteotomy is NOT a standard greater trochanteric osteotomy - it is an anterior, thin-slice osteotomy that leaves the posterior soft-tissue envelope intact
- “The most dangerous step is anterior dislocation - the hip must be gently flexed, adducted and externally rotated; forceful manipulation can tear the retinacular vessels
- “Always mention the Bernese group (Ganz) when discussing this technique - it is their landmark contribution to hip preservation surgery
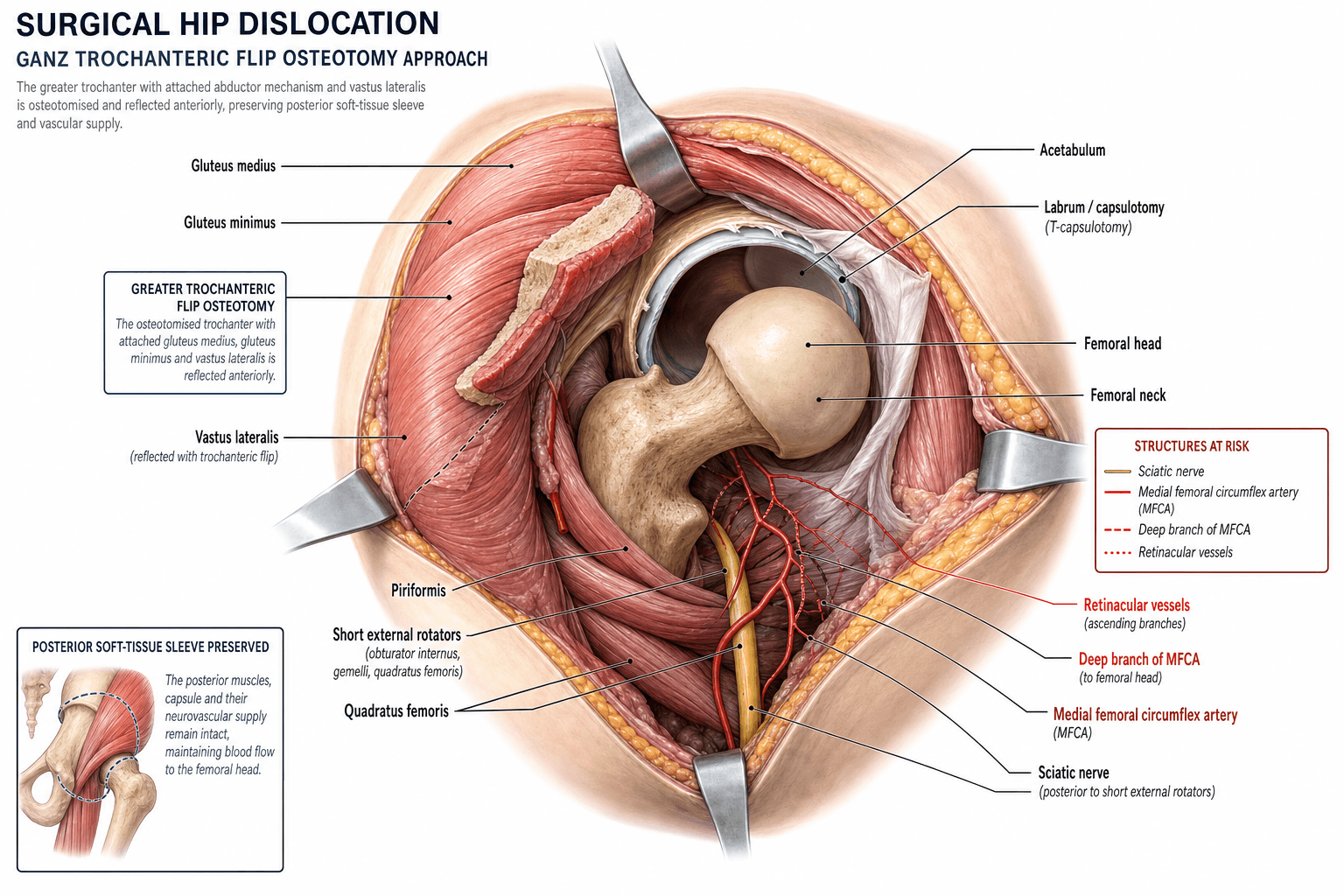
Surgical Hip Dislocation (Ganz Trochanteric Flip)
The Ganz technique is safe only when the vascular anatomy is understood and respected. The deep branch of the medial femoral circumflex artery (MFCA) pierces the hip capsule at the posterosuperior aspect and runs along the femoral neck within the retinacular flap. If the trochanteric osteotomy is too thick (posterior), if the short external rotators are divided too close to the femur, or if the hip is dislocated forcefully, the MFCA or its retinacular branches can be lacerated, stretched or thrombosed. The result is avascular necrosis of the femoral head - a catastrophic complication in a young patient.
