Antiresorptive or antiangiogenic therapy | Exposed bone greater than 8 weeks | No prior jaw radiation | Extraction is the common trigger | Prevention beats cure
- Definition: exposed or probeable necrotic bone in the maxillofacial region persisting greater than 8 weeks in a patient with current or previous antiresorptive (bisphosphonate or denosumab) or antiangiogenic therapy, and no history of head and neck radiation
- Risk gradient: intravenous oncology-dose zoledronic acid or denosumab (120 mg monthly) carries the highest risk; oral bisphosphonates for osteoporosis carry very low risk (less than 1 in 10,000 to 1 in 100,000 patient-years)
- Extraction is the classic trigger: the majority of cases follow dental extraction or other invasive procedures in the high-risk group; spontaneous cases occur but are less common
- Staging drives management: stage 1 is usually observation and oral care; stage 2 adds infection control; stage 3 requires surgical resection for cure
- Prevention is everything: dental review and any necessary extractions or periodontal treatment BEFORE starting high-risk antiresorptive or antiangiogenic therapy in cancer patients reduces incidence dramatically
- “When a patient on zoledronate or denosumab needs an extraction, the safest window is before the first dose if possible; if already on therapy, primary closure, antibiotic cover, and chlorhexidine are used but risk is never zero
- “A non-healing extraction socket with exposed bone at 8 weeks in an oncology patient on antiresorptives is MRONJ until proven otherwise - do not assume osteomyelitis or metastasis first
- “CBCT or panoramic radiograph is first line; look for sequestra, moth-eaten lysis, sclerosis, and periosteal reaction; advanced imaging (MRI, bone scan) if extent unclear or to exclude other pathology
- “Drug holiday before extraction is controversial and not supported by strong evidence for MRONJ prevention; the AAOMS position papers emphasise individual risk-benefit rather than routine cessation
Exposed bone or a fistula that probes to bone in the maxillofacial region for greater than 8 weeks, current or previous antiresorptive or antiangiogenic therapy, and no jaw radiation history. This is the AAOMS working definition that examiners expect verbatim.
Oncology-dose intravenous zoledronic acid (4 mg monthly) and denosumab (120 mg monthly) carry by far the highest risk. Oral bisphosphonates for osteoporosis have a very low absolute risk. Duration of therapy and cumulative dose matter.
The majority of MRONJ cases follow dental extraction, implant placement, or periodontal surgery in high-risk patients. Prevention (dental optimisation before therapy) is far more effective than any treatment after the bone is exposed.
Pathologic fracture, extraoral fistula, or osteolysis extending to the inferior border or beyond requires resection (marginal or segmental mandibulectomy) with appropriate reconstruction. Conservative measures will not heal stage 3 disease.
Overview
Medication-related osteonecrosis of the jaw (MRONJ) is a rare but serious complication of potent antiresorptive therapy (nitrogen-containing bisphosphonates and denosumab) and certain antiangiogenic agents. It is defined by exposed or probeable necrotic bone in the maxillofacial region that persists for greater than 8 weeks in a patient with relevant drug exposure and without prior jaw radiotherapy. The condition was first recognised with intravenous bisphosphonates used in oncology (zoledronic acid, pamidronate) and later with denosumab; it also occurs, at much lower rates, with oral bisphosphonates for osteoporosis and with some targeted cancer therapies.
The clinical burden falls almost entirely on patients receiving high-dose intravenous or subcutaneous antiresorptives for skeletal metastases or multiple myeloma. In this group the incidence after dental extraction can reach several percent; in osteoporosis patients on oral agents the absolute risk is orders of magnitude lower (often cited less than 1 in 10,000 patient-years). The posterior mandible is the most common site because of its high bone turnover, thin overlying mucosa, and relatively terminal blood supply.
For the exam the essential threads are: the precise definition and staging (AAOMS), why antiresorptives cause it (impaired osteoclast-mediated repair after trauma), the central role of dental extraction as trigger, the radiographic signs that distinguish it from metastasis or simple osteomyelitis, and the management ladder from prevention through conservative care to resection in advanced disease. Drug holidays before extraction remain controversial and are not a substitute for pre-therapy dental optimisation.
