A structured way to build a differential | VITAMIN CDEF / VINDICATE | Fast pattern recognition plus slow analysis | Beat the biases that cause diagnostic error
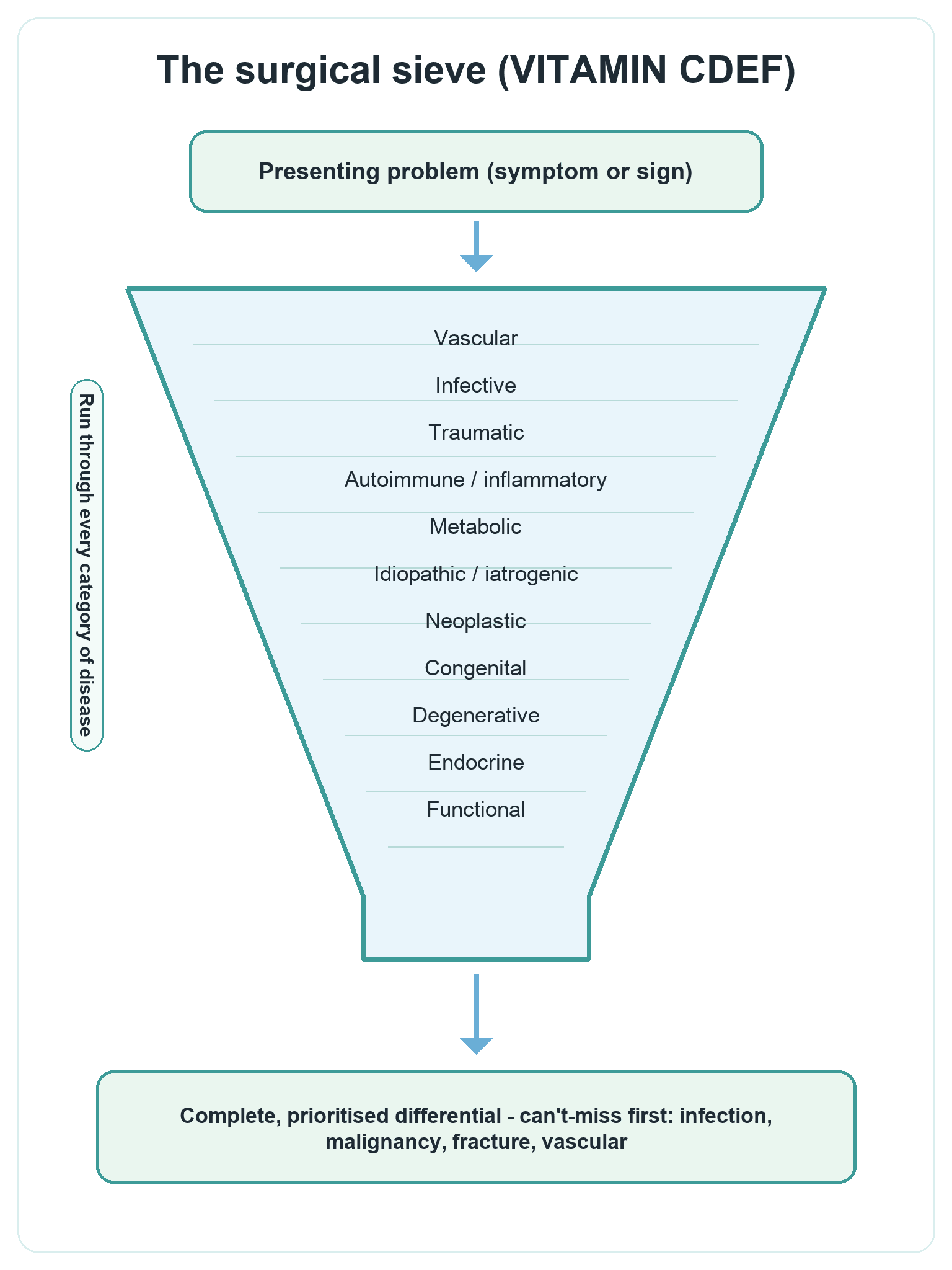
- The surgical sieve is a checklist of categories of disease (vascular, infective, inflammatory, traumatic, autoimmune, metabolic, idiopathic, neoplastic, congenital, degenerative, endocrine, functional) that you run through so your differential is complete rather than just the first thing you thought of
- It is a System 2 (analytical) tool - a deliberate framework that backs up fast pattern recognition (System 1) and stops you committing to the first plausible answer
- Most diagnostic error is a reasoning error, not a knowledge gap - the common culprits are cognitive biases such as anchoring, premature closure, availability and confirmation bias
- In a viva, structure scores marks: starting with a named framework (VITAMIN CDEF or VINDICATE) and a sensible order shows the examiner an organised, safe mind even before you reach the right answer
- The sieve is a tool, not a script - tailor it to the clinical context (a painful joint, a bone lesion, a limping child) and lead with the dangerous and common diagnoses, not an exhaustive list read off in random order
- “If you go blank in a viva, fall back on the sieve out loud - 'I would think about this in categories: vascular, infective, inflammatory...' - it buys time and demonstrates a safe, systematic approach
- “Always say the can't-miss diagnoses first (infection, malignancy, fracture, vascular compromise) - examiners reward safety, not just completeness
- “Premature closure - settling on a diagnosis before it is fully verified - is the single most common reasoning error; the sieve is the antidote
- “Tie the sieve to the patient: a hot swollen joint is septic arthritis until proven otherwise, but the sieve reminds you of gout, reactive arthritis, haemarthrosis and a flare of inflammatory arthritis too
In any viva that asks for a differential or causes, name a structure first - "I would use a surgical sieve, thinking in categories: vascular, infective, inflammatory, traumatic, autoimmune, metabolic, idiopathic, neoplastic, congenital, degenerative, endocrine, functional". Structure shown out loud is what earns marks, even before the right answer.