- Best approach
- Ganz surgical dislocation (trochanteric flip)
- Reasoning
- 360-degree visualisation of femoral head and acetabulum; allows osteochondroplasty, labral repair, and direct assessment of chondral damage; preserves femoral head vascularity
- Best approach
- Hip arthroscopy
- Reasoning
- Less invasive; faster recovery; equivalent outcomes for isolated labral repair in experienced hands; but limited for complex or combined FAI pathology
- Best approach
- Kocher-Langenbeck or surgical dislocation
- Reasoning
- Surgical dislocation provides direct joint surface visualisation and is preferred when femoral head assessment is critical; Kocher-Langenbeck provides posterior column access without dislocation
- Best approach
- Ganz surgical dislocation
- Reasoning
- Allows extraction of loose fragments, ORIF of the femoral head, and assessment of femoral head vascularity; the approach itself does not devascularise the head when performed correctly
Overview and Indications
The Ganz surgical dislocation of the hip is a joint-preserving surgical approach that provides 360-degree visualisation of the femoral head and the entire acetabulum while preserving the blood supply to the femoral head. It was developed by Reinhold Ganz and colleagues at the University of Bern (Inselspital) in the 1990s and published as a reproducible technique in 2001. The approach has transformed the management of young adult hip pathology, particularly femoroacetabular impingement (FAI).
the blood supply to the femoral head is predominantly from the deep branch of the medial femoral circumflex artery (MFCA), which courses along the posterosuperior femoral neck within a synovial retinacular fold. By performing a specific anterior trochanteric flip osteotomy that preserves the posterior soft-tissue envelope (including the short external rotators and the MFCA retinacular branches), the hip can be safely dislocated anteriorly without devascularising the femoral head.
- Femoroacetabular impingement (FAI) - cam, pincer, or mixed type requiring osteochondroplasty, acetabuloplasty, labral repair or refixation
- Intra-articular loose bodies - synovial chondromatosis, fracture fragments, osteochondral loose bodies
- Femoral head fractures - Pipkin type I and II, allowing ORIF with direct joint visualisation
- Acetabular fractures - posterior wall, transverse, and T-type fractures where joint surface visualisation is essential
- Early avascular necrosis - staging, core decompression, or bone grafting under direct vision
- Slipped capital femoral epiphysis (SCFE) - modified Dunn procedure for realignment with vascular protection
- Pigmented villonodular synovitis (PVNS) and other synovial pathology requiring complete synovectomy
- Complex labral pathology - labral reconstruction, refixation in the setting of dysplasia or FAI
- Chondral lesions - assessment and treatment of osteochondral defects of the femoral head
- Legg-Calve-Perthes disease deformity correction in the healed stage
- Post-traumatic deformity of the femoral head or acetabular rim
- Ischiofemoral impingement requiring lesser trochanteric osteoplasty
- Revision after failed hip arthroscopy with residual impingement
Key contraindications include advanced osteoarthritis (Tonnis grade 3), obesity (BMI greater than 35-40 makes positioning and exposure difficult), severe dysplasia (where a periacetabular osteotomy is more appropriate), active infection, and pre-existing femoral head avascular necrosis with collapse (where the head is already unsalvageable). Examiners test whether you know when NOT to open the hip joint.
A named deformity-correction application of surgical dislocation worth being able to describe is relative femoral neck lengthening, used for the coxa breva / coxa magna with a high-riding (over-grown) greater trochanter seen after healed Legg-Calve-Perthes disease or post-SCFE/AVN deformity:
- The problem: a short, wide neck with a relatively overgrown trochanter causes abductor weakness (shortened lever arm, Trendelenburg), extra-articular (trochanteric-pelvic) impingement and intra-articular impingement from the aspherical head.