Principles of MRONJ
MRONJ is fundamentally a failure of bone repair after trauma in the setting of osteoclast suppression. Antiresorptives (amino-bisphosphonates via FPPS inhibition in the mevalonate pathway; denosumab via RANKL blockade) drastically reduce osteoclast number and activity. In most of the skeleton this is therapeutic (reduced fracture risk), but the jaws experience repeated low-level trauma from mastication, periodontal disease, and especially dental procedures. When an extraction socket or mucosal breach occurs, the normal sequence of inflammation followed by osteoclast-mediated resorption of damaged bone and osteoblast-driven new bone formation is interrupted. The result is persistent devitalised bone that becomes exposed when overlying soft tissue cannot heal over it.
Additional amplifying factors include antiangiogenic effects (reduced blood supply for healing), secondary bacterial colonisation (Actinomyces and oral flora), and in cancer patients the cumulative insults of chemotherapy, steroids, malnutrition, and the underlying malignancy. The posterior mandible is disproportionately affected because of high baseline turnover in alveolar bone, thin mucosa, and relatively limited collateral circulation once the inferior alveolar artery is compromised.
The clinical corollary is that prevention (optimising the dentition before the first high-risk dose) is vastly more effective than any treatment after exposure has occurred. Once necrotic bone is exposed, management is staged and largely supportive until sequestra separate or surgical resection is required for complications.
Anatomy and Pathophysiology
The jaws (particularly the mandible) are uniquely vulnerable. The mandible has a high rate of bone remodeling, especially in the alveolar process that supports teeth. When teeth are extracted the socket must heal by a coordinated sequence of inflammation, granulation, woven bone formation, and remodeling. Potent antiresorptives suppress osteoclast recruitment and function, so the remodeling phase stalls. The result is devitalised bone that becomes exposed when the thin mucosa breaks down or after surgical trauma.
Key anatomic points:
- Mandible is affected far more often than maxilla (roughly 2 to 3:1 or higher in most series).
- Posterior mandible (molar and premolar regions) is the classic site; the thin mucosa over the mylohyoid ridge and the limited collateral circulation make it susceptible.
- The inferior alveolar nerve can be involved, producing numbness or paraesthesia when necrosis reaches the canal.
- Maxillary cases are more likely to present with oro-antral fistula or sinusitis because of the thin bone and proximity to the antrum.
Pathophysiology is multifactorial:
- Osteoclast inhibition (via farnesyl pyrophosphate synthase blockade for amino-bisphosphonates; RANKL neutralisation for denosumab) prevents the normal repair of micro-damage and the resorption of necrotic bone.
- Antiangiogenic effects (seen with some bisphosphonates and with agents such as bevacizumab) reduce vascularity and healing capacity.
- Local trauma (extraction, ill-fitting dentures, periodontal surgery) creates a wound that cannot epithelialise over the non-viable bone.
- Secondary infection (Actinomyces and mixed oral flora are frequently cultured) perpetuates inflammation and bone death.
- In cancer patients, the underlying disease, chemotherapy, steroids, and poor nutrition compound the problem.
Spontaneous MRONJ (no obvious dental trigger) occurs, especially in the mylohyoid region or torus, but extraction or other invasive procedures remain the dominant precipitant in reported series.
Classification and Staging
The AAOMS staging system (updated 2014 and with further clarification in 2022) is the international standard used in examinations and in multidisciplinary discussion. It is clinical-radiographic and directly guides treatment.
- Clinical Features
- No exposed bone or fistula, but symptoms (pain, tooth mobility, radiographic sclerosis or lysis) or non-specific signs that suggest early disease
- Initial Management Approach
- Optimise oral hygiene, chlorhexidine rinses, address infection, close follow-up; consider drug holiday only if oncologist agrees it does not compromise skeletal protection
- Clinical Features
- Exposed bone or a fistula that probes to bone, present greater than 8 weeks, asymptomatic, no clinical signs of infection
- Initial Management Approach
- Conservative: 0.12 percent chlorhexidine rinses, oral hygiene instruction, avoid further trauma, review every 2 to 3 months; antibiotics only if infection develops
- Clinical Features
- Exposed or probeable bone with pain and clinical infection (erythema, swelling, purulent discharge, or sinus tract)
- Initial Management Approach
- Infection control: culture-directed or empirical oral antibiotics (amoxicillin-clavulanate or clindamycin), antiseptic rinses, pain control, limited superficial debridement of mobile sequestra only
- Clinical Features
- Exposed bone plus one or more of: pathologic fracture, extraoral fistula, osteolysis extending to the inferior border or ramus, or extensive necrosis
- Initial Management Approach
- Surgical: segmental or marginal resection of necrotic bone with margins into bleeding viable bone; reconstruction with plate or free flap as indicated; antibiotics and supportive care
Stage is dynamic. A patient can move from stage 1 to stage 2 with secondary infection, or from stage 2 to stage 1 after successful infection control and sequestration of a small fragment. Document stage at every visit and photograph exposed bone when possible.