Examiners reward a safe clinician. Lead with the can't-miss diagnoses for that presentation - infection, malignancy, fracture, vascular compromise - then work through the rest of the sieve. A long list read in random order that buries septic arthritis or tumour scores poorly.
Diagnostic error usually comes from flawed reasoning, not missing knowledge. Know the named biases - anchoring, premature closure, availability bias, confirmation bias, diagnostic momentum - and how a deliberate System 2 cross-check (the sieve) mitigates them.
Do not recite the full sieve mechanically. Filter it through the clinical context - a bone lesion, a hot joint, a limping child - and emphasise the categories that actually matter there. The sieve is a prompt to be complete, not a script to read.
Overview
The surgical sieve is a simple but powerful tool: a checklist of the broad categories of disease (vascular, infective, traumatic, neoplastic, and so on) that you run through to make sure your differential diagnosis is complete. Instead of listing the first two or three diagnoses that spring to mind, you deliberately ask "could this be a vascular cause? an infective cause? a tumour?" and work through every category. It is one of the oldest and most reliable aids to clinical reasoning, and it is exactly the kind of structured thinking examiners want to see.
Clinical reasoning - how a clinician gets from a presenting problem to a diagnosis - is now understood through a dual-process model. System 1 is fast, intuitive pattern recognition (you glance at an x-ray and "just know" it is a scaphoid fracture). System 2 is slow, effortful, analytical thinking (you methodically work through a differential). Experienced clinicians rely heavily on System 1 because it is efficient, but it is also where most snap errors come from. The surgical sieve is a System 2 safety net: a way to deliberately cross-check the intuitive answer against a complete list of possibilities.
For the exam, three threads recur throughout this topic: how to build a complete differential using a named sieve, how the brain actually reasons (the dual-process model and why intuition is both useful and dangerous), and why diagnoses get missed - the cognitive biases that cause diagnostic error and how a structured approach guards against them.