- The procedure (via Ganz dislocation): the trochanteric flip is performed, the redundant lateral femoral neck is resected/contoured down to the head-neck junction (head-neck osteochondroplasty), and the greater trochanter is distalised and advanced (re-fixed more distally and laterally) - this lengthens the neck relative to the trochanter, restores the abductor lever arm and offset, and relieves both intra- and extra-articular impingement.
- Vascular safety: it is done under the same MFCA-protecting principles (and, for major neck reshaping, an extended retinacular flap - see below) so the head is not devascularised.
Exam point: a healed-Perthes hip with coxa breva, a high trochanter and a positive Trendelenburg is the classic indication for relative neck lengthening with trochanteric distalisation/advancement through a surgical dislocation.
Relevant Anatomy and Vascular Considerations
The blood supply to the adult femoral head is predominantly from the medial femoral circumflex artery (MFCA), with a minor contribution from the lateral epiphyseal vessels (from the MFCA retinacular branches) and the artery of the ligamentum teres (variable and usually insufficient to sustain the head alone).
- The deep branch of the MFCA originates from the profunda femoris artery, passes posteriorly between the pectineus and iliopsoas tendons, then courses between the obturator externus and adductor brevis muscles. It pierces the hip capsule at the posterosuperior aspect of the femoral neck.
- At the capsule, the MFCA gives off retinacular branches that run along the posterosuperior femoral neck within a synovial fold (the retinaculum of Weitbrecht). These are the superior retinacular arteries (also called lateral epiphyseal arteries) - the dominant supply to the weight-bearing segment of the femoral head.
- The MFCA forms an extracapsular anastomotic ring at the base of the femoral neck with branches of the lateral femoral circumflex artery and the inferior gluteal artery.
the trochanteric flip osteotomy is designed so that the entire retinacular vascular chain remains attached to the trochanteric fragment and the posterior soft tissues. The osteotomy is performed anterior to the insertion of the external rotators, and the short external rotators (obturator internus, gemelli, piriformis) are NOT divided - they are mobilised posteriorly with the trochanteric fragment, carrying the MFCA within their protective soft-tissue envelope.
- The gluteus medius inserts on the posterosuperior and lateral greater trochanter
- The gluteus minimus inserts on the anterior facet of the greater trochanter
- The vastus lateralis originates from the inferior aspect of the greater trochanter
- The trochanteric fossa (digital fossa) is the posterior depression where the obturator externus tendon inserts - the osteotomy must NOT extend into this fossa
- The piriformis fossa is the entry point for the MFCA deep branch - this must be protected
- The hip capsule attaches to the acetabular labrum and transverse ligament centrally and to the intertrochanteric line anteriorly and the femoral neck posteriorly (mid-neck level)
- The Z-shaped capsulotomy used in the Ganz technique runs from the anterosuperior acetabular rim along the femoral neck, then turns posterosuperiorly along the head-neck junction, avoiding the inferior capsule where additional retinacular vessels may be present
Internervous Plane and Surgical Interval
The Ganz surgical dislocation does not follow a classic internervous plane. Instead, it uses a soft-tissue preserving approach that maintains the neurovascular integrity of the posterior structures.
- A lateral or posterolateral skin incision is made centred over the greater trochanter, extending approximately 15-20 cm. The incision can be straight (standard) or slightly curved posteriorly (modified Gibson approach).
- The iliotibial band (ITB) is incised in line with the skin incision, and the gluteus maximus fibres are split bluntly along their posterior border if a Gibson-type approach is used.
- The anterior border of the gluteus medius is identified. The trochanteric osteotomy is performed with an oscillating saw in the sagittal plane, approximately 1-1.5 cm thick at the base, from the posterosuperior aspect of the greater trochanter to a point just distal to the anterior trochanteric ridge.
- The osteotomy is directed from posterior to anterior, leaving the gluteus medius attachment on the trochanteric fragment superiorly and the vastus lateralis origin attached inferiorly. This creates a mobile osteotomised fragment that can be flipped anteriorly with its muscle attachments.
- The short external rotators (piriformis, obturator internus, gemelli) remain attached to the intact posterior femur - they are NOT detached. The MFCA runs deep to these muscles and is protected by keeping them intact.