Clinical Presentation
History
- Current or previous bisphosphonate (zoledronate, alendronate, risedronate, pamidronate, ibandronate) or denosumab, or antiangiogenic therapy (bevacizumab, sunitinib, etc.).
- Oncology indication (bone metastases, multiple myeloma, giant cell tumour) versus osteoporosis or Paget disease.
- Recent dental extraction, implant, periodontal surgery, or denture trauma - timing relative to drug exposure is critical.
- Pain, swelling, bad taste, halitosis, discharge, or a non-healing socket that has persisted beyond the expected 4 to 6 weeks.
- Numbness of the lower lip or chin (inferior alveolar nerve involvement).
Examination
- Exposed bone in the oral cavity, often with a yellow-white or grey sequestrum; the surrounding mucosa may be erythematous or rolled.
- A fistula (intraoral or extraoral) that can be probed to bone or to a sequestrum.
- Signs of infection: pus, swelling, trismus, lymphadenopathy.
- Pathologic fracture: mobile mandible segments, malocclusion, pain on loading.
- Extraoral cutaneous fistula or exposed bone through skin in advanced cases.
- Dental status: caries, periodontal pocketing, ill-fitting prostheses.
Always examine both jaws, the full dentition, and the neck. Bilateral or multifocal disease occurs, especially in high-dose intravenous therapy.
Investigations
Imaging
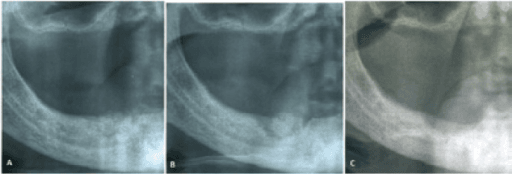
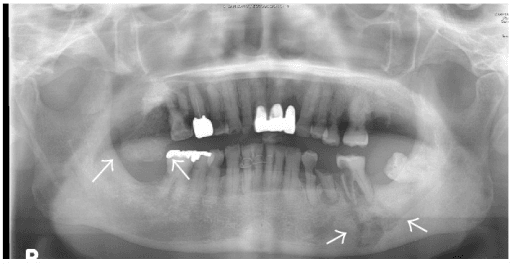
- Panoramic radiograph (orthopantomogram) is the first-line study: look for poorly defined radiolucencies, sclerotic zones, sequestra (dense fragments separated by lucent rims), moth-eaten destruction, and periosteal reaction.
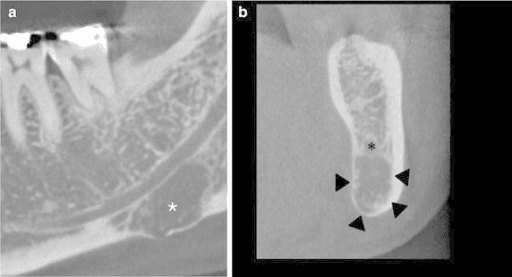
- Cone-beam CT (CBCT) or conventional CT provides better three-dimensional assessment of extent, cortical perforation, involvement of the inferior alveolar canal, and proximity to the maxillary sinus.
- MRI is useful when soft-tissue extent or marrow involvement needs clarification, or when ruling out metastatic disease or osteomyelitis.
- Bone scintigraphy or PET can show increased uptake but is non-specific; useful in selected cases to assess whole-skeleton burden or occult sites.
Laboratory
- No specific blood test diagnoses MRONJ. Check full blood count, inflammatory markers (CRP, ESR), and albumin/pre-albumin if nutrition is a concern.
- In oncology patients, coordinate with the medical oncology team regarding renal function (especially before any further zoledronate) and calcium (hypocalcaemia risk with denosumab).
- Microbiology: swab or biopsy of exposed bone or pus for culture and sensitivity; Actinomyces is frequently isolated but its role as primary pathogen versus coloniser is debated.
Biopsy / histology
- Not required for every case. When performed (to exclude metastasis or primary malignancy), histology shows necrotic bone with empty lacunae, bacterial colonisation, and minimal inflammatory infiltrate in pure MRONJ; vital bone at the resection margin confirms adequacy.
- Always send tissue in stage 3 surgical cases.