Principles: How the Surgical Sieve Works
The sieve works by forcing breadth before you commit to depth. Faced with a symptom or a sign, you do not jump to the most likely diagnosis - you first generate possibilities across every category of disease, then narrow down using the history, examination and investigations. The categories are remembered with a mnemonic; the two most popular are VITAMIN CDEF and VINDICATE, which cover the same ground.
- What it means
- Problems of blood supply
- Orthopaedic examples
- Avascular necrosis, compartment syndrome, ischaemia, haemarthrosis
- What it means
- Infection of bone, joint or soft tissue
- Orthopaedic examples
- Septic arthritis, osteomyelitis, discitis, necrotising fasciitis
- What it means
- Immune-driven inflammation
- Orthopaedic examples
- Rheumatoid arthritis, ankylosing spondylitis, reactive arthritis
- What it means
- Mechanical injury
- Orthopaedic examples
- Fracture, dislocation, ligament and tendon rupture
- What it means
- Disordered chemistry or hormones
- Orthopaedic examples
- Gout, osteomalacia, Paget disease, hyperparathyroid bone disease
- What it means
- Benign or malignant tumour
- Orthopaedic examples
- Osteosarcoma, giant cell tumour, metastasis, myeloma
- What it means
- Present from birth or developmental
- Orthopaedic examples
- Developmental dysplasia of the hip, skeletal dysplasia, club foot
- What it means
- Wear and ageing
- Orthopaedic examples
- Osteoarthritis, disc degeneration, rotator cuff tendinopathy
- What it means
- No cause found, treatment-related, or non-structural
- Orthopaedic examples
- Idiopathic scoliosis, post-surgical complication, functional pain
The crucial point is that the sieve is a prompt for completeness, not a list to recite. In practice you run through the categories silently and quickly, pull out the ones that fit the clinical picture, and present a focused, prioritised differential - leading with the dangerous and the common.
A complete differential is not the same as a long one. Use the sieve to make sure you have considered every category, then present a short, prioritised list - the can't-miss diagnoses first, then the likely ones. The examiner wants to see that you thought broadly and then chose wisely.
The Anatomical (Structural) Sieve
The aetiological sieve above (VITAMIN CDEF) asks what kind of process — but the "surgical sieve" has a second, complementary axis: the anatomical (structural) sieve, which asks which structure is responsible by working through the tissue layers at the site of the problem. It is especially useful for a localised problem — a painful joint, a lump, a single region — where listing every disease category is less helpful than asking "which structure here is the culprit?".
- Orthopaedic example of pathology
- Cellulitis, sinus, ganglion, lipoma, skin malignancy over a lump
- Orthopaedic example of pathology
- Compartment syndrome, muscle tear or haematoma, myositis, soft-tissue sarcoma
- Orthopaedic example of pathology
- Tendinopathy, tendon rupture, tenosynovitis, bursitis
- Orthopaedic example of pathology
- Sprain, instability, capsulitis
- Orthopaedic example of pathology
- Fracture, osteomyelitis, primary or metastatic tumour, metabolic bone disease
- Orthopaedic example of pathology
- Osteoarthritis, septic or inflammatory arthritis, crystal arthropathy, loose body
- Orthopaedic example of pathology
- Entrapment, neuroma, referred radicular pain
- Orthopaedic example of pathology
- Ischaemia, aneurysm, deep vein thrombosis, vascular malformation
- Orthopaedic example of pathology
- Pain referred from a proximal joint or the spine (for example hip pathology presenting as knee pain)
In practice the two sieves are used together: the anatomical sieve localises the problem to a structure, and the aetiological (VITAMIN) sieve then asks what process is affecting it — a quick way to generate a complete yet focused differential, and a classic recovery move when a "causes of a lump / painful joint" viva question stalls.