- The trochanteric fragment, with the gluteus medius and vastus lateralis attached, is mobilised anteriorly by releasing the gluteus minimus from the anterior capsule (the gluteus minimus tendon inserts on the anterior facet and must be carefully elevated).
- The capsule is now exposed anteriorly, superiorly, and posterosuperiorly.
The trochanteric osteotomy must be (1) thin (approximately 1-1.5 cm), (2) directed from posterior to anterior in the sagittal plane, (3) at the junction of the greater trochanter and the femoral neck, and (4) must NOT extend into the trochanteric fossa or piriformis fossa. A thick or mal-directed osteotomy risks lacerating the MFCA as it enters the retinacular fold. The short external rotators are NEVER divided in the Ganz technique.
Patient Positioning and Setup
- Position: lateral decubitus with the affected hip uppermost. The patient is stabilised with a peg-board, beanbag, or lateral hip positioner. The leg is draped completely free to allow full range of motion including flexion, adduction, external rotation (for dislocation) and extension, abduction, internal rotation (for reduction and acetabular work).
- Anaesthesia: general anaesthesia with muscle relaxation is preferred to allow controlled dislocation without resistance. Supplemental regional blocks (lumbar plexus or fascia iliaca) may be used for post-operative analgesia.
- Traction: no formal traction table is used. The assistant provides manual traction as needed during dislocation and reduction. A sterile pocket or leg holder may be used to support the leg when the hip is dislocated.
- Fluoroscopy: intra-operative fluoroscopy is used to confirm osteotomy position, femoral neck osteoplasty adequacy, and trochanteric fragment reduction and fixation. The C-arm is positioned for AP and lateral views of the hip.
- Instruments: standard hip instrumentation plus fine osteotomes (for femoral neck osteoplasty), a femoral head sizer or templating guide, labral repair anchors (suture anchors for labral refixation), and small fragment fixation set for trochanteric fixation (typically 3.5 mm or 4.5 mm screws).
- Positioning precautions: ensure the peroneal nerve is free of pressure at the fibular head of the dependent leg. Protect the axilla and brachial plexus of the dependent arm with an axillary roll.
Surgical Technique
The patient is positioned lateral. A straight lateral or modified Gibson skin incision is made, centred over the greater trochanter, extending approximately 15-20 cm. The fascia lata and gluteus maximus are split. The anterior border of the gluteus medius is identified and the trochanteric bursa is excised for exposure.
The trochanteric osteotomy is marked and performed with an oscillating saw. The cut is in the sagittal plane, beginning just posterior to the tip of the greater trochanter and directed anteriorly and distally, exiting just distal to the anterior trochanteric ridge. The fragment thickness is approximately 1-1.5 cm at the base. The saw cut must stay anterior to the piriformis fossa.
The trochanteric fragment (with attached gluteus medius superiorly and vastus lateralis inferiorly) is mobilised anteriorly. The gluteus minimus is carefully released from its insertion on the anterior capsule, preserving the muscle belly. The fragment is flipped anteriorly, exposing the anterior and superior hip capsule. The capsule is cleaned of overlying tissue.
A Z-shaped capsulotomy is performed: the first limb runs along the anterosuperior acetabular rim (from the anterior margin of the reflected head of rectus femoris to the posterosuperior rim), and the second limb runs along the femoral neck from the first limb's termination, directed inferoposteriorly along the head-neck junction. This exposes the femoral head and the acetabular labrum.
The repeatedly-cited modified Dunn procedure deserves its own answer, because it is the highest-stakes application of surgical dislocation and depends on the extended retinacular soft-tissue flap - an evolution of the basic technique:
- The extended retinacular flap: after the trochanteric flip and capsulotomy, the synovial retinacular fold carrying the MFCA terminal branches is mobilised off the posterosuperior neck as a soft-tissue flap (a "second" osteotomy of a step of trochanter can be raised with it). This frees the surgeon to resect the metaphyseal neck and reposition the epiphysis without putting the vessels on stretch - the vessels travel with the flap rather than being tethered to the neck.
- The modified Dunn procedure uses this to treat moderate-to-severe and unstable slipped capital femoral epiphysis (SCFE): the callus/metaphyseal prominence is removed, the epiphysis is reduced anatomically onto the neck under direct vision and fixed, correcting the deformity at its source while the retinacular flap protects perfusion (often monitored intra-operatively).