Differential diagnosis
- Metastatic carcinoma (breast, prostate, lung, myeloma) - can coexist with MRONJ.
- Osteoradionecrosis (if radiation history).
- Chronic osteomyelitis (no drug history).
- Primary bone tumours or osteonecrosis from other causes (rare).
Management
Prevention (the only intervention with level-1 impact)
- All patients due to start high-risk intravenous or subcutaneous antiresorptive or antiangiogenic therapy for cancer should have a dental review before the first dose.
- Extract non-restorable teeth and complete periodontal therapy; allow 4 to 6 weeks of mucosal healing before commencing the drug when clinically safe.
- For patients already on therapy who require extraction, primary closure, perioperative antibiotics, and chlorhexidine are used; risk cannot be eliminated.
- Patient education: report any non-healing socket, pain, or exposed bone immediately.
Stage-directed treatment
- Stage 0 and 1: conservative. Chlorhexidine 0.12 percent rinses twice daily, meticulous oral hygiene, regular review. No elective surgery. Mobile sequestra may be removed if they are easily accessed without further trauma.
- Stage 2: add infection control. Empirical or culture-directed oral antibiotics (amoxicillin-clavulanate 875/125 mg twice daily or clindamycin 300 mg three times daily for 7 to 14 days), antiseptic rinses, pain management, and limited debridement of loose bone only. Most cases stabilise; some progress.
- Stage 3: surgical resection. Under general anaesthesia, resect all necrotic bone back to bleeding, viable bone margins (marginal mandibulectomy if inferior border intact; segmental if not). Stabilise with reconstruction plate; consider free fibula or scapula flap for large defects in fit patients. Continue antibiotics and chlorhexidine postoperatively. Long-term follow-up is mandatory.
Drug holiday
- The 2014 and later AAOMS guidance does not recommend routine drug interruption solely for MRONJ prevention in patients who need ongoing skeletal protection. Individualised discussion with the oncologist is required. For osteoporosis patients on long-term oral therapy, a drug holiday may be considered for other reasons (atypical fracture risk) but is not proven to reduce MRONJ.
Supportive measures
- Nutrition, smoking cessation, glycaemic control in diabetics, and management of comorbidities improve healing potential.
- Hyperbaric oxygen is not routinely recommended by AAOMS for MRONJ (unlike ORN); evidence is weak.
Bisphosphonate versus Denosumab: Pharmacology and Why It Changes Timing
Both drugs suppress osteoclasts and both cause MRONJ, but they do so by different mechanisms with very different kinetics - and that difference is the basic-science reason a "drug holiday" behaves so differently between them.
- Nitrogen-containing bisphosphonate
- Inhibits farnesyl pyrophosphate synthase in the osteoclast (mevalonate pathway)
- Denosumab
- Monoclonal antibody that neutralises RANKL, preventing osteoclast formation and activation
- Nitrogen-containing bisphosphonate
- YES - binds hydroxyapatite and is incorporated into the skeleton
- Denosumab
- NO - circulates and is not deposited in bone
- Nitrogen-containing bisphosphonate
- Very long skeletal half-life (years) - effect PERSISTS long after stopping
- Denosumab
- Short circulating half-life (about 26 days); bone turnover RECOVERS within months of stopping
- Nitrogen-containing bisphosphonate
- A short holiday does little - the drug lingers in bone, so MRONJ risk persists
- Denosumab
- Effect is reversible, so timing invasive dentistry near the end of the dosing interval (the trough) is rational
A further denosumab-specific caveat is the rebound phenomenon: stopping denosumab without transitioning to a bisphosphonate causes rapid loss of the accrued bone density and a risk of multiple rebound vertebral fractures - so cessation decisions are never the dentist's alone and must involve the prescribing physician.
The key pharmacology: bisphosphonates are incorporated into bone with a half-life of years, so their effect (and MRONJ risk) persists long after stopping - which is why a short holiday is largely ineffective. Denosumab is not bone-bound, has a roughly 26-day half-life and its effect reverses within months, so invasive dental work is best timed towards the trough of the dosing interval. Never stop denosumab without a bisphosphonate bridge because of rebound fractures.
Complications
Local
- Chronic pain, recurrent infection, and halitosis.
- Pathologic fracture of the mandible (most feared stage 3 event).
- Oro-cutaneous fistula, oro-antral communication, maxillary sinusitis.
- Inferior alveolar or lingual nerve injury (from disease or surgery).