Dual-Process Theory: How Clinicians Actually Think
Modern theory describes two systems of thinking that work together:
- System 1 (intuitive)
- Fast, automatic, effortless
- System 2 (analytical)
- Slow, deliberate, effortful
- System 1 (intuitive)
- Pattern recognition - matches to remembered examples
- System 2 (analytical)
- Step-by-step reasoning through possibilities
- System 1 (intuitive)
- Familiar, classic presentations in experienced hands
- System 2 (analytical)
- Unfamiliar, complex or atypical presentations
- System 1 (intuitive)
- Prone to cognitive bias and snap errors
- System 2 (analytical)
- Limited by working memory; tiring and time-consuming
- System 1 (intuitive)
- This is the answer the sieve cross-checks
- System 2 (analytical)
- This is the system the sieve belongs to
Neither system is inherently better - the evidence is that experts use both, and the safest clinicians deliberately switch from intuition to analysis when something does not fit. This switch is sometimes called executive override: you take a brief time-out to ask "what else could this be?" and run the sieve. The reverse danger is when fast intuition overrides good analysis - for example ignoring a clinical decision rule because "it just looks like a sprain".
Importantly, research shows that simply teaching clinicians to "slow down and avoid bias" does not reliably reduce errors on its own. What helps more is better organised knowledge and practice with feedback, so that both your pattern recognition and your analytical checks improve. The sieve is most useful as a habit that prompts the analytical cross-check, combined with genuine knowledge of the conditions in each category.
Cognitive Biases and Diagnostic Error
Diagnostic error is common and is usually a failure of reasoning, not a failure of knowledge. A handful of named biases account for most of it, and examiners like you to be able to name them and say how to mitigate each.
- What it is
- Fixating on the first piece of information and failing to adjust
- How to guard against it
- Deliberately re-weigh later findings; ask 'what does not fit?'
- What it is
- Accepting a diagnosis before it is fully verified - the commonest error
- How to guard against it
- Run the sieve; ask 'what else could this be?' before committing
- What it is
- Favouring a diagnosis that comes to mind easily (recent or memorable)
- How to guard against it
- Consider base rates - what is actually common in this patient?
- What it is
- Seeking evidence that fits your hunch and ignoring the rest
- How to guard against it
- Actively look for evidence against your leading diagnosis
- What it is
- Inheriting a previous label and carrying it on unchecked
- How to guard against it
- Re-take the history yourself; re-examine the assumptions
- What it is
- Being swayed by how the problem is presented to you
- How to guard against it
- Re-frame neutrally; restate the problem in your own words
- What it is
- Over-trusting your own judgement and skipping the check
- How to guard against it
- Use checklists and the sieve; seek a second opinion when unsure
The practical defence against all of these is the same: a deliberate System 2 cross-check using a structured tool. The surgical sieve is one such tool; checklists, "diagnostic time-outs", and actively asking "what is the worst this could be, and have I excluded it?" are others.
Causes of Error in Clinical Reasoning: Bias, Knowledge and Dual Process
- Clinical reasoning follows a dual-process model: fast intuitive Type 1 thinking and slow analytical Type 2 thinking
- Both Type 1 and Type 2 reasoning can produce diagnostic errors
- Educational strategies aimed only at teaching clinicians to recognise their biases are largely ineffective at reducing errors
- Strategies that reorganise and strengthen knowledge produce small but consistent reductions in error
Cognitive Debiasing: Origins of Bias and the Theory of Debiasing
- Diagnostic failure is strongly influenced by the psychology of the decision-maker, framed by dual-process theory
- Most cognitive and affective biases arise in the fast, intuitive Type 1 processes that dominate everyday decisions
- Biases come from two sources: innate, evolutionary shortcuts and biases acquired through training and environment
- Fatigue, sleep deprivation and cognitive overload increase the risk of biased decisions; debiasing requires a deliberate switch from intuitive to analytical thinking
Bayesian Reasoning: Weighting the Differential
The sieve generates the list; Bayesian reasoning decides how to weight it. Every diagnosis starts with a pre-test probability (how likely it is before testing, driven by prevalence and the clinical picture), and each finding or test result updates that probability up or down toward a post-test probability. This is the quantitative complement to the qualitative sieve.