- The caveat examiners want: despite the elegant vascular protection, the modified Dunn in unstable SCFE still carries a real AVN risk (reported in a meaningful minority), so it is a specialist procedure and the consent/risk discussion is critical; it is not a guaranteed AVN-free operation.
Exam point: modified Dunn = surgical-dislocation subcapital realignment of SCFE using an extended retinacular flap to reduce the epiphysis without tensioning the MFCA - powerful for deformity correction but with a genuine residual AVN risk in unstable slips.
The posterosuperior femoral neck is the territory of the retinacular vessels. During the entire procedure - capsulotomy, dislocation, femoral osteoplasty, and reduction - NO dissection or retraction should occur on the posterosuperior neck surface. The MFCA retinacular branches run in the synovial fold here and are the sole dominant blood supply to the weight-bearing femoral head. Even minor trauma to these vessels can cause segmental AVN.
Structures at Risk and Complications
The Ganz surgical dislocation has a well-documented safety profile when performed by experienced surgeons, but carries specific risks related to the trochanteric osteotomy, vascular anatomy, and nerve proximity.
- Avascular necrosis (AVN) of the femoral head - the most feared complication. Reported rates are 0-2% in large series when the technique is performed correctly. AVN typically manifests within the first 12-24 months post-operatively with progressive groin pain and radiographic changes. Risk factors include incorrect osteotomy (too posterior, entering the piriformis fossa), forceful dislocation (tearing the retinacular vessels), and pre-existing compromised vascularity (e.g., previous SCFE, Perthes disease).
- Trochanteric nonunion or malunion - reported in approximately 1-3% of cases. Risk factors include inadequate fixation, poor bone quality, early weight-bearing, and large fragment size. Presents with lateral hip pain, weakness on abduction, and a positive Trendelenburg sign. Treatment ranges from observation (fibrous union that is asymptomatic) to revision fixation with bone grafting.
- Sciatic nerve injury - neuropraxia of the sciatic nerve from retraction occurs in approximately 1% of cases. The peroneal division is more susceptible. Most resolve within 3-6 months. The nerve is at risk during posterior capsular exposure and acetabular work. Careful retraction and avoiding prolonged posterior retraction are protective.
- Heterotopic ossification (HO) - reported in approximately 5-8% of cases without prophylaxis. Prophylaxis with indomethacin (75 mg daily for 3-6 weeks) or a single dose of post-operative radiation (700 cGy) reduces this risk. HO is more common when extensive acetabular rim work or bone grafting is performed.
- Abductor weakness - transient weakness of hip abduction is common due to the trochanteric osteotomy and gluteus medius dissection. Most patients recover abductor strength by 6-12 months. Persistent weakness may indicate trochanteric nonunion or failure of the gluteus medius repair.
- Infection - deep infection is rare (less than 1%) but catastrophic in a young patient with a native hip joint. Standard peri-operative antibiotic prophylaxis (cephalosporin or clindamycin) is mandatory.
- Femoral neck fracture - rare but reported, particularly when extensive cam osteoplasty is performed (over-resection of the femoral neck cortex weakens the structural integrity). A resection of greater than 30% of the femoral neck diameter significantly increases fracture risk.
- Chondral damage progression - pre-existing chondral damage may progress despite successful impingement correction, leading to early osteoarthritis. This is not a complication of the technique per se but a limitation related to the underlying pathology.
- Persistent impingement - inadequate resection of the cam or pincer lesion leads to residual impingement and persistent symptoms. Intra-operative fluoroscopic confirmation of adequate resection is essential.
In the viva, lead with AVN (0-2%, technique-dependent, devastating) and trochanteric nonunion (1-3%, most common mechanical complication). Then mention sciatic neuropraxia, HO, and abductor weakness. Examiners want to see that you understand WHY AVN is rare with this technique (vessel preservation) and HOW it occurs when it does happen (incorrect osteotomy or forceful dislocation).
Guidelines, Registries and Global Practice
There is no single universal guideline for surgical hip dislocation; practice follows evidence-based principles and surgeon experience. Several international organisations have published guidance relevant to the indications and technique:
- AAOS (US): the AAOS clinical practice guideline for non-arthroplasty management of OA of the hip recognises FAI treatment as a developing area. Surgical dislocation is supported as an option for comprehensive FAI correction when arthroscopic treatment is insufficient or when the pathology requires open visualisation. AAOS has endorsed labral refixation over resection when technically feasible.