- Loss of teeth, denture intolerance, and severe functional impairment.
Systemic
- In frail oncology patients, uncontrolled jaw sepsis can contribute to systemic inflammatory response or delay cancer treatment.
- Malnutrition from pain on eating.
Treatment-related
- Surgical complications: plate exposure, flap failure, further necrosis at margins, donor-site morbidity.
- Antibiotic-associated diarrhoea or resistance with prolonged courses.
- Psychological impact of facial disfigurement or prolonged illness in patients already facing cancer.
Late failure
- Recurrence of exposed bone at the resection margin or at distant sites if the underlying drug exposure and risk factors continue.
MRONJ versus Osteoradionecrosis (ORN)
The topic's definition deliberately excludes prior jaw radiation - because necrotic exposed jaw bone in an irradiated patient is osteoradionecrosis (ORN), a separate entity that looks similar but differs in cause, mechanism, and (critically) the role of hyperbaric oxygen.
- MRONJ
- Antiresorptive (bisphosphonate or denosumab) or antiangiogenic drug; NO radiation
- Osteoradionecrosis (ORN)
- Head and neck radiotherapy (classically over 60 Gy to the field)
- MRONJ
- Osteoclast suppression - failure to repair and remodel injured bone
- Osteoradionecrosis (ORN)
- Hypovascular-hypocellular-hypoxic tissue (Marx 3-H theory); also a radiation-induced fibro-atrophic process
- MRONJ
- Dental extraction or invasive procedure (or spontaneous)
- Osteoradionecrosis (ORN)
- Dental extraction in the irradiated field, or spontaneous
- MRONJ
- NOT routinely recommended (weak evidence)
- Osteoradionecrosis (ORN)
- Has an established role and evidence base (Marx protocol)
- MRONJ
- Antiseptic and antibiotic cover, staged surgery
- Osteoradionecrosis (ORN)
- Pentoxifylline plus tocopherol (PENTOCLO) targeting the fibro-atrophic process
Because the two are defined to be mutually exclusive, the single discriminating question is the radiation history: an antiresorptive patient with no jaw radiation has MRONJ; an irradiated patient has ORN even if also on a bisphosphonate. The distinction matters because hyperbaric oxygen helps ORN but is not a standard MRONJ treatment.
Exposed necrotic jaw bone after radiotherapy = osteoradionecrosis (Marx hypovascular-hypocellular-hypoxic / radiation-induced fibro-atrophy); after an antiresorptive or antiangiogenic with no radiation = MRONJ. They look alike and share the extraction trigger and posterior-mandible predilection, but hyperbaric oxygen has a role in ORN and is NOT routinely recommended for MRONJ - a classic examiner discriminator.
Clinical Relevance
MRONJ sits at the intersection of oncology, oral surgery, and orthopaedic/metabolic bone medicine. Every patient who starts a high-potency antiresorptive for skeletal metastases or myeloma should be viewed as having a lifelong risk to the jaws. The orthopaedic surgeon or endocrinologist who prescribes these agents must either arrange pre-treatment dental clearance or document that the patient has been counselled and that dental review has occurred or is planned.
In the exam, the topic tests understanding of:
- Basic bone biology (osteoclast function, remodeling, angiogenesis).
- Risk stratification by drug, dose, route, and indication.
- Practical prevention rather than heroic salvage.
- Clear staging language that communicates urgency to the maxillofacial team.
- The limits of conservative care and the indications for resection.
The same principles apply to denosumab as to bisphosphonates; the RANKL inhibitor produces a comparable, if not higher, incidence of MRONJ in oncology doses. As more patients receive these therapies for longer periods and for additional indications (giant cell tumour, osteoporosis with high fracture risk), the absolute number of MRONJ cases will remain clinically relevant even if the per-patient risk is managed.
Guidelines, Registries and Global Practice
-
AAOMS position papers (2007, 2009, 2014, 2022 updates) remain the most widely referenced international guidance. They established the current definition, the four-stage system, and the emphasis on prevention before high-risk therapy. The 2014 paper broadened the term from BRONJ to MRONJ to include denosumab and antiangiogenics.
-
European / international consensus (e.g. from ESMO, MASCC, and national oral medicine societies) aligns closely with AAOMS on staging and the central role of pre-treatment dental assessment for patients starting oncology-dose antiresorptives. Some European guidelines place slightly more weight on drug holidays in selected low-risk scenarios, but evidence remains limited.