- What it means / how to use it
- Likelihood of the diagnosis before testing (prevalence plus the clinical picture); it sets the starting point for everything that follows
- What it means / how to use it
- A highly SENSITIVE test, when NEGATIVE, helps rule a diagnosis OUT
- What it means / how to use it
- A highly SPECIFIC test, when POSITIVE, helps rule a diagnosis IN
- What it means / how to use it
- How much a result shifts probability: an LR greater than 10 (or less than 0.1) moves it a large, often decision-changing amount; an LR near 1 is uninformative
- What it means / how to use it
- Below the test threshold the probability is too low to test; above the treatment threshold it is high enough to treat without further tests; testing is worthwhile only in between
This explains why a hot joint with a high pre-test probability of sepsis is aspirated and often treated empirically, whereas the same test is not ordered when the pre-test probability is trivial. The exam point: the sieve makes the differential complete, but prioritising it requires probability — lead with what is both dangerous and, given this patient's pre-test probability, actually likely.
Using the Sieve Well (and Its Limits)
A sieve is only as good as the way you use it. Used badly it becomes a mechanical recital; used well it is a fast, silent safety check that produces a focused differential.
Filter the categories through the clinical picture. For a hot, swollen joint the sieve points you to infection (septic arthritis), crystals (gout), trauma (haemarthrosis) and inflammatory flare - not to congenital causes. Lead with what is dangerous and common.
Always front-load infection, malignancy, fracture and vascular compromise where relevant. Demonstrating safety is worth more than an exhaustive list, and it protects the patient.
Running through every category mechanically, including irrelevant ones, wastes time and sounds rote. Use the sieve internally to be complete, then present a prioritised answer.
The framework cannot substitute for knowing the actual diseases. A confident "neoplastic" category is useless if you cannot name the relevant tumours. Structure plus knowledge is what scores.
A structured differential should always keep septic arthritis at the top of an acute monoarthritis until it is excluded, because a missed joint infection destroys cartilage within days. The sieve is there to ensure you also consider gout, haemarthrosis and an inflammatory flare - but never to demote the can't-miss diagnosis. Aspirate the joint if in doubt.
Clinical Relevance
The surgical sieve and the reasoning behind it run through every part of orthopaedic practice and assessment. In clinical and viva examinations, a question that asks for "the causes of" or "your differential" is an explicit invitation to use a sieve - and a structured, safety-first answer scores far better than a scattergun list. In the emergency and on-call setting, where you are tired and busy, the deliberate analytical cross-check is exactly what stops a fracture, a tumour or a joint infection being missed. In everyday clinic, the sieve keeps rare-but-serious diagnoses on the radar when a patient does not fit the usual pattern. Knowing how to build a complete differential, how your own mind reasons, and which biases catch clinicians out is core basic-science material - and it is the habit that, more than any single fact, keeps patients safe.
Guidelines, Registries and Global Practice
- Diagnostic error is a recognised global patient-safety priority: bodies such as the WHO and national patient-safety agencies highlight diagnostic safety as a major source of avoidable harm, and structured reasoning is a core mitigation across all health systems.
- Surgical-style sieves are taught worldwide under various mnemonics (VITAMIN CDEF, VINDICATE, and others). They cover the same categories of disease; candidates should use whichever they recall reliably under pressure - examiners reward the structure, not a particular acronym.
- Dual-process theory and cognitive debiasing are part of medical-education curricula internationally (for example in medical-school clinical-reasoning courses and postgraduate training), reflecting consensus that reasoning skills are teachable and examinable, not just innate.
- The consistent message across settings: a structured differential plus genuine knowledge plus feedback on missed cases is what reduces diagnostic error - not exhortation to "be careful". The surgical sieve is the practical, examinable expression of that principle.
Memory aids
VITAMIN CDEFThe Surgical Sieve (Categories of Disease)
Hook:VITAMIN CDEF - take your vitamins and run through every category so nothing is missed.
VINDICATEAn Alternative Sieve
Hook:VINDICATE - a second sieve that covers the same ground; use whichever you remember under pressure.
A PADThe Errors That Catch You Out
Hook:A PAD of bad habits - Anchoring, Premature closure, Availability, Diagnostic momentum - the four reasoning traps the sieve protects against.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you a plain radiograph with a lytic lesion in the proximal tibia of a young adult and asks for your differential diagnosis.”
“The examiner asks: 'A junior repeatedly anchors on the obvious injury and misses the second one. How do you think about clinical reasoning, and how do you avoid diagnostic error?'”
The Sieve (Categories)
- VITAMIN CDEF or VINDICATE - cover the same ground
- Vascular, Infective, Inflammatory/autoimmune, Traumatic
- Metabolic/Endocrine, Idiopathic/Iatrogenic, Neoplastic
- Congenital, Degenerative, Functional
How the Mind Reasons
- System 1: fast, intuitive pattern recognition
- System 2: slow, analytical - where the sieve belongs
- Safe clinician uses both and switches when things do not fit
- Executive override: deliberate time-out to re-think
The Biases (Why Diagnoses Are Missed)
- Anchoring: stuck on the first impression
- Premature closure: stopping too early (commonest)
- Availability: favouring a recently seen diagnosis
- Confirmation, diagnostic momentum, framing, overconfidence
Viva Technique
- Name the framework first - structure scores marks
- Lead with can't-miss diagnoses: infection, malignancy, fracture, vascular
- Tailor the sieve to the presentation; do not recite it all
- Structure plus real knowledge - the sieve is not a substitute for facts
Evidence: Does a Diagnostic Aid Help?
Diagnostic Aids: The Surgical Sieve Revisited
- Study of 48 third-year medical students comparing two diagnostic aids - the surgical sieve and a hand-held diagnostic wheel - for generating differentials
- Both diagnostic aids prompted students to generate a greater number of diagnoses
- There was no significant difference in effect between the two aids
- Diagnostic errors are well documented, supporting the early teaching of structured diagnostic frameworks
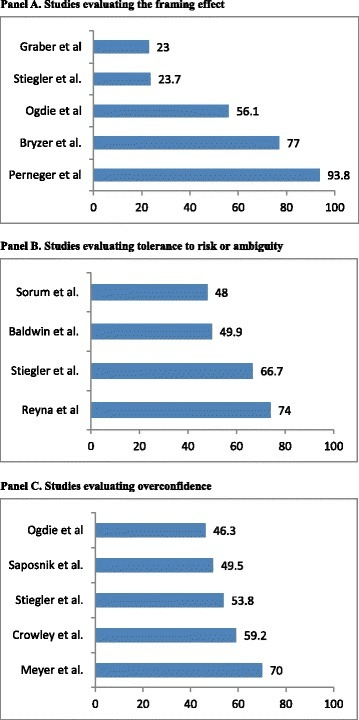
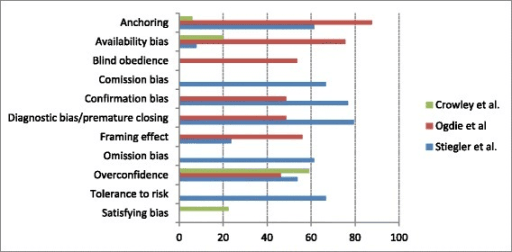
The systematic-review data shown in the imaging section reinforce the same point from the other direction: cognitive biases such as anchoring, availability, confirmation bias, premature closure and overconfidence are common and measurable across medical decision-making. A deliberate structured approach is the rational countermeasure - it forces the analytical, System 2 step that these biases bypass.