- BOA/BHS (UK): the British Hip Society supports surgical dislocation as a joint-preserving option for complex FAI, femoral head fractures (Pipkin), and intra-articular pathology requiring direct visualisation. The technique is typically performed in specialist hip preservation units.
- EFORT/European consensus: European centres (particularly Bern, Munich, Lausanne, and other high-volume hip preservation centres) have extensive experience with the Ganz technique. European practice has historically favoured open surgical dislocation more than North American practice, where hip arthroscopy gained earlier widespread adoption.
- No national arthroplasty registry specifically tracks surgical dislocation procedures, as they are joint-preserving operations. However, conversion rates to total hip arthroplasty after surgical dislocation are tracked in institutional series and provide surrogate survivorship data.
- Large institutional series from Bern, Melbourne, and Boston report conversion to THA in approximately 10-15% at 10 years, predominantly in patients with pre-existing chondral damage or advanced FAI at the time of the index procedure.
- The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) captures data on patients who subsequently undergo THA after hip preservation procedures, providing real-world conversion rate data.
- European surgeons (particularly in Switzerland, Germany, and France) have the longest experience with surgical dislocation and continue to favour it for complex FAI pathology. The Bernese group's influence remains strong.
- North American practice has shifted toward hip arthroscopy as the first-line treatment for FAI, with surgical dislocation reserved for complex or revision cases, pincer-type FAI requiring extensive rim work, and femoral head fractures. The threshold for open dislocation varies significantly between centres.
- Asian practice, particularly in Japan and South Korea, follows a similar pattern with arthroscopy as first-line and surgical dislocation for complex cases.
- In low- and middle-income settings, surgical dislocation may be more commonly used than arthroscopy due to the lower capital equipment costs (no arthroscopy tower required), though the technical expertise required limits its availability.
- The modified Dunn procedure (surgical dislocation for SCFE deformity correction in the acute or chronic setting) is increasingly adopted in paediatric orthopaedic centres worldwide, with specific protocols for vascular monitoring.
- Combined approaches (surgical dislocation with periacetabular osteotomy for FAI with dysplasia) are performed in specialist centres for complex hip deformity.
- Advances in hip arthroscopy continue to expand the scope of what can be treated arthroscopically, narrowing the indications for open dislocation, but the Ganz approach remains essential for pathology that cannot be addressed arthroscopically.
Memory Aids
RETINACULARVascular Anatomy of the Femoral Head - RETINACULAR
Hook:RETINACULAR spells out every step of vascular protection - the entire rationale for the Ganz technique is keeping this vessel chain intact
HIPIndications for Surgical Dislocation - HIP ACCESS
Hook:HIP ACCESS covers every indication - if you need to SEE the femoral head and acetabulum fully, Ganz dislocation is the answer
FLIPComplications After Ganz Dislocation - FLIP GUARD
Hook:FLIP GUARD reminds you of every complication - AVN is the most feared but FLIP-related trochanteric issues are the most common
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male semi-professional footballer presents with 18 months of progressive left groin pain, worse with deep flexion and twisting activities. Examination reveals limited internal rotation (10 degrees) and a positive anterior impingement test. Radiographs show a prominent cam lesion at the anterosuperior femoral head-neck junction with an alpha angle of 72 degrees. The acetabular coverage appears normal. MRI confirms a full-thickness chondral defect on the anterosuperior acetabulum with a stable labral tear. Discuss your management.”
“A 35-year-old man sustained a posterior fracture-dislocation of the right hip in a high-speed motor vehicle accident. The hip was reduced in the emergency department within 4 hours. Post-reduction CT shows a Pipkin type II fracture (a displaced infra-foveal fragment of the femoral head) with a small posterior wall acetabular fracture. The hip is concentrically reduced. Discuss the surgical management.”
One-liner
- Safe surgical dislocation of the hip via trochanteric flip osteotomy, developed by Ganz in Bern, preserving the MFCA and its retinacular branches
- Provides 360-degree visualisation of the femoral head and acetabulum without devascularising the femoral head
Vascular anatomy (critical)
- Deep branch of the MFCA is the dominant blood supply to the femoral head
- Runs along the posterosuperior femoral neck within the retinacular fold
- Pierces the capsule posterosuperiorly, protected by the obturator externus tendon
- Terminal branches are the lateral epiphyseal (superior retinacular) arteries
- AVN rate 0-2% when technique is correct
Indications (HIP ACCESS)
- Head fractures (Pipkin), Impingement (FAI), Peri-articular pathology (PVNS)
- Acetabular fractures needing joint visualisation, Chondral assessment
- Capsular/labral repair, Extra-articular impingement
- SCFE (modified Dunn), Septic arthritis debridement
Trochanteric osteotomy rules
- Sagittal plane, posterior to anterior direction
- Approximately 1-1.5 cm thick at the base
- Must NOT extend into piriformis fossa or trochanteric fossa
- Gluteus medius stays attached superiorly, vastus lateralis inferiorly
- Short external rotators are NEVER divided
Key steps
- Lateral decubitus, leg free
- Anterior trochanteric flip with gluteus medius and vastus lateralis attached
- Z-shaped capsulotomy (anterosuperior rim to posterosuperior neck)
- Gentle anterior dislocation (flexion, adduction, external rotation)
- Perform femoral and acetabular work under direct 360-degree vision
- Reduce gently, fix trochanter with 2-3 bicortical screws
Complications (FLIP GUARD)
- Femoral head AVN (0-2%, technique-dependent)
- Loss of trochanteric fixation (1-3%)
- Iatrogenent nerve injury (sciatic neuropraxia approximately 1%)
- Persistent pain/stiffness, HO (5-8% without prophylaxis)
- Gluteal weakness (usually recovers 6-12 months)
- Unrecognised chondral damage changes prognosis
- Arthrosis progression (related to pre-existing damage)
- Reoperation approximately 5-15% at long-term follow-up
- Deep infection less than 1%
Contraindications
- Advanced OA (Tonnis grade 3)
- BMI greater than 35-40 (positioning and exposure difficulties)
- Severe dysplasia (PAO is more appropriate)
- Pre-existing AVN with femoral head collapse
- Active infection
Evidence Base
- In the landmark description of 213 surgical hip dislocations performed in 193 patients, there were no cases of avascular necrosis of the femoral head at a minimum follow-up of 2 years. The technique provided 360-degree access to the femoral head and acetabulum. Complications included trochanteric nonunion (approximately 1.5%), sciatic nerve neuropraxia (approximately 1%), and heterotopic ossification. The authors demonstrated that the deep branch of the MFCA is preserved by the trochanteric flip osteotomy and that the femoral head remains vascularised throughout the procedure.
- Detailed cadaveric dissection of 24 hips mapped the course of the deep branch of the MFCA, demonstrating that it passes between the obturator externus and adductor brevis, then pierces the hip capsule at the posterosuperior femoral neck within the retinacular fold. The deep branch was the dominant arterial supply to the femoral head in all specimens. The study showed that the trochanteric flip osteotomy preserves the MFCA by keeping the posterior soft-tissue envelope intact.
- In a comparison of patients treated with surgical dislocation for FAI, those who underwent labral refixation (re-attachment with suture anchors) had significantly better clinical outcomes and less progression of osteoarthritis at 2-year follow-up compared with those who had labral resection. The 5-year results confirmed that labral preservation was associated with a lower rate of OA progression. Patients with labral refixation had a Merle d'Aubigne score improvement that was significantly greater than the resection group.
- In a series of patients treated with surgical dislocation for FAI, clinical outcomes were good to excellent in approximately 80-85% at mid-term follow-up when chondral damage was limited (Tonnis grade 0-1). Patients with pre-existing full-thickness chondral defects had significantly worse outcomes. The open approach allowed direct visualisation and treatment of cam and pincer pathology with comprehensive correction. Conversion to THA was primarily in patients with advanced pre-operative chondral damage.
- Intra-operative laser Doppler flowmetry was used to measure femoral head perfusion during surgical hip dislocation in 14 patients. Perfusion was maintained throughout the procedure when the Ganz technique was followed correctly. The critical step was the trochanteric flip osteotomy, which preserved the retinacular vessels. Extension or external rotation of the dislocated hip did not significantly reduce perfusion, confirming the safety of anterior dislocation when the retinacular vessels are protected.