-
Denosumab-specific data: oncology-dose denosumab (120 mg monthly) carries a comparable or slightly higher MRONJ incidence than zoledronic acid in head-to-head trials and real-world cohorts. The same prevention and staging principles apply.
-
Registry and cohort evidence: large oncology cohorts and systematic reviews (including the 20-year single-centre series and extraction-risk meta-analyses) confirm that dental extraction is the dominant modifiable risk factor and that structured prevention programs reduce incidence. Absolute risk in osteoporosis patients on oral agents remains very low worldwide.
-
Global practice variation: access to specialist maxillofacial care, CBCT, and reconstructive microsurgery varies. In resource-limited settings, emphasis remains on prevention and conservative infection control; advanced stage 3 disease may be managed with local debridement and antibiotics rather than major resection. No country-specific billing codes are used in guidance.
-
Key practical message: wherever a patient is started on high-potency antiresorptive therapy for cancer, dental review before the first dose is a quality and safety standard across AAOMS, European, and Asia-Pacific recommendations.
Memory aids
SANEMRONJ Staging (AAOMS)
Hook:SANE staging: from subtle symptoms (0) to asymptomatic exposed (1), necrotic infected (2), and extensive surgical (3).
IV DENTHigh-Risk Drugs and Patients
Hook:IV DENT: Intravenous high-dose, Very long use, Dental trauma, Existing infection, No radiation, Thrombosis/angiogenic drugs.
CLEANPrevention Before High-Risk Therapy
Hook:CLEAN mouth before you start: Complete assessment, Limit extractions to pre-therapy, Educate, Avoid new surgery on therapy, Never dismiss even low-risk patients.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old woman with metastatic breast cancer on monthly zoledronic acid 4 mg for 18 months requires extraction of three non-restorable lower molars. The oncologist asks how you will manage the risk of MRONJ.”
“A 68-year-old man with myeloma on denosumab 120 mg monthly for 14 months presents with a 10-week history of exposed bone in the left posterior mandible after extraction, now with pain, swelling, and a small amount of pus. Panoramic radiograph shows a 2 cm area of lysis with a sequestrum but the inferior border is intact. How do you stage and manage this?”
“A 55-year-old woman with metastatic lung cancer on zoledronic acid and bevacizumab presents with sudden pain and a mobile mandible after a trivial fall. Examination shows a cutaneous fistula with exposed bone and malocclusion. Radiographs confirm a pathologic fracture through an area of osteonecrosis. What is your approach?”
Evidence
AAOMS Position Paper on Medication-Related Osteonecrosis of the Jaw (2014 Update)
- Updated consensus definition: exposed bone or probeable bone greater than 8 weeks in a patient with antiresorptive or antiangiogenic exposure and no jaw radiation
- Four-stage system (0-3) that directly informs treatment; stage 3 explicitly includes pathologic fracture, extraoral fistula, and extensive osteolysis
- Risk is highest with intravenous oncology-dose bisphosphonates and denosumab; oral agents for osteoporosis carry very low absolute risk
- Dental extraction remains the most common precipitating event; prevention through pre-therapy dental optimisation is the most effective strategy
Diagnosis and Treatment of Medication-Related Osteonecrosis of the Jaws: A Cohort Study Over 20 Years
- Copenhagen ONJ Cohort: 934 MRONJ patients diagnosed 2005-2024 at a single tertiary centre
- Mean age 71.6 years, 68.4% female; commonest antiresorptive indications were osteoporosis, breast cancer, prostate cancer and multiple myeloma
- Conservative management in 18.1% versus surgical intervention in 81.9% of patients
- Tooth removal was the most frequent triggering event (52.9%); demographics and concomitant steroid/immunosuppressant/antiangiogenic use differed across antiresorptive-dose groups
Does Tooth Extraction Increase the Risk of MRONJ in Oncologic Patients? A Systematic Review and Meta-Analysis
- Systematic review and meta-analysis of 7 studies (497 oncology patients) of MRONJ after tooth extraction
- Pooled proportion of MRONJ after extraction was 27.6% (95% CI 16.0-43.3%) in this high-risk oncology population
- No significant association with female sex or chemotherapy; MRONJ patients had a significantly longer duration of bone-modifying-agent therapy (pooled mean difference 8.38 months, 95% CI 2.44-14.32)
- Key nuance: the evidence does NOT support extraction as an isolated, uniformly avoidable trigger - local infection, inflammatory dental disease, extraction timing and cumulative drug exposure appear more consistently associated with